What you’ll learn in this article…
- Over 1,600 full-time nursing faculty positions were vacant during the 2024-2025 academic year, fueling urgent demand for nurse educators.
- Academic nurse educator salaries typically fall below RN and NP medians, though benefits like tuition remission and summers off narrow the real gap.
- Low-cost steps such as clinical precepting or guest lecturing let you test your fit for teaching before committing to an MSN program.
- Burnout, schedule predictability, and the desire to shape the next generation rank among the top reasons nurses leave the bedside for education.
Nursing programs turned away more than 80,000 qualified applicants in 2024, largely because schools could not hire enough faculty to teach them. Behind that statistic sits a quieter shift: thousands of experienced RNs are stepping away from 12-hour floor shifts, trading scrubs for lecture halls and simulation labs.
The reasons run deeper than simple career fatigue. Many nurses hit a wall after years of physical strain, rotating schedules, and the emotional weight of direct patient care. Others want to shape the next generation of clinicians rather than manage one patient assignment at a time. The growing nurse educator shortage only amplifies the urgency of that calling. But wanting a change and making a smart transition are different things.
Salaries often drop. Academic job security varies by institution type. The path from bedside to classroom requires credentials, planning, and an honest look at what you are willing to trade.
Top Reasons Nurses Transition Into Educator Roles
Nurses do not leave the bedside on a whim. The decision to move into education is almost always driven by a combination of forces that have been building for years, and understanding those forces makes the path forward much clearer.
Multiplying Your Impact
One of the most cited reasons to become a nurse educator is the shift in scale. At the bedside, a skilled nurse changes lives one patient at a time. In the classroom, that same nurse can shape the clinical judgment, ethical reasoning, and technical skill of hundreds of students over the course of a career. For nurses who have spent years accumulating hard-won knowledge, teaching becomes a way to make that expertise work far beyond any single shift or unit.
Physical and Emotional Sustainability
The body keeps score. Twelve-hour shifts, overnight rotations, frequent lifting, and the relentless pace of acute care settings take a cumulative toll that no amount of passion fully offsets. Many nurses reach a point in their thirties or forties when continuing at that intensity feels genuinely unsustainable. Educator roles, whether in a university classroom or a hospital staff-development department, tend to involve more predictable schedules and far less physical strain. That is not a retreat from nursing; it is a practical decision to protect a long career.
Emotional burnout plays an equally large role. Chronic exposure to trauma, understaffing, and moral distress exhausts even the most resilient clinicians. Stepping into education allows nurses to remain deeply embedded in the profession while rebuilding the reserves that direct care can deplete.
A Latent Passion, Finally Recognized
Many nurses discover their teaching instincts long before they formalize them. The nurse who volunteers to precept every new graduate, who rewrites the unit orientation checklist because the old one was confusing, who stays late explaining the pathophysiology behind a medication to an anxious student: that person is already teaching. Moving into an official educator role often feels less like a career change and more like finally catching up to what you were already doing. If that description sounds familiar, you may want to explore the signs you should become a nurse educator.
Schedule, Flexibility, and the Long View
Academic calendars offer rhythms that hospital staffing grids simply cannot. Semester breaks, more consistent daytime hours, and the growing availability of remote or hybrid positions in online nurse educator program advantages all appeal to nurses who are also managing family responsibilities or pursuing advanced degrees. The lifestyle alignment is real, and for many nurses, it is the final factor that tips the decision.
Paying It Forward
Experienced nurses carry a detailed memory of what it felt like to be underprepared: the first code, the first time a patient deteriorated without warning, the procedures no simulation fully replicates. Many transition into education specifically to close those gaps for the next generation. The motivation is less about leaving clinical practice and more about ensuring that the nurses coming up behind them arrive better equipped than they did.
Nurse Educator Vs. Bedside Nursing: A Side-By-Side Comparison
Twelve-hour shifts on a hospital floor versus a semester-based academic calendar: the daily reality of bedside nursing and nurse education could hardly look more different. Before you commit to a career change, understanding how these paths diverge across schedule, physical toll, flexibility, pay trajectory, burnout risk, and long-term growth will help you make an informed decision.
