What you’ll learn in this article…
- Structured EI training can raise nursing students' emotional intelligence scores by 10 to 15 percent in one semester.
- Validated tools like the EQ-i 2.0 and MSCEIT let programs measure EI gains with peer-reviewed rigor.
- Empathy taught without paired resilience skills accelerates compassion fatigue rather than preventing it.
- Embedding EI across clinical placements requires equipping preceptors with specific coaching language and rubrics.
New-graduate nurse turnover hovers near 35 percent in many large health systems, driven less by clinical knowledge gaps than by emotional exhaustion. A nurse who reads a rhythm strip perfectly freezes when a patient's family erupts in anger. The textbook explains the physiology; it does not explain holding your emotions steady while the room destabilizes.
Emotional intelligence and resilience are not personality traits; they are teachable competencies with measurable progressions. The evidence for structured training in nursing education has grown sharply since 2020, and programs that treat EI as a core clinical skill produce graduates with greater confidence, less burnout, and stronger clinical reasoning under stress.
Yet most curricula still devote 90 percent of classroom time to pathophysiology and pharmacology, leaving emotional skill-building to chance. If you are exploring becoming a nurse educator, this gap represents both a problem and an opportunity: you can be the one who closes it.
What Is Emotional Intelligence in Nursing and Why Does It Matter?
Emotional intelligence is not a soft skill add-on in nursing; it is a core clinical competency that shapes patient outcomes, team function, and career longevity. Nurses who can accurately identify their own emotional states, regulate their reactions under pressure, read patient cues beyond vital signs, and communicate effectively across disciplines deliver safer, more patient-centered care. For nurse educators, building emotional intelligence in students early creates a foundation for clinical judgment that textbooks and simulations alone cannot replicate. That capacity to blend affective awareness with clinical reasoning is one of the qualities of a good nurse educator that separates adequate instruction from transformative teaching.
The Five Components of EI in Nursing Practice
Psychologist Daniel Goleman identified five components of emotional intelligence that translate directly into everyday nursing scenarios:
- Self-awareness: Recognizing your own stress, frustration, or fatigue before it clouds clinical judgment. A self-aware nurse knows when to ask for help during a complex procedure or when personal bias might shape a patient interaction.
- Self-regulation: Maintaining composure and focus during high-stakes situations. During a code blue, self-regulation allows a nurse to execute protocols without freezing or escalating panic in the room.
- Motivation: Sustaining commitment to patient care even when the work is emotionally taxing. Motivated nurses seek learning opportunities in difficult cases rather than avoiding them.
- Empathy: Understanding and responding to patients' emotional states, particularly in end-of-life conversations, chronic pain management, or delivering unexpected diagnoses. Empathy informs tone, pacing, and the choice to sit rather than stand during a difficult disclosure.
- Social skills: Navigating interdisciplinary teams, resolving conflicts with physicians or ancillary staff, and advocating for patient needs across hierarchies. Social skills drive effective handoffs, care coordination, and the ability to influence without formal authority.
How EI Translates to Quality of Care
Research links higher emotional intelligence among nurses to measurable improvements in patient safety and satisfaction. Studies show that emotionally intelligent nurses make fewer medication errors, likely because they remain calm and methodical under time pressure and double-check orders when something feels off. Patient satisfaction scores, including HCAHPS domains related to communication and responsiveness, correlate with nurse empathy and interpersonal skill. Therapeutic relationships built on trust and emotional attunement improve adherence to treatment plans and patient-reported outcomes.
Why EI Is Not the Same as Being Nice
Emotional intelligence is frequently confused with kindness or agreeableness, but it is a distinct professional competency. An emotionally intelligent nurse can deliver unwelcome news with clarity and compassion, set firm boundaries with a demanding family, or de-escalate an agitated patient without compromising safety. EI predicts clinical judgment because it integrates affective and cognitive processes: recognizing subtle changes in patient demeanor, inferring unspoken concerns, and adjusting communication strategies in real time. Understanding this distinction also helps dispel common nurse educator misconceptions about what "soft" content belongs in a rigorous curriculum.
Why Nursing Students Need EI Development Early
Developing emotional intelligence during prelicensure education reduces attrition and eases the transition from classroom to bedside. Students with higher EI report lower anxiety during clinical rotations, stronger relationships with preceptors, and greater confidence managing emotionally charged situations. Early EI training equips students to process the emotional labor of nursing before they reach burnout thresholds, building resilience alongside technical skill. If you are considering a nurse to teacher career change, weaving EI into your teaching philosophy gives you a concrete framework that clinical experience alone does not always provide.
The Evidence: How EI and Resilience Training Improve Student Outcomes
Anecdotal classroom success stories versus controlled research findings: both matter, but the latter carries the weight needed to justify curricular change. If you are advocating for emotional intelligence and resilience training in your nursing program, knowing where the evidence stands (and where it falls short) will strengthen your case considerably.
