What you’ll learn in this article…
- Nearly 66,000 qualified nursing applicants were turned away in one year, largely because faculty shortages left no one to teach them.
- Burnout in nurse educators clusters around three dimensions: emotional exhaustion, depersonalization, and reduced personal accomplishment.
- Organizational interventions such as peer mentorship, competitive pay, and AI-supported workload reduction outperform individual coping strategies alone.
- Validated tools like the Maslach Burnout Inventory let educators track their burnout trajectory before symptoms become career threatening.
You can frame the nursing shortage as a pipeline problem: too few seats, too many applicants. Or you can trace it back to the educators leaving the classroom. When the American Association of Colleges of Nursing reports that nearly 66,000 qualified nursing school applicants were turned away in a single year, the bottleneck is not just capacity. It is faculty attrition fueled by burnout, a reality the nurse educator shortage has only intensified. Recognizing the warning signs, measuring your own risk, and advocating for structural support are no longer optional. They are essential for retaining the educators who train the next generation of nurses.
Nurse Educator Burnout Is a Growing Crisis: The Numbers Behind the Problem
Nurse educator burnout is not a vague sense of job dissatisfaction. It is a measurable, documented collapse of the energy, motivation, and engagement that faculty need to teach effectively, mentor students, and sustain their careers in academic nursing.
The Burnout Rates Are Striking
Multiple national surveys paint a consistent picture. A 2022 study found that approximately 85% of nursing faculty reported experiencing burnout.1 The following year, a national survey published through Elsevier put the numbers into even sharper focus: 85.2% of nursing faculty met criteria for overall burnout, with 85.5% reporting high levels of emotional exhaustion and 84.9% reporting significant disengagement from their work.2 By 2024, a separate analysis found that 72% of nursing faculty identified burnout as a pressing concern, suggesting the problem has not resolved on its own.3
These figures are not outliers or artifacts of pandemic-era stress. They reflect a structural problem that has persisted across multiple survey cycles and shows no meaningful sign of improvement without deliberate intervention.
Vacancies and Turnover Are Compounding the Pressure
As experienced faculty burn out and leave, the positions they vacate often go unfilled for extended periods. As of 2025, the national faculty vacancy rate sits at 7.2%, representing roughly 1,588 open positions across the country.4 Of those vacancies, 80.9% are at the doctoral level, where qualified candidates are fewest and competition from clinical and research sectors is most intense. Beyond current openings, programs report needing to create approximately 150 additional positions to meet rising student demand. For a deeper look at these trends, see our overview of the nursing faculty shortage.
Every unfilled seat at the faculty table increases the workload on those who remain, which accelerates the very burnout that caused vacancies in the first place.
The Downstream Consequence: Fewer Nurses Entering the Workforce
This is where faculty burnout becomes a public health concern. In 2024, more than 80,000 qualified applicants were turned away from nursing programs, largely because programs lacked the faculty capacity to admit them.4 The American Association of Colleges of Nursing has identified the faculty shortage as a primary driver of those rejections, and a June 2026 analysis published by Daily Nurse echoes that conclusion directly, noting that faculty attrition driven by burnout and workload strain is narrowing the pipeline of future nurses.
Pay Disparity Widens the Gap
One factor accelerating faculty attrition rarely gets the attention it deserves: compensation. In 2023, the median annual wage for nursing faculty was approximately $93,958, compared to roughly $129,480 for advanced practice registered nurses in clinical settings.4 That gap of about $35,500 (27 to 30 percent less than clinical peers) makes it financially difficult for highly qualified nurses to choose or remain in academic roles. You can explore how these salary differences play out across career paths in our nurse educator salary vs nurse practitioner salary comparison. When burnout is already eroding the non-financial rewards of teaching, a pay gap of this magnitude becomes a decisive reason to leave.