Weekly Schedule and Workload
Bedside RNs typically work 36 to 48 hours per week, often in rotating day, night, or weekend shifts. Schedules are dictated by patient census and unit needs, leaving little room for negotiation.
Academic nurse educators report 40 to 60 hours weekly, though the breakdown is far less predictable.1 A typical week might include 4 to 8 hours of classroom teaching, 6 to 16 hours of clinical supervision, 8 to 15 hours of grading, 3 to 8 hours of committee meetings, and 3 to 5 hours of student advising.2 Research-intensive universities expect an additional 8 to 16 hours devoted to scholarship.3 Clinical nurse educators land closer to 40 to 45 hours, with heavier clinical supervision loads (16 to 24 hours) and 10 to 16 hours of preparation and documentation. For a deeper look at how these two tracks differ day to day, see our breakdown of academic vs clinical nurse educator roles.
Be realistic: educator hours spike hard during midterms, finals week, and accreditation reviews. This is not a pure nine-to-five.
Physical Demands
Bedside nurses spend entire shifts on their feet, lifting patients, responding to codes, and managing the sensory overload of alarms and emergencies. The physical wear accumulates over years.
Educators trade that intensity for prolonged sitting, screen time, and voice strain from lecturing. Clinical supervision still requires standing and walking, but the acute lifting and rapid-response demands drop substantially.
Autonomy and Flexibility
Bedside nurses have limited control over when and where they work. Mandatory overtime, floating to unfamiliar units, and holiday rotations are common.
Academic educators enjoy more predictability: semester calendars are set months in advance, and grading or course prep can often be done remotely. That said, committee obligations and accreditation deadlines can erode flexibility during crunch periods.
Compensation Trajectory
Entry-level educators may earn slightly less than experienced bedside RNs, especially those working nights or weekends with shift differentials. Over time, however, educators can advance to program director, department chair, or dean roles with salaries that exceed most staff-nurse positions. Research grants and consulting can add supplemental income for faculty at universities. For a broader look at advancement options, explore nurse educator career advancement paths.
Burnout Risk and Job Satisfaction
Recent workforce surveys show 40 to 50 percent of bedside nurses report high burnout, driven by staffing shortages, emotional exhaustion, and moral distress.5 Job satisfaction in that group trends low.
Academic nurse educators report moderate burnout, with satisfaction levels ranging from moderate to high.5 The stressors differ: publication pressure, heavy grading loads, and shrinking budgets replace bedside emergencies, but most educators describe a renewed sense of purpose in shaping the next generation.
Career Ceiling
Bedside nursing offers a clear but relatively flat trajectory: staff nurse, charge nurse, unit manager. Advanced practice roles require additional degrees.
Education opens pathways to curriculum design, simulation center leadership, associate dean, or provost-level administration. A doctorate unlocks the widest range of options, but even an MSN-prepared educator can rise to clinical coordinator or assistant program director at many schools. You can learn more about the full scope of the difference between a nurse and a nurse educator to see how far these trajectories can diverge.
Use the comparison above to weigh what you are willing to trade. Neither path is objectively better; the right fit depends on whether you thrive in acute, hands-on care or find energy in mentorship, scholarship, and long-horizon influence.
Questions to Ask Yourself
How Nurse Educator Salaries Compare Across Settings and States
Salary is one of the first questions nurses ask when weighing an educator career, and the answer depends heavily on where you live and which role you're comparing against. The table below places postsecondary nursing instructor median pay alongside registered nurse and nurse practitioner medians in the same state, all drawn from BLS data. Keep in mind that BLS figures for postsecondary educators reflect base academic salary; they do not capture the overtime, night shift differentials, weekend premiums, and holiday bonuses that can significantly inflate a bedside RN's actual take home pay. That nuance matters when you're doing an honest side by side comparison.