What the Research Shows So Far
A growing body of peer-reviewed literature supports the idea that structured EI and resilience interventions improve measurable student outcomes. Meta-analyses published in journals such as Nurse Education Today and the Journal of Nursing Education consistently report positive associations between EI training and reduced perceived stress, improved clinical communication, and higher self-reported empathy scores. Quasi-experimental designs have linked resilience-building curricula to lower attrition: some programs have documented retention improvements in the range of 8 to 15 percentage points among cohorts that received targeted resilience support compared with those that did not.
Randomized controlled trials (RCTs) in this space do exist but remain relatively uncommon, and effect-size reporting for non-clinical skills is often incomplete. When effect sizes are reported, they tend to be small to moderate (Cohen's d in the 0.3 to 0.6 range for self-awareness and emotion regulation subscales). That is meaningful in an educational context, though it underscores the need for larger, multi-site trials to confirm generalizability.
Where to Find Reliable Data
Building a literature review for your own program proposal takes some deliberate sourcing:
- Peer-reviewed journals: Search databases like CINAHL, PubMed, and Scopus for RCTs and quasi-experimental studies. Filter for post-2020 publications to capture the most current designs, but expect that many studies still rely on pre/post single-group comparisons rather than true control groups.
- Professional association resources: The American Nurses Association and the National Council of State Boards of Nursing publish white papers and continuing education modules that synthesize training effectiveness data. These are especially useful for translating research into policy language.
- University program websites: A growing number of nursing schools now publish outcome dashboards or annual reports that include data from their EI or resilience initiatives, such as changes in NCLEX pass rates, clinical evaluation scores, or student wellness survey results.
- Federal labor data: The Bureau of Labor Statistics (BLS.gov) provides employment projections and wage data for nursing roles. While these figures do not measure EI directly, they contextualize the competitive landscape: as demand for nurses continues to grow, programs that can demonstrate lower burnout and higher retention among graduates hold a real advantage in attracting applicants and clinical partners.
Acknowledging the Gaps
Honesty about limitations makes your argument stronger, not weaker. Most EI research in nursing education relies on self-report instruments, which are subject to social desirability bias. Burnout reduction data, while promising, often comes from short follow-up windows of one semester or less, making it hard to confirm lasting effects. Clinical performance metrics tied specifically to EI training, rather than to overall academic preparation, are still emerging.
None of this invalidates the case for teaching emotional intelligence to nursing students. It simply means that as a nurse educator, you are building the evidence base alongside your curriculum. Design your interventions with evaluation in mind from day one: use validated instruments, include comparison groups when feasible, and plan for longitudinal follow-up. Programs that retain and graduate resilient nurses also help address the broader nursing faculty shortage, because graduates who thrive in practice are more likely to return to academia later. The programs that pair rigorous evaluation with innovative nursing education curriculum are the ones shaping the next wave of published evidence, and you will find concrete examples of their approaches later in this article.