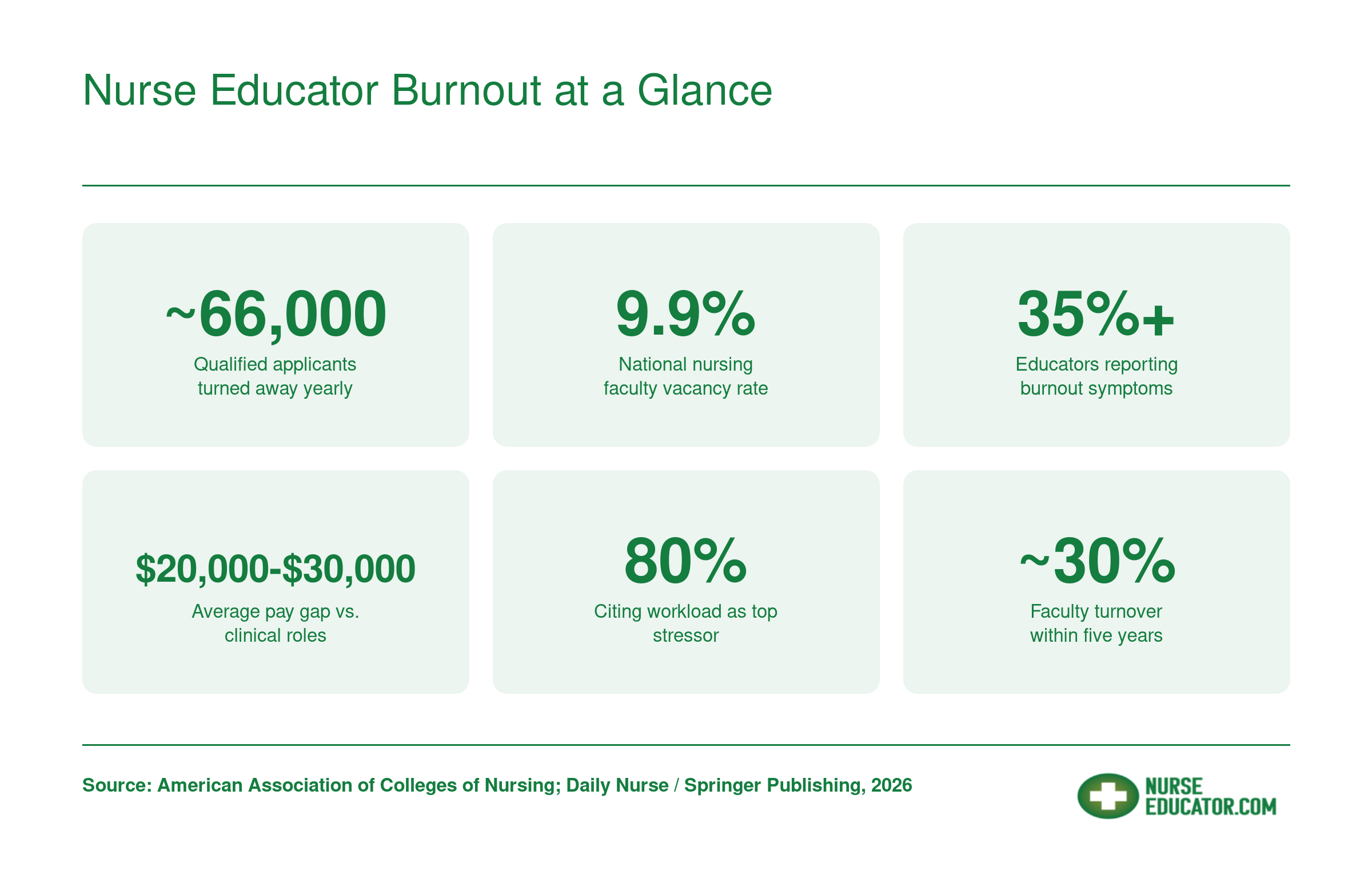
Nurse Educator Burnout at a Glance
The numbers paint a clear picture: nurse educators face unsustainable pressures that threaten both their well-being and the future nursing workforce. These figures highlight why burnout prevention must become an institutional priority.