| State | Nursing Instructor Median | Registered Nurse Median | Nurse Practitioner Median |
|---|---|---|---|
| California | $99,010 | N/A | $166,610 |
| Texas | $97,610 | $90,010 | $129,880 |
| New York | $93,640 | N/A | $145,390 |
| Florida | $83,940 | $82,850 | $129,010 |
| Illinois | $78,870 | $86,410 | $128,620 |
| Pennsylvania | $79,920 | $87,610 | N/A |
| Colorado | $80,440 | $96,520 | $129,750 |
| North Carolina | $78,740 | $81,860 | N/A |
| Wisconsin | $79,810 | $86,070 | $128,580 |
| Montana | $84,550 | $81,560 | $133,640 |
| Michigan | $80,740 | $85,670 | N/A |
| Virginia | $78,850 | $88,820 | N/A |
| Connecticut | $81,490 | N/A | $138,960 |
| New Hampshire | $81,260 | $96,830 | $132,440 |
| Minnesota | $78,110 | N/A | $128,570 |
| Nebraska | $79,120 | $81,020 | N/A |
| Vermont | $78,800 | $85,150 | $129,740 |
| Maine | $78,770 | $82,860 | N/A |
| Alaska | $92,050 | N/A | $145,450 |
| Nevada | $84,660 | N/A | N/A |
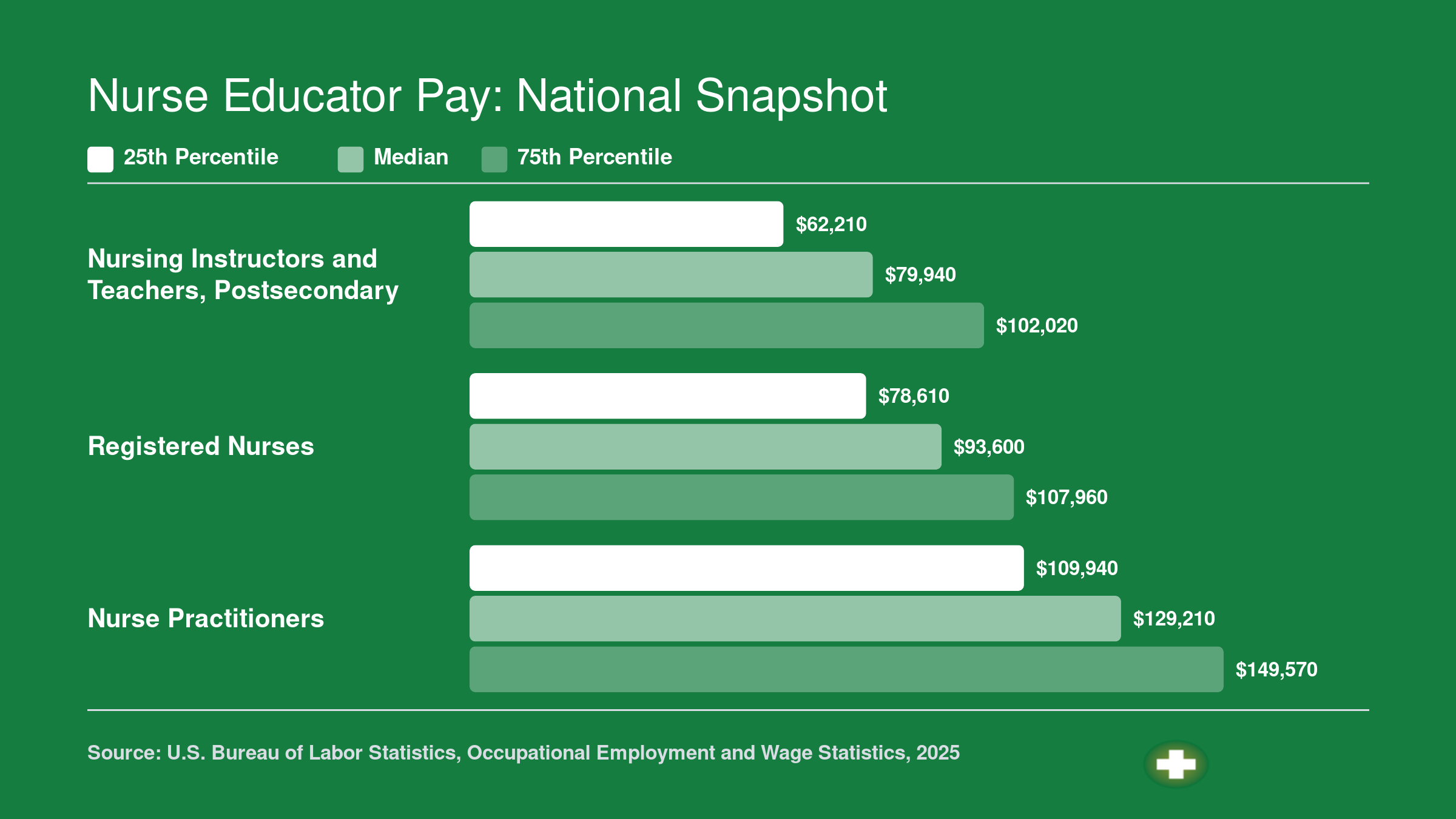
Nurse Educator Pay: National Snapshot
Nurse educator salaries sit below both RN and NP national medians, but the comparison is more nuanced than raw numbers suggest. NP compensation reflects graduate-level clinical practice and its associated demands, while academic nurse educator packages often include tuition remission, generous retirement contributions, and flexible summer schedules. When you factor in those non-salary benefits, the effective gap narrows considerably.