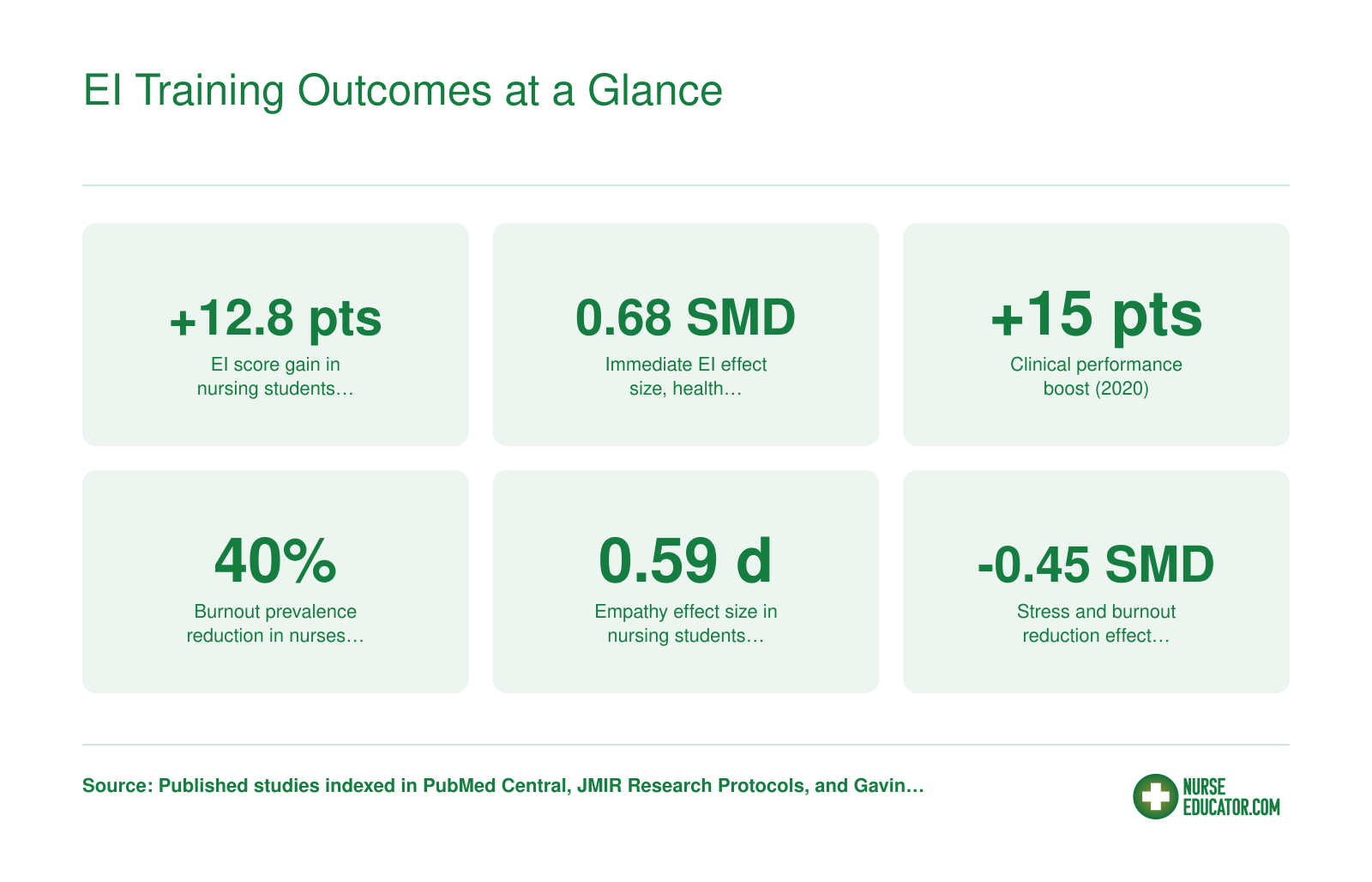
EI Training Outcomes at a Glance
Research consistently shows that structured emotional intelligence and resilience training produces measurable gains for nursing students and practicing nurses alike. Here are six key findings from published studies and meta-analyses.
Validated EI Assessment Tools for Nursing Education
Choosing the right emotional intelligence assessment comes down to a core tradeoff: do you need a tool that fits inside a single class session, or one that can stand up to peer-reviewed scrutiny in a program evaluation? The instruments below vary considerably on both dimensions, and the right choice depends on your timeline, budget, and how you plan to use the data.
Schutte Self-Report EI Scale (SSREI)
The SSREI is the workhorse of nursing education research, and for good reason. Its 33 items tap four facets of trait emotional intelligence: appraisal of emotions in self and others, regulation of emotions, utilization of emotions, and social skills.1 Respondents complete it in five to ten minutes, internal reliability runs between 0.87 and 0.90 across studies, and test-retest reliability sits at 0.78, meaning scores hold up reasonably well over time.2 The scale is free for research use, which makes it practical for programs running semester-long pre-post designs.2 Because it appears frequently in nursing student research, you can compare your cohort's mean scores against published benchmarks from similar populations, something harder to do with less common instruments.
TEIQue-SF
The Trait Emotional Intelligence Questionnaire-Short Form condenses a longer instrument into 30 items and produces a global trait EI score along with four factor scores. Like the SSREI, it is self-report and takes roughly ten minutes. The TEIQue-SF has been validated across multiple countries and age groups, and a free research license is available through the London Psychometric Laboratory. It works well as a baseline screen at program entry and can be paired with the full TEIQue if deeper subscale data are needed for a capstone or thesis project.
MSCEIT
The Mayer-Salovey-Caruso Emotional Intelligence Test takes a fundamentally different approach. Rather than asking respondents how they perceive their own emotional skills, it presents actual cognitive tasks: identifying emotions in faces, reasoning about emotional scenarios, and solving emotion-laden problems.3 This ability-based format reduces social desirability bias and produces scores that correlate more strongly with real-world performance, though administration takes 30 to 45 minutes and the instrument carries a per-use fee through Multi-Health Systems. For programs conducting rigorous outcome research or affordable nurse educator DNP programs tied to grant-funded faculty development studies, the MSCEIT's objectivity is a genuine advantage. For a 15-week semester with limited assessment windows, the cost and time commitment may be harder to justify.
Wong and Law Emotional Intelligence Scale (WLEIS)
The WLEIS is a 16-item self-report scale built around four dimensions: self-emotion appraisal, others-emotion appraisal, use of emotion, and regulation of emotion. It was designed with applied organizational research in mind, and its brevity makes it particularly useful when EI is one of several constructs being measured in a single survey session. Psychometric properties are solid across published nursing and healthcare samples. It does not require a license fee for academic research, though researchers should contact the authors for permission before use in formal studies.