Common Stressors Unique to Nurse Educators
Nurse educators face a constellation of stressors that bedside nurses rarely encounter, which is precisely why generic burnout advice often misses the mark. While clinical nurses grapple with patient acuity and staffing ratios, faculty members navigate an entirely different landscape of pressures that demand recognition and targeted solutions.
The Accreditation Compliance Burden
Few responsibilities weigh as heavily on nurse educators as accreditation preparation and maintenance. Faculty must continuously document student learning outcomes, maintain detailed records of clinical competency evaluations, and produce evidence of nursing education curriculum alignment with evolving national standards. This work happens alongside regular teaching duties, often without dedicated release time. When accreditation visits approach, the documentation demands can consume evenings and weekends for months. Unlike a challenging patient assignment that ends with a shift, accreditation pressure cycles continuously throughout an academic career.
Grading Overload and Dual Role Expectations
The sheer volume of student work requiring thoughtful feedback creates chronic time pressure. Nurse educators grade clinical evaluations, care plans, simulation debriefs, written assignments, and examinations, often for multiple sections simultaneously. Many programs also expect faculty to maintain active clinical practice to stay current, effectively requiring them to hold two demanding jobs at once. This nurse educator patient care expectation means educators often work clinical shifts on top of full teaching loads, stretching their time and energy to unsustainable levels.
Online and Hybrid Teaching Demands
The rapid shift to remote instruction during the pandemic introduced technical and pedagogical challenges that have not receded. Faculty now manage learning management systems, troubleshoot technology issues during virtual sessions, create engaging asynchronous content, and provide individualized feedback through digital platforms. These responsibilities layer onto traditional teaching rather than replacing it, since most programs have retained hybrid or flexible formats that require faculty to teach effectively in multiple modalities.
Adjunct Precarity
A significant portion of nursing education relies on adjunct faculty who face distinct stressors:
- Low pay: Compensation per course often falls well below what the same hours would yield in clinical practice.
- No benefits: Health insurance, retirement contributions, and paid leave are typically unavailable.
- Semester uncertainty: Contracts renewed term by term make financial planning difficult and career stability elusive.
This precarity creates chronic anxiety that compounds all other stressors. If you are weighing these trade-offs, understanding why nurses become nurse educators can help you decide whether the mission outweighs the challenges.
Simulation Lab and Clinical Currency Pressures
Coordinating simulation experiences requires faculty to master complex equipment, develop realistic scenarios, and facilitate debriefing sessions that promote critical thinking. Meanwhile, the expectation to remain clinically competent means pursuing continuing education and often maintaining certification requirements, all while teaching full course loads. The pressure to excel in both academic and clinical domains creates a unique form of role strain that bedside nurses simply do not face. Recognizing these educator-specific stressors is the first step toward developing interventions that actually work.
Questions to Ask Yourself
Recognizing the Signs of Burnout in Nurse Educators
Burnout in nurse educators typically clusters around three validated dimensions first described in the Maslach Burnout Inventory: emotional exhaustion, depersonalization, and reduced personal accomplishment. While those categories apply across helping professions, the way each one shows up in your day-to-day life as a nursing faculty member can look quite different from what a bedside nurse or corporate employee experiences. Learning to spot these signs early, in yourself and in colleagues, is one of the most practical steps you can take to protect your career and your health.
Emotional Exhaustion: More Than Just Being Tired
Emotional exhaustion is the dimension most people associate with burnout, and for good reason. In a teaching context, it often appears as:
- Dreading class prep: You once enjoyed designing case studies or updating lecture slides, but now the thought of opening your course files fills you with dread.
- Tearfulness after routine interactions: Crying after a faculty meeting or a student advising session signals that your emotional reserves are depleted, not that you are "too sensitive."
- Persistent fatigue unrelieved by weekends: A hallmark of true exhaustion is that rest does not restore you. If you return to campus on Monday feeling just as drained as you did on Friday, your body is telling you something important.