Types of Nurse Educator Roles: Academic, Clinical, and Beyond
Nurse educator is not a single job title; it is a career lane with several distinct tracks, each shaped by the setting you work in, the learners you teach, and how close you stay to the bedside. Understanding the four main pathways, plus a handful of newer roles, helps you match your clinical strengths and personal motivations to the right position.
Academic Faculty at Universities and Community Colleges
Full-time academic faculty teach didactic and clinical courses in BSN, ADN, or graduate nursing programs. Tenure-track positions typically require a doctoral degree (PhD or DNP), and the work blends classroom instruction with scholarly research, curriculum development, and committee service. Nurses drawn to this lane often want to shape the profession at scale, publishing research and mentoring the next generation of clinicians. Salaries for full-time postsecondary nursing instructors generally follow the BLS data for that occupation category, which tends to sit below what experienced bedside nurses earn in high-acuity settings. For a closer look at pay across settings, see our breakdown of highest paid nurse educator roles.
Clinical Educator and Staff Development Specialist
Hospital-based clinical educators (sometimes called staff development specialists or nursing professional development practitioners) design orientation programs, run skills competency days, and keep unit staff current on evidence-based protocols. Because these roles live inside health systems, compensation often mirrors bedside RN pay scales and may actually exceed them once shift differentials, certification bonuses, and overtime eligibility are factored in. If your main motivation is staying close to patient outcomes while teaching, this is the track that keeps one foot firmly on the unit floor. You can learn more about how these professionals interact with patients in our guide on nurse educators work with patients.
Simulation Lab Coordinator
Simulation coordinators manage high-fidelity mannequin labs, design scenario-based learning experiences, and debrief students or staff after each run. The role blends technical skill with pedagogical creativity. You will spend your days programming patient scenarios, troubleshooting equipment, and coaching learners through clinical decision-making in a zero-risk environment. Many simulation positions sit within academic programs, but a growing number of hospitals now maintain their own sim centers for ongoing staff training.
Online and Hybrid Adjunct Instructor
Adjunct faculty teach one or two courses per term, often online or in a hybrid format, while maintaining clinical employment elsewhere. This is a common entry point for nurses testing whether education feels like the right fit. Adjunct pay is typically per-credit or per-course and varies widely by institution, so it is worth asking about compensation structures before committing.
Emerging Roles Worth Watching
The educator landscape is expanding beyond traditional classrooms and hospitals. A few newer niches are worth noting:
- Continuing education program developer: Creates accredited CE modules for nurses seeking license renewal or specialty certification.
- Nursing informatics educator: Trains clinical staff on electronic health record systems, data analytics tools, and emerging health technologies.
- NCLEX prep curriculum designer: Builds review courses, question banks, and adaptive study plans for licensure exam candidates, often in partnership with publishing companies or test-prep platforms.
These roles reward nurses who combine teaching instincts with expertise in technology, regulatory standards, or content design. They also tend to offer remote-friendly schedules, which can be a deciding factor for nurses ready to step away from shift work entirely.
No matter which lane appeals to you, the common thread is this: every nurse educator role lets you multiply your clinical knowledge by passing it on, whether that happens in a lecture hall, a simulation bay, a hospital conference room, or a laptop screen.