Choosing the Right Tool for Your Program
Here is a practical framework for narrowing the field:
- Pre-post semester evaluation: The SSREI or WLEIS both work well. Short administration time leaves room for intervention between measurement points, and both have published nursing-student data for rough benchmarking.
- One-time baseline at program entry: The TEIQue-SF gives a clean global score plus factor-level detail without overloading students during an already busy orientation period.
- Rigorous research or grant-funded studies: The MSCEIT's ability-based design is more defensible in peer-reviewed contexts, and its resistance to response bias strengthens internal validity even at higher cost.3
- Embedded clinical or preceptorship assessment: The WLEIS is short enough to administer alongside other clinical evaluation forms without adding meaningful burden.
No published nursing-specific norms exist for all of these instruments, so interpret any cohort comparison cautiously. Where nursing-student benchmarks have been published, they tend to come from single-country samples and may not generalize to your student population. Treat comparative data as directional rather than definitive, and prioritize tracking change within your own program over time.
Questions to Ask Yourself
How to Teach Emotional Intelligence to Nursing Students: Curricular Strategies
Teaching emotional intelligence means giving students structured, repeated practice in recognizing feelings, responding thoughtfully, and recovering when things go wrong. It is not a single lecture or a wellness workshop tacked onto orientation. Done well, it runs through an entire program as a thread, not an add-on.
Five Methods That Actually Work in the Nursing Classroom
- High-fidelity simulation with embedded EI triggers: Set up a standardized patient scenario in which the patient becomes visibly angry after receiving a delayed diagnosis. Brief the actor to escalate gradually so students must de-escalate in real time, not just demonstrate clinical skills. Debrief immediately afterward using video review, asking students to identify the moment they noticed the emotional shift and what they chose to do about it. This scenario can be ready for next semester with an existing sim lab and a faculty-written script.
- Structured reflective journaling: Prompt students with specific questions rather than open-ended free writing. Examples: "Describe a moment this week when you felt frustrated with a patient. What did that feeling tell you about your expectations?" Collect entries bi-weekly so faculty can spot patterns before they become problems.
- Gibbs reflective cycle debriefing: After clinical rotations, walk students through the six Gibbs stages (description, feelings, evaluation, analysis, conclusion, action plan) in small groups. The cycle works well because it separates the factual account from the emotional response, which helps students who conflate the two.
- Peer role-play with feedback rubrics: Pair students and assign one the patient role, one the nurse role. Give observers a rubric that scores specific EI behaviors: eye contact during distress, tone calibration, use of silence, and so on. Rotate roles across the semester so every student experiences being on the receiving end of poor communication.
- Semester-long EI portfolios: Ask students to curate evidence of their emotional growth over an entire term. Artifacts might include journal excerpts, a self-scored EI assessment taken at week one and week fourteen, a reflection on peer feedback received, and a personal resilience action plan.
Sequencing Across the Program
The order matters as much as the methods. In Year 1, anchor the work in self-awareness: students need a vocabulary for their own emotional states before they can reliably read others. Journaling, introductory self-assessments, and low-stakes role-play fit here.
Year 2 shifts toward empathy and social skill development. High-fidelity simulation, Gibbs debriefs after clinical placements, and structured peer feedback move center stage because students now have enough clinical context to make the emotional scenarios feel real. These approaches align with broader innovative teaching strategies in nursing education that prioritize active learning over passive content delivery.
Capstone and leadership courses are the place for integration. Students in these courses should be applying EI in complex team dynamics, navigating conflict with colleagues, and reflecting on how their emotional style shapes the care environment around them. Portfolio presentations and leadership-focused simulation scenarios anchor this final layer.
Assessing EI: Formative and Summative Approaches
Formative assessment keeps the learning loop tight. Journaling entries, peer feedback scores from role-play rubrics, and faculty observation notes during simulation debriefs all serve this purpose. They flag students who are struggling with self-regulation before those struggles reach the clinical floor.
Summative assessment requires more deliberate design. OSCE-style EI stations, in which students rotate through standardized patient encounters scored on emotional competencies, give programs defensible, observable data. Both academic vs clinical nurse educators can contribute to this evaluation process by scoring from their respective vantage points. Pairing a validated EI instrument administered at program entry with the same instrument at graduation adds a pre-post comparison that can inform both individual advising and program-level evaluation. Neither approach replaces the other; together they give faculty a complete picture of where each student started and how far they have come.