These signs can be easy to dismiss during a busy semester, especially if your colleagues seem equally worn down. Normalizing chronic exhaustion is itself a warning sign.
Depersonalization: When Students Become Problems
Depersonalization involves emotional distancing from the people you serve. For nurse educators, this dimension often surfaces as:
- Cynicism toward students: Catching yourself making dismissive comments such as "they don't even want to learn" or "this cohort is the worst yet."
- Avoidance of office hours: Canceling drop-in times, keeping your door closed, or routing all communication to email so you do not have to interact face to face.
- Referring to learners impersonally: Using phrases like "the cohort" or "those students" in a tone that strips away individual identity.
If you notice these patterns, pause before blaming the students. Depersonalization is a coping mechanism your brain uses when it can no longer sustain empathic engagement at the level teaching demands. If you are curious about how the difference between a nurse and a nurse educator shapes emotional load, understanding those distinct stressors can add useful context.
Reduced Personal Accomplishment: Losing Your "Why"
This dimension is sometimes the quietest and the most corrosive. It shows up as a creeping belief that your work does not matter, no matter how much effort you invest.
- Disengagement from scholarship: Letting research projects stall, declining conference invitations, or abandoning a manuscript mid-draft.
- Grading avoidance and procrastination: Piling up ungraded assignments not because you are busy, but because the task feels pointless.
- Feeling invisible in your institution: Believing that neither students nor administration recognize the value of what you do.
Reduced accomplishment feeds a vicious cycle: the less engaged you feel, the less energy you put in, which reinforces the sense that your contributions are insignificant. Revisiting the qualities of a good nurse educator you already possess can sometimes help reframe that internal narrative.
Compassion Fatigue: A Distinct Layer for Clinical Faculty
If you teach in clinical settings, you carry a burden that classroom-only faculty may not share. Compassion fatigue, sometimes called secondary traumatic stress, develops when you absorb the emotional weight of patient care alongside your teaching responsibilities. You may witness students making errors with real patients, manage the anxiety of clinical supervision in high-acuity units, or relive your own traumatic clinical experiences through your students' encounters.
Compassion fatigue can intensify any of the three burnout dimensions above, creating an overlay that makes recovery harder without targeted intervention. Recognizing it as a separate phenomenon, rather than lumping it in with "regular" burnout, is essential because the coping strategies differ. Peer debriefing after difficult clinical days, structured reflective practice, and clear emotional boundaries between your educator role and any residual patient care duties all play a part. Building skills in teaching emotional intelligence to nursing students can also serve as a protective practice, reinforcing your own resilience while you model it for learners.
If several of these signs feel uncomfortably familiar, take that recognition seriously. Awareness is the first requirement for change, and the next sections of this guide will walk you through validated self-assessment tools and evidence-based strategies to move from recognition to recovery.
Self-Assessment Tools: How to Measure Your Own Burnout
Validated self-assessment tools give nurse educators a concrete way to track their burnout trajectory before symptoms become career-threatening.
The following instruments have been tested in teaching and healthcare populations, offering both quantitative baselines and trends over time.1 Each differs in scope, cost, and what dimension of burnout it prioritizes. Choosing the right tool depends on whether you need to measure emotional exhaustion alone, compassion fatigue, or the full spectrum of professional quality of life.
Maslach Burnout Inventory (MBI)
The Maslach Burnout Inventory remains the most widely cited burnout measure in research and has been validated extensively in nursing and educational settings.2 The MBI Educators Survey, a variant designed specifically for teachers and faculty, consists of 22 items and assesses three dimensions: emotional exhaustion, depersonalization (cynicism toward students or colleagues), and personal accomplishment (a sense of professional efficacy).3
High scores on exhaustion and depersonalization combined with low personal accomplishment signal burnout. Exact cut-scores vary by population, so interpret your results in context rather than against a single universal threshold.4 The MBI requires purchase and licensing, which can range from individual test-taker fees to institutional subscriptions.5 This cost barrier makes it less accessible for nurse educators seeking a quick personal check-in, though many research studies and employee assistance programs administer it as part of formal wellness initiatives.