How to Test Your Fit Before Committing to an MSN
Some nurses dive straight into an MSN program, but others map out a more cautious route, testing the educator role first through small, low-commitment experiences. The second path costs little, clarifies your decision, and builds a CV that strengthens any future application.
Low-Risk Ways to Explore the Educator Role
- Precept nursing students: Volunteer to mentor a student during a clinical rotation. Precepting mimics the day-to-day rhythm of guiding learners, giving feedback, and balancing patient care with teaching.
- Guest-lecture at a local program: Many nursing schools welcome practicing RNs to deliver a single class session on a specialty topic. You get a taste of classroom management, slide preparation, and student Q&A without a multi-week commitment.
- Lead a hospital in-service or skills workshop: Work with your unit educator to design and present a short session on a new protocol, device, or procedure. This tests your comfort with public speaking and your ability to distill complex information for peers.
- Apply for an adjunct clinical instructor role: Most community college and university programs hire BSN-prepared nurses to supervise clinical groups. You remain in the patient-care environment while shifting your primary focus from direct care to coaching students. Understanding the clinical nurse educator role can help you decide whether this path suits you.
Personality Traits That Predict Success
- Patience with repetition: Learners need to hear the same concept multiple times in different ways. If repeating explanations without visible frustration feels natural, you have a core educator strength.
- Comfort with public speaking: Giving calm, clear instructions to a group, whether it is five students around a bed or thirty in a lecture hall, is a daily demand.
- Ability to give constructive feedback: Moving a student from 'not yet safe' to 'safe' requires specific, actionable critique delivered with empathy. If you already enjoy coaching new graduates on your unit, that instinct transfers directly.
- Tolerance for ambiguity: Grading written work, evaluating clinical judgment, and managing student expectations rarely have black-and-white answers. Comfort with nuance protects against burnout.
Why Precepting Should Be Your First Move
Precepting is the closest analog to the full educator role. You assess a learner's current ability, plan incremental skill-building, and evaluate progress, all while managing a patient assignment. Most hospitals already maintain a structured preceptor program, so ask your manager about the next training cohort. Even a single semester with a student can reveal whether teaching energizes or exhausts you, and it tells admission committees that you have been intentional about the career shift. If precepting confirms your interest, you may also want to separate common nurse educator misconceptions from reality before applying.
Testing your fit does not delay your timeline; it de-risks it. A short trial reveals more than any amount of internet research, and the experience itself becomes the evidence you need to write a compelling MSN application.
Related Articles
Honest Trade-Offs: Challenges Nurse Educators Face
Choosing nursing education often means accepting a significant pay cut compared to bedside roles, and the financial gap extends beyond base salary to the loss of shift differentials, overtime, and per-diem bonuses that can add thousands of dollars to a clinical nurse's annual take-home pay. According to national data from the American Association of Colleges of Nursing and salary analyses published by the National Institutes of Health, nurse educators earn on average $18,346 less than staff nurses working at the bedside, $19,863 less than charge nurses, and $27,526 less than nurse managers.1 These figures reflect 2022 salary comparisons and do not account for the premium pay structures available in clinical settings: night and weekend shift differentials, overtime at time-and-a-half, and crisis or high-demand bonuses. When those extras are factored in, the real compensation gap can exceed $20,000 annually.2 A clinical nurse earning $80,000 with shift premiums may step into a faculty position paying $50,000 or less, particularly at community colleges or in non-tenure-track adjunct roles. For a deeper look at pay-related assumptions, see our breakdown of common nurse educator salary myths.
Publish-or-Perish Pressure and Administrative Overload
At research universities and institutions pursuing higher Carnegie classifications, new faculty face the expectation to publish regularly in peer-reviewed journals, secure grant funding, and contribute to the institution's research profile while simultaneously teaching full course loads. This publish-or-perish culture adds hours of unpaid work each week and becomes a major source of stress for educators who came from clinical backgrounds with little research training. Beyond scholarship, the day-to-day administrative burden is heavy: grading clinical evaluations, documenting student performance for accreditation reports, serving on curriculum committees, preparing for site visits from accrediting bodies such as the Commission on Collegiate Nursing Education, and revising course materials to meet evolving standards. Many faculty report that the time spent on committee service and accreditation preparation rivals or exceeds the hours devoted to actual teaching.