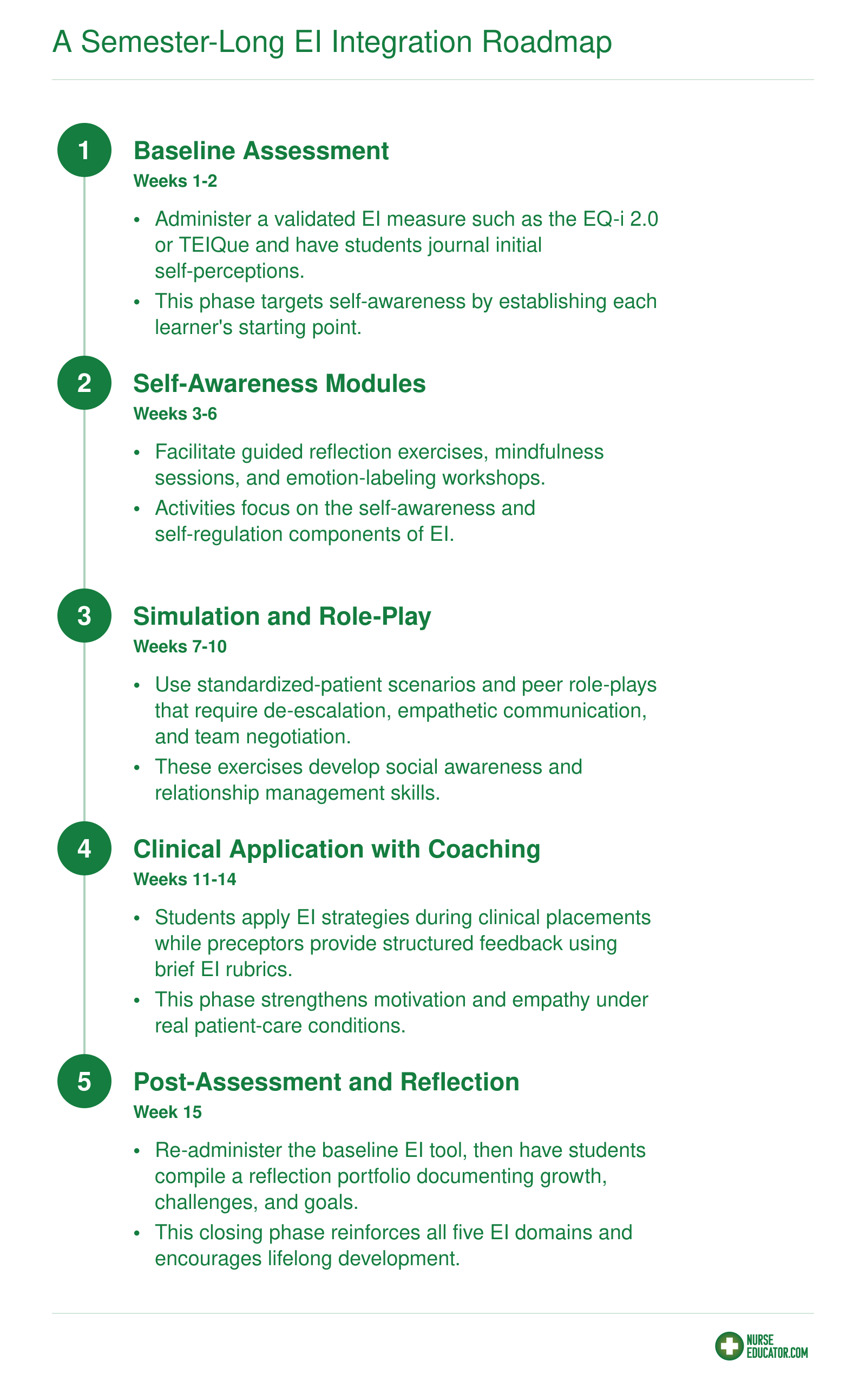
A Semester-Long EI Integration Roadmap
Embedding emotional intelligence across a full semester lets nursing students build skills incrementally, moving from self-knowledge to real-world clinical application. The roadmap below maps each phase to specific activities and the EI competency it develops.
Building Resilience: Frameworks and Activities for the Nursing Classroom
A single end-of-semester wellness workshop versus a structured, semester-long resilience thread woven into every course week: the difference in student outcomes is dramatic. Resilience is not a trait students either have or lack. It is a set of skills that can be taught, practiced, and measured, and it maps directly onto the emotional intelligence competencies your curriculum already targets.
Three Evidence-Based Frameworks Worth Knowing
The Connor-Davidson Resilience Scale (CD-RISC) is probably the most widely used measurement tool in nursing education research.1 Available in 25-item, 10-item, and 16-item versions, it assesses personal competence, trust in one's instincts, positive acceptance of change, perceived control, and spiritual influences.2 The 10-item version has been validated with good construct validity and internal consistency (Cronbach's alpha of 0.81) in student nurse populations.3 Baccalaureate programs frequently administer the CD-RISC at baseline to identify students who may benefit from targeted support and to inform broader curriculum design.2 Because the scale captures self-regulation and adaptive coping, it connects directly to the EI domains of self-awareness and self-management.