Copenhagen Burnout Inventory (CBI)
The Copenhagen Burnout Inventory offers a free, open-access alternative.1 It measures burnout across three domains: personal burnout, work-related burnout, and client-related burnout (the exhaustion tied to interactions with students or patients). The CBI uses a mean item score format rather than strict cut-points, so you track changes over time rather than comparing yourself to a diagnostic threshold.
For nurse educators balancing clinical nurse educator role responsibilities and classroom instruction, the client-related subscale captures the unique strain of mentoring students through high-stakes clinical rotations. Because the CBI is free and available in the public domain, it is practical for quarterly self-checks without needing institutional approval or budget.
Professional Quality of Life Scale (ProQOL)
The ProQOL is also free and widely used among helping professionals.1 It measures three constructs: compassion satisfaction (the fulfillment you draw from your work), burnout, and secondary traumatic stress (the emotional toll of witnessing student or patient suffering). Scores are reported as T-scores, with low, average, and high categories but no clinical diagnosis cutoff.
Nurse educators working with trauma-exposed student populations or teaching in high-acuity simulation environments may find the secondary traumatic stress subscale particularly relevant. The ProQOL helps distinguish whether your exhaustion stems from workload, from vicarious trauma, or from a loss of meaning in your nursing educator role.
How Often to Self-Assess and What the Scores Cannot Tell You
Quarterly self-assessment is a practical rhythm. It allows you to spot trends before they escalate while avoiding the fatigue of over-testing. Keep in mind that all these tools rely on self-report, which means scores reflect your awareness and willingness to acknowledge distress. Social desirability bias, denial, and cognitive fatigue can all suppress scores even when burnout is severe. Use these instruments as one data point alongside peer feedback, supervisor observations, and changes in your physical health or sleep patterns.
Related Articles
Evidence-Based Individual Strategies for Nurse Educators
Across 2022 to 2026 reviews of mindfulness-based stress reduction (MBSR) in nursing faculty and healthcare educator populations, standardized mean difference effect sizes land between -0.2 and -0.4 for emotional exhaustion, -0.2 to -0.3 for depersonalization, and 0.3 to 0.5 for personal accomplishment.1 Those are small to moderate effects, which matters: they tell you what individual strategies can realistically deliver, and where you need institutional change instead.
Ranking What Actually Works
When you sort the evidence by strength rather than popularity, a clear hierarchy emerges for nurse educators:
- MBSR (strongest individual-level evidence): Multiple controlled trials and meta-analyses in healthcare and educator samples show consistent, replicable reductions in exhaustion and gains in personal accomplishment. An 8-week structured program is the most-studied format.2
- Resilience training (solid but narrower): Recent studies report emotional exhaustion effect sizes of -0.2 to -0.3 and resilience gains of 0.4 to 0.6. Effects are stronger on coping capacity than on burnout symptoms directly.2
- Cognitive behavioral strategies: Useful for educators with rumination, perfectionism, or imposter patterns, often delivered alongside MBSR or coaching.
- Job crafting: Growing evidence in academic settings that reshaping tasks toward personally meaningful work (e.g., trading one committee seat for a curriculum innovation project) buffers exhaustion and raises engagement.
- Microboundary-setting: A 2024 DNP project with 24 nursing faculty reported statistically significant burnout improvement after a structured microboundary intervention. Small sample, but practical and low-cost.3
Microboundaries as a Daily Tactic
Microboundaries are the smallest enforceable limits you can put around your time and attention. Concrete examples that have shown up in faculty interventions:
- No-email windows before 8am and after 6pm, with an autoresponder explaining the schedule.
- Hard caps on grading time per assignment (e.g., 7 minutes per care plan), enforced with a timer.
- A one-committee-per-semester rule, declining additional service requests in writing.