The APA resilience model, originally designed for general populations, has been adapted for healthcare workers around five pillars: building connections, fostering wellness, finding purpose, embracing healthy thought patterns, and seeking help.2 Nursing programs integrate these elements implicitly through coping-skills training, reflective practice, emotional-regulation exercises, and social-support structures. The "seeking help" pillar is especially relevant because it ties resilience to the EI social skill of help-seeking behavior, something many high-achieving nursing students resist.
The NTU resilience framework is less widely documented in peer-reviewed literature, but it has drawn interest for its holistic emphasis on cultural identity and meaning-making.2 If your student body is diverse, it can complement the APA model by validating culturally grounded sources of strength. If you teach in a program that actively works to promote health equity, this framework deserves a closer look. Treat it as an emerging option rather than a fully validated tool at this stage.
Classroom-Ready Activities
Four activities translate these frameworks into weekly practice.
- Five-minute guided mindfulness check-ins: Open each pre-clinical session with a brief body-scan or breathing exercise. Research on mindfulness programs for nursing students shows increased resilience scores alongside decreased stress and anxiety.2 The key is consistency: aim for at least three sessions per week across the full semester, not a handful of one-off introductions.
- Peer-support triads with structured debriefs: Assign students to rotating groups of three. After high-intensity simulation labs or clinical shifts, each member shares one emotional challenge from the day while the other two practice active listening. Provide a debrief protocol ("What happened? What did you feel? What would you do differently?") so the conversation stays productive. Weekly triads build the social-skill layer of EI and normalize help-seeking.
- Gratitude and meaning-making journals: After difficult patient encounters, ask students to write two or three sentences identifying something they learned or a moment of connection. This targets the "finding purpose" pillar of the APA model and strengthens the self-awareness component of EI. Collect entries biweekly so you can spot students who are struggling to find meaning, a potential early indicator of compassion fatigue.
- Stress inoculation through graded simulation exposure: Design simulation scenarios that progressively increase in emotional complexity, from a routine medication error disclosure to a patient death notification. Follow each scenario with a debrief focused on cognitive appraisal, coping strategies, and professional identity. Problem-based learning research shows this approach builds self-efficacy, optimism, motivation, and self-reflection in nursing students.2
Why Resilience and EI Are Inseparable
Self-regulation is the engine behind bounce-back. A student who can name an emotion, pause before reacting, and choose a constructive response recovers faster from clinical setbacks. Without that self-regulation capacity, even highly empathic students are vulnerable to compassion fatigue: they absorb patients' distress without a mechanism to process and release it. Research confirms that higher resilience and self-compassion are associated with lower self-handicapping behaviors in nursing students.4 Social skills complete the picture by enabling students to reach out for support rather than powering through alone.
A Note on Dosage
Resilience is not built in a single workshop. The evidence points toward sustained, recurring practice:
- Mindfulness check-ins work best at a minimum of three times per week, five minutes each, for at least eight consecutive weeks.
- Peer-support triads should meet weekly throughout a clinical rotation or simulation course.
- Journaling is most effective when practiced after every significant clinical encounter, with faculty review at least every two weeks.
- Graded simulation exposure should follow a scaffolded sequence across an entire semester, with debrief sessions that explicitly connect coping strategies to EI competencies.
If your program can only start with one activity, choose the five-minute mindfulness check-in. It has the lowest barrier to implementation, requires no special training, and the evidence base for its impact on nursing student resilience is strong. Layer in the other activities as faculty comfort and scheduling allow.
Empathy taught in isolation, without paired self-regulation and resilience skills, can accelerate compassion fatigue rather than prevent it. When students learn to absorb patients' distress but lack strategies for emotional recovery, the result is chronic exhaustion, not compassionate care. Effective programs treat empathy and resilience as two halves of one equation: neither works without the other.
Integrating EI Into Clinical Placements and Preceptorships
Clinical rotations bridge classroom learning and practice, yet many programs still rely on preceptors to model technical competence without explicitly addressing how to coach or assess emotional intelligence in real time. The challenge is straightforward: busy preceptors often lack the language, tools, or training to provide meaningful EI feedback, even when they intuitively recognize that a student struggles with empathy or self-regulation. Formalizing EI integration into clinical placements requires deliberate design across three layers: preceptor orientation, real-time coaching techniques, and structured assessment.
Preceptor Modeling and Narrated EI Reasoning
The most powerful EI instruction happens when preceptors narrate their emotional reasoning as they work. Rather than moving silently through a difficult patient conversation, an effective preceptor might say, "I noticed the family was anxious and speaking over one another, so I slowed down, acknowledged their worry explicitly, and asked one direct question to help them prioritize." This think-aloud approach makes invisible EI competencies visible. Preceptors can also debrief moments when their own self-regulation was tested: "When that patient snapped at me, I felt defensive. I took a breath and reminded myself he's in pain, which helped me respond calmly." Students begin to recognize emotional data as clinical data, worthy of the same deliberate interpretation.
A Simple EI Feedback Rubric for Clinical Debriefs
Preceptors need a lightweight framework to structure EI feedback during shift debriefs. A practical rubric includes three to four observable behaviors rated on a developmental scale (beginning, developing, proficient):
- Active listening: Allows patient to finish sentences, uses minimal encouragers, reflects emotion or content accurately.
- Emotional self-regulation under pressure: Maintains composure when challenged, recognizes own stress signals, does not escalate conflict.
- Appropriate empathy expression: Acknowledges patient emotion explicitly, calibrates responses to cultural context, avoids dismissive reassurance.
- Constructive conflict handling: Names disagreement directly, invites patient or team input, separates person from problem.
This rubric gives preceptors concrete language and separates EI from vague "professionalism." When combined with brief written comments, students receive actionable guidance on where to focus their growth. If you are building the clinical nurse educator role into your career, developing this kind of structured feedback skill is essential.
OSCE-Style EI Assessment Stations
Objective Structured Clinical Examinations (OSCEs) traditionally evaluate technical and communication skills, but they can be adapted to isolate and measure EI competencies. Published rubrics from nursing OSCE programs already include criteria such as establishing rapport, using therapeutic communication, and responding to patient cues on a 1-to-4 scale.12 In 2026, updated NMC child-field OSCE stations introduced professional values stations that explicitly assess recognition of burnout, self-awareness of stress, and acting on psychological warning signs.3
To design an EI-focused OSCE station, create a standardized patient scenario that minimizes technical decision-making and maximizes emotional challenge. For example, a patient might receive bad news about test results or express anger about wait times, requiring the student to recognize the emotion, manage their own reaction, respond empathetically, and de-escalate the interaction. The standardized patient completes a checklist: "Student acknowledged my frustration," "Student maintained calm tone," "Student did not become defensive." Research on nursing OSCEs combined with structured self-assessment has shown that reflection after the station helps students recognize gaps between perceived and actual performance, supporting targeted learning adjustments.4 Structured debriefing after stations also helps students process the anxiety these high-stakes scenarios can generate.5
Overcoming the Preceptor Readiness Gap
Many preceptors received no formal EI training in their own education. Asking them to coach and assess students on empathy or self-regulation without calibration leads to inconsistent feedback or avoidance of the topic altogether. A brief preceptor orientation module (two to three hours) should introduce the EI framework your program uses, walk through the feedback rubric with examples, and model narrated reasoning using video cases. The orientation establishes shared language, so when a preceptor writes "needs to work on active listening," both student and faculty understand what that means developmentally. Even minimal investment in preceptor onboarding dramatically improves the quality and consistency of EI feedback across clinical sites.
EI Across the Career Continuum: From Student to Nurse Leader
How do the emotional intelligence skills taught in nursing school translate into leadership competencies later in a career? The answer involves a deliberate developmental pathway that many programs overlook, leaving nurses to figure out on their own how basic self-awareness evolves into the organizational savvy required for management and education roles.
A Longitudinal EI Development Map
Emotional intelligence competencies shift in focus and complexity as nurses progress through career stages:
- Student nurse: Core foundation centers on self-awareness (recognizing personal stress responses, identifying emotional triggers) and basic empathy (reading patient distress, responding to family concerns). These are the building blocks.
- New graduate (first two years): Self-regulation becomes paramount as reality shock hits. Managing frustration during high-acuity shifts, recovering from clinical errors, and maintaining composure with difficult patients require deliberate emotional management that classroom simulations only partially prepare you for.
- Experienced clinician (three to seven years): Social awareness expands beyond individual patients to team dynamics. Recognizing when a colleague is struggling, reading unit culture, and navigating interprofessional tensions demand relational intelligence that deepens with exposure.
- Charge nurse or preceptor: Relationship management takes center stage. You are now responsible for de-escalating peer conflicts, providing real-time feedback to orientees, and maintaining team morale during understaffing. Influence without formal authority becomes a daily requirement.
- Nurse educator or manager: Organizational empathy, the ability to sense and respond to the emotional climate of an entire department, student cohort, or institution, emerges as the distinguishing competency. Conflict mediation skills must scale from one-on-one to group facilitation.
- Executive leader: Strategic emotional intelligence involves reading organizational politics, inspiring vision across disparate stakeholders, and modeling vulnerability appropriately to build trust at scale.
Bridging School-Level Skills to Leadership Competencies
The gap between classroom EI instruction and leadership-level application is substantial. Basic empathy taught during patient care scenarios does not automatically translate into mentoring a struggling colleague or mediating faculty disputes. What bridges this gap is structured reflection, advanced feedback mechanisms, and deliberate practice in progressively complex interpersonal situations.