- Protected deep-work blocks of 90 minutes, twice a week, on your calendar before anyone else can claim them.
Job Crafting and Role-Specific Adaptations
Job crafting looks different depending on your appointment. Tenure-track faculty have the most latitude to redirect scholarship toward topics they find energizing. If you are considering innovative teaching strategies in nursing education, that kind of curriculum redesign can double as both professional development and a burnout buffer. Clinical-only and simulation faculty often benefit from negotiating fewer clinical sites in exchange for deeper involvement in one. Adjuncts, with the least structural power, typically get the most out of tight microboundaries and selective course acceptance rather than role redesign.
One caveat the 2024 to 2025 literature is consistent on: organizational interventions produce larger and more sustained effects than individual ones, and combined approaches are recommended for deeper impact.4 The broader nursing faculty shortage makes these institutional investments even more urgent. Use these strategies, but do not treat them as the whole answer.
Research consistently shows that organizational interventions outperform individual coping strategies alone. Journaling, mindfulness, and setting boundaries can help, but they cannot fix unsustainable workloads, inadequate pay, or a culture that ignores educator needs. Self-care without systemic change is a temporary patch. The next section explores what institutions and leaders must do to create environments where nurse educators can genuinely thrive long-term.
Institutional and Leadership Interventions That Work
Institutional commitment is the single most powerful lever for reducing nurse educator burnout and improving retention.
Structured Peer Mentorship for Faculty Support
Research consistently shows that peer mentoring reduces isolation and accelerates acclimation for new nurse educators, directly improving retention. Pairing novices with experienced faculty through formal programs provides a safe space for discussing challenges, sharing teaching strategies, and navigating institutional culture. The Daily Nurse source highlights mentorship as a critical retention tool; institutions that invest in structured pairing see lower turnover and higher job satisfaction among their educators.1
AI-Integrated LMS Platforms That Streamline Work
Administrative overload is a primary burnout driver, but AI-supported learning management systems are now offering targeted relief.2
- Canvas LMS: Features AI-assisted quiz generation, automated rubric creation, and student performance analytics that flag at-risk learners, reducing time spent on clerical tasks.
- D2L Brightspace Lumi AI: Can build entire course modules and assessments from a syllabus, plus predictive learner analytics and AI-assisted feedback.
- Adaptive courseware: Auto-grades NCLEX-style questions, provides individualized remediation plans, and delivers at-risk student dashboards.
These tools reclaim hours each week, letting educators focus on teaching and mentoring rather than repetitive documentation. Faculty at several institutions report saving up to 5 to 7 hours per week on grading and course management after adopting AI-enhanced platforms.3 For educators preparing students for the redesigned licensure exam, curriculum mapping for NGN adds another layer of course-design complexity that AI tools can help manage.
Competitive Pay and Loan Forgiveness as Retention Levers
Pay disparities between academic and clinical roles remain a stubborn driver of faculty attrition. According to the 2026 Daily Nurse article, competitive compensation is non-negotiable for attracting and retaining qualified nurse educators.1 Loan forgiveness programs tied to teaching service in nursing programs further ease the financial burden, making the transition from bedside to classroom more viable. When institutions align salaries closer to clinical benchmarks, they signal that educator expertise is valued.
Realistic Workload Models That Prevent Overload
Traditional faculty workloads often obscure the true time required for course development, advising, and committee work. A typical nurse educator day already spans clinical supervision, lectures, and student advising, so credit-hour equivalency models that assign a weighting for preparation and grading are essential for preventing hidden overload. Release time for scholarship protects educators' ability to remain clinically and academically current, which in turn boosts classroom credibility and personal satisfaction. Capping committee assignments prevents the relentless accumulation of service obligations that fuels burnout.