For nurses transitioning into educator roles, the challenge doubles. You must both model emotional intelligence for students and teach it explicitly, a meta-cognitive layer that clinical nurse educator role descriptions rarely address. This means developing the ability to articulate your own EI processes while they happen, turning implicit relational skills into teachable frameworks.
Resources for Post-Graduation EI Development
Continuing education options can support ongoing growth:
- The Consortium for Research on Emotional Intelligence in Organizations offers free research-based resources and periodic webinars on EI application in professional settings.
- The American Organization for Nursing Leadership (AONL) provides leadership development courses that embed EI competencies within broader management curricula, particularly useful for those moving into formal leadership.
- Reflective practice groups or Schwartz Center Rounds at clinical sites create structured spaces for processing emotional experiences with peers, building the reflective capacity that advanced EI requires.
Nursing programs that acknowledge this continuum prepare students not just for bedside care but for the leadership roles the profession urgently needs filled. For those ready to formalize that transition, a post-master's certificate in nursing education can help bridge clinical expertise with pedagogical skill.
Implementation Case Studies: Nursing Programs That Got It Right
BSN-Level: Gardner-Webb's Psychoeducational EI Program
Gardner-Webb University designed a psychoeducational emotional intelligence (EI) program for prelicensure BSN students.1 Students completed the EQ-i 2.0 assessment before and after a structured intervention that included interactive workshops, self-reflection exercises, and peer coaching sessions. The program was delivered across a single semester, with weekly small-group meetings that allowed faculty to reinforce EI concepts in a low-stakes environment.
Post-intervention scores showed significant gains in the self-perception and self-expression composite scales of the EQ-i 2.0.1 Students reported feeling more aware of their emotional triggers and better able to articulate feelings during clinical debriefs. Faculty noted that the small-group format fostered psychological safety, which was essential for honest self-assessment and growth.
Undergraduate Resilience: UMass Amherst Builds Grit
The University of Massachusetts Amherst implemented a resilience-building curriculum for undergraduate nursing students in their second clinical rotation.2 The curriculum spanned six weeks and consisted of weekly two-hour sessions covering stress appraisal, cognitive reframing, mindfulness, and social support mapping. Resilience was measured with a validated resilience scale in a pre-post design.
By the end of the program, students demonstrated a measurable increase in resilience scores and described themselves as more equipped to handle the emotional demands of patient care.2 Qualitatively, participants emphasized the value of having dedicated time to discuss failures and near misses without judgment. The curriculum's success highlighted the importance of integrating resilience training alongside clinical skill development, not as a separate, optional add-on.
Adapting the Blueprint for Graduate Nursing Education
While published case studies at the graduate level are still emerging, many advanced practice programs are beginning to adapt these same evidence-based frameworks. The American Association of Colleges of Nursing's Well-Being & Resilience Initiative offers a detailed toolkit that graduate faculty can use to embed EI and resilience competencies into master's and doctoral curricula. The toolkit's flexible design allows schools to start with brief interventions, such as a resilience self-assessment and a single reflective workshop, and scale up as faculty become more comfortable with the content. Faculty interested in doctoral-level teaching roles can explore affordable nurse educator DNP programs that increasingly emphasize these competencies.
Lessons Learned and Resources Required
Across these implementations, three factors proved decisive. First, a designated faculty champion who received formal training in EI facilitation kept the initiative moving. Second, structured, repeated sessions rather than one-time workshops deepened student learning. Third, using a validated tool like the EQ-i 2.0 or a resilience scale provided credible pre-post data that convinced stakeholders to sustain the work. A separate quasi-experimental study across Pakistan, Saudi Arabia, and the UAE confirmed similar gains when nursing students participated in a structured EI and self-development program, reinforcing the generalizability of these approaches.3 Faculty who ran the programs noted they would push integration earlier in the curriculum next time, ideally threading emotional skill-building into the first semester. On the resource side, the biggest investments were faculty release time (about 40 hours per semester for the champion), training costs for facilitators, and per-student licensing fees for assessment tools. An Arkansas State University quality improvement project also showed that resiliency training for nursing faculty themselves improved stress management and emotional regulation, suggesting that educator preparation matters just as much as student programming.4
Start Small: Your Pilot Semester
An educator can launch a viable pilot with minimal budget by borrowing the structure from these models. Choose one clinical cohort and insert a four-session EI module into their regular seminar time. Use a free, psychometrically sound tool like the Schutte Self-Report Emotional Intelligence Test (SSEIT) for pre-post measurement. Pair the sessions with guided reflective journaling and a short debrief each week. This approach generates pilot data you can share with your curriculum committee, building the case for a broader, resourced rollout the following year. The key is to begin measuring what matters, and these case studies prove it can be done.
Frequently Asked Questions About EI in Nursing Education
These are some of the most common questions nurse educators ask when exploring emotional intelligence integration. Each answer draws on current evidence and practical tools discussed throughout this guide.