Leadership Development and Robust Onboarding
New faculty who undergo comprehensive orientation programs built around competency milestones and ongoing support feel more prepared and less likely to leave. Effective programs go beyond a checklist: they include ongoing mentorship, peer support networks, and gradual integration into committee work. Pairing this with leadership development opportunities creates a pipeline of confident, engaged educators who are equipped to handle the rigors of the role, as underscored in the Daily Nurse recommendations.1
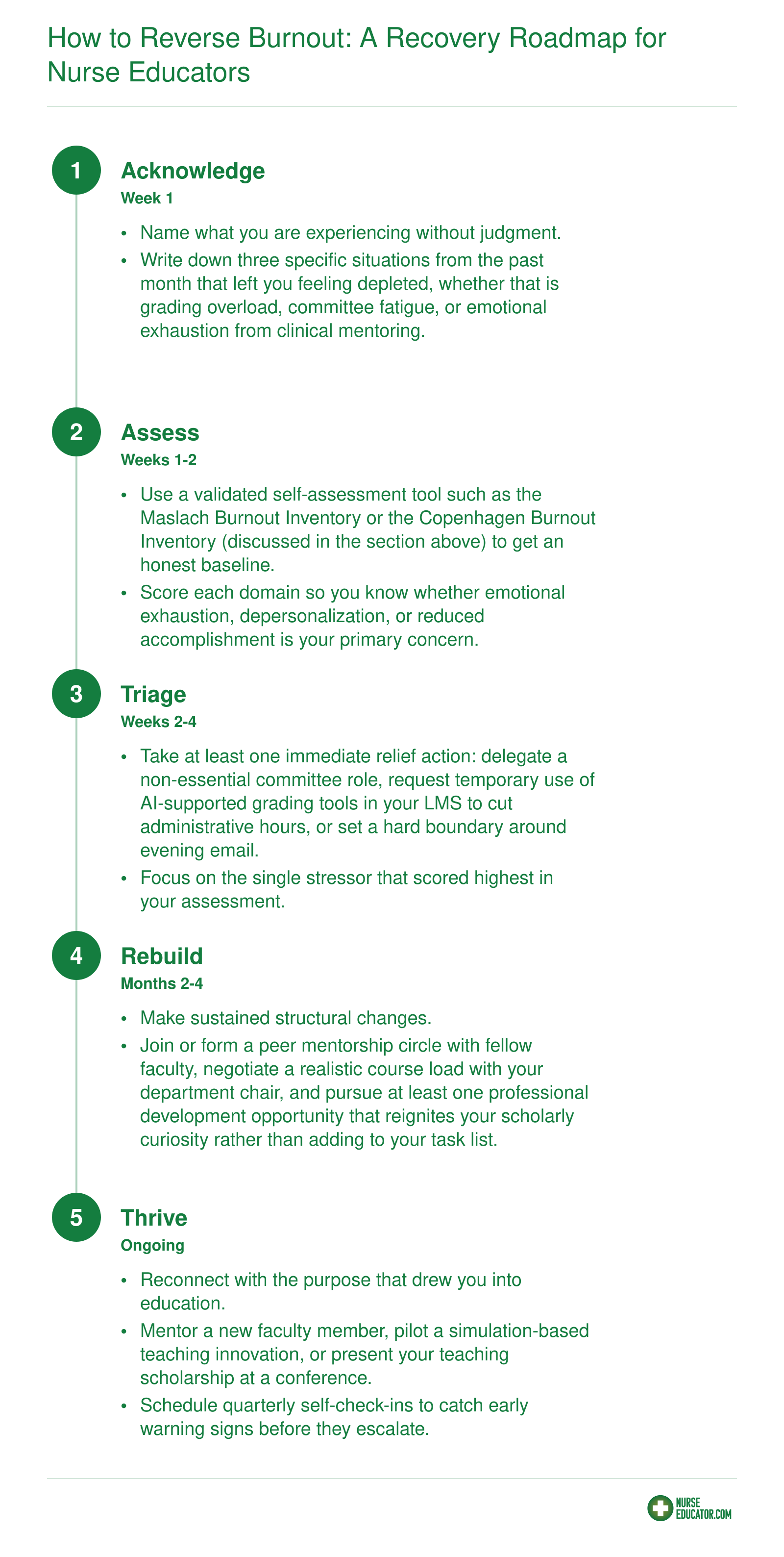
How to Reverse Burnout: A Recovery Roadmap for Nurse Educators
Recovery from burnout is not a straight line. You may circle back to earlier stages as semesters shift or new stressors emerge, and that is completely normal. The important thing is to keep moving forward, even in small steps. If you have been asking yourself how to reverse teacher burnout, this five-stage framework offers a practical path designed specifically for nursing faculty.
Advocating for Change: What Nurse Educators Can Push For
Advocacy, in this context, means making a structured case to the people who control your workload, your budget lines, and your contract: department chairs, deans, provosts, and accreditation liaisons. It is not vague complaining or waiting for a wellness committee to fix things. It is presenting specific, prioritized asks backed by data the institution already cares about: retention numbers, NCLEX pass rates, accreditation standards, and student satisfaction scores.
A Prioritized List of Asks, From Easy Wins to Systemic Reform
- Workload transparency: Ask for a written accounting of teaching, advising, committee, and clinical supervision hours per faculty member. This costs nothing and surfaces hidden inequities.
- Meeting-free days and protected scholarship time: One full day per week with no scheduled meetings is a high-impact, zero-budget change.
- Administrative support and technology adoption: Push for shared course coordinators, grading assistance, and AI-supported learning management tools that automate routine tasks.
- Mentorship and orientation funding: Formal mentoring programs and structured onboarding for new faculty reduce first-year attrition significantly.
- Salary parity and tenure-track expansion: The longest fight, but the one that addresses the root pay gap between academic and clinical roles.
How to Frame the Conversation
Instead of "I am overwhelmed," try: "Our program lost two faculty last year, and I am currently covering 1.4 FTE in teaching load. Here is what I need to sustain quality instruction." Tie every request to a metric the dean reports upward: faculty retention, applicant yield, accreditation compliance with CCNE or ACEN standards on faculty sufficiency, and student outcomes. Accreditors explicitly evaluate whether faculty workload supports program quality, which makes well-being a compliance issue, not a personal one. If you need data to support your case, the broader nurse educator shortage picture provides compelling national context.
If You Are Adjunct or Non-Tenure-Track
Individual leverage is limited, so build coalitions. Connect with full-time colleagues who can carry your concerns into governance meetings you cannot attend. Organize informally through email groups, contingent faculty caucuses, or your campus AAUP chapter. Document patterns across multiple adjuncts rather than raising isolated complaints.
Use Professional Organizations as Amplifiers
The National League for Nursing and the American Association of Colleges of Nursing publish faculty workload benchmarks, salary surveys, and position statements you can cite directly. Walking into a meeting with NLN data showing your institution lags peer programs on faculty compensation reframes the conversation from personal request to competitive necessity. You can also explore nurse educator resources for downloadable tools, salary benchmarks, and advocacy templates.
Frequently Asked Questions About Nurse Educator Burnout
These are among the most common questions nurse educators ask when they start recognizing the toll their workload takes. Each answer offers a brief overview; for a deeper look, refer to the corresponding section earlier in this article.
Is nurse educator burnout a personal shortcoming? No. As demonstrated throughout this article, burnout among nurse educators is a systemic issue fueled by understaffing, workload strain, pay disparities, and insufficient institutional support. The data is clear: nearly 66,000 qualified applicants were turned away in a single year because we lack the faculty to teach them. Every educator who stays in the role trains hundreds of future nurses. When burnout forces you out, the entire pipeline suffers.
Your next step is simple and concrete: choose one self-assessment tool from the section above, complete it this week, and share your results with a trusted colleague or mentor. That single conversation can shift isolation into connection and silence into advocacy. If you are still weighing whether becoming a nurse educator is sustainable, know that real change starts when individuals and institutions act together. Your well-being matters, not just for your own health, but for every student you will teach and every patient they will care for.