Student Incivility and the Emotional Cost of Failing Students
Student incivility, ranging from classroom disruptions and disrespectful communication to formal grievances and threats, is a documented and under-discussed stressor in nursing education. Faculty must manage students who challenge grades aggressively, bypass professional boundaries, or react with hostility to constructive feedback. More difficult still is the emotional labor of failing a student who is not clinically safe. Nurse educators carry the dual responsibility of gatekeeping the profession and supporting learner development, and dismissing a student from a program, even when patient safety demands it, weighs heavily on faculty who entered teaching to help others succeed.
Academic Politics and Career Ceilings
Academic politics, particularly around tenure and promotion decisions, can feel opaque and contentious to nurses accustomed to the clarity of clinical hierarchies. Non-tenure-track positions, which now comprise the majority of faculty appointments at many institutions, offer limited job security and fewer opportunities for advancement. According to AACN data, over 80 percent of current nursing faculty vacancies require or prefer a doctoral degree, and master's-prepared educators often hit a career ceiling quickly without further education.3 Pursuing an affordable online nurse educator PhD or affordable nurse educator DNP programs can help bridge that gap, though the time commitment is significant. The average age of master's-prepared faculty is in their 50s, and doctoral faculty average in their 60s, reflecting the long timelines required to build competitive academic credentials and the reality that many nurses pursue education roles later in their careers.3
In 2024, U.S. nursing programs turned away more than 80,000 qualified applicants because they lacked enough faculty to teach them. With a national faculty vacancy rate of 7.2% in 2025, schools are struggling to fill seats even as demand for nurses climbs.
The Nursing Faculty Shortage: Why Educators Are Needed Now
More than 1,600 full-time nursing faculty positions sat vacant across the country during the 2024-2025 academic year, according to the American Association of Colleges of Nursing (AACN).1 That number is not a staffing inconvenience. It is the primary bottleneck choking the entire nursing pipeline at a time when the healthcare workforce desperately needs more graduates.
The Scale of the Problem
AACN's 2024-2025 survey counted 1,693 unfilled full-time faculty positions nationwide, with schools that reported vacancies averaging 3.63 open slots each.1 The overall faculty vacancy rate sits at 7.9 percent, rising to 9.9 percent when measured only among programs actively trying to fill positions.1 The direct consequence: nursing programs routinely turn away thousands of qualified applicants every year, not because those students lack ability, but because there are not enough instructors to teach them. For a deeper look at the data behind this nursing faculty shortage, those numbers only grow more striking at the state level.
The retirement wave bearing down on the profession makes the near-term picture even sharper. Roughly one-third of current nursing faculty were projected to retire by 2025.2 Look at the age data and the urgency becomes concrete. Doctorally prepared professors average 61.2 years old, associate professors 55.6, and even assistant professors average 49.6.2 Master's-prepared faculty show a similar pattern. Replacements are not arriving fast enough to absorb those departures.
What Is Driving the Shortage
Three structural forces keep the vacancy rate elevated year after year.
- Degree requirements: Fully 84 percent of vacant positions require a doctoral degree, which limits the eligible candidate pool to nurses willing and able to complete a PhD or DNP.1
- Salary competition: Academic salaries routinely trail what experienced nurses can earn in clinical or advanced practice roles, making the transition a financial trade-off for many.
- Demographics: An older faculty workforce means retirements will outpace new hires for the foreseeable future, widening gaps rather than closing them.
The Bureau of Labor Statistics projects faster-than-average job growth for postsecondary nursing instructors, with several thousand openings expected annually through the coming decade, driven by both new positions and the need to replace departing faculty. You can explore the full picture of nurse educator demand in our companion guide.
What This Means for You
If you are a nurse seriously weighing a move into education, the market is working in your favor. Programs competing for a thin pool of qualified candidates have real incentive to offer competitive packages, flexible scheduling, and support for faculty development. Job security in this field is genuinely strong, not just talking-point strong. Entering the educator workforce now, especially with a doctoral credential or one in progress, puts you in a position to negotiate rather than simply accept whatever is offered. The shortage that frustrates program directors is, for the right candidate, a legitimate opening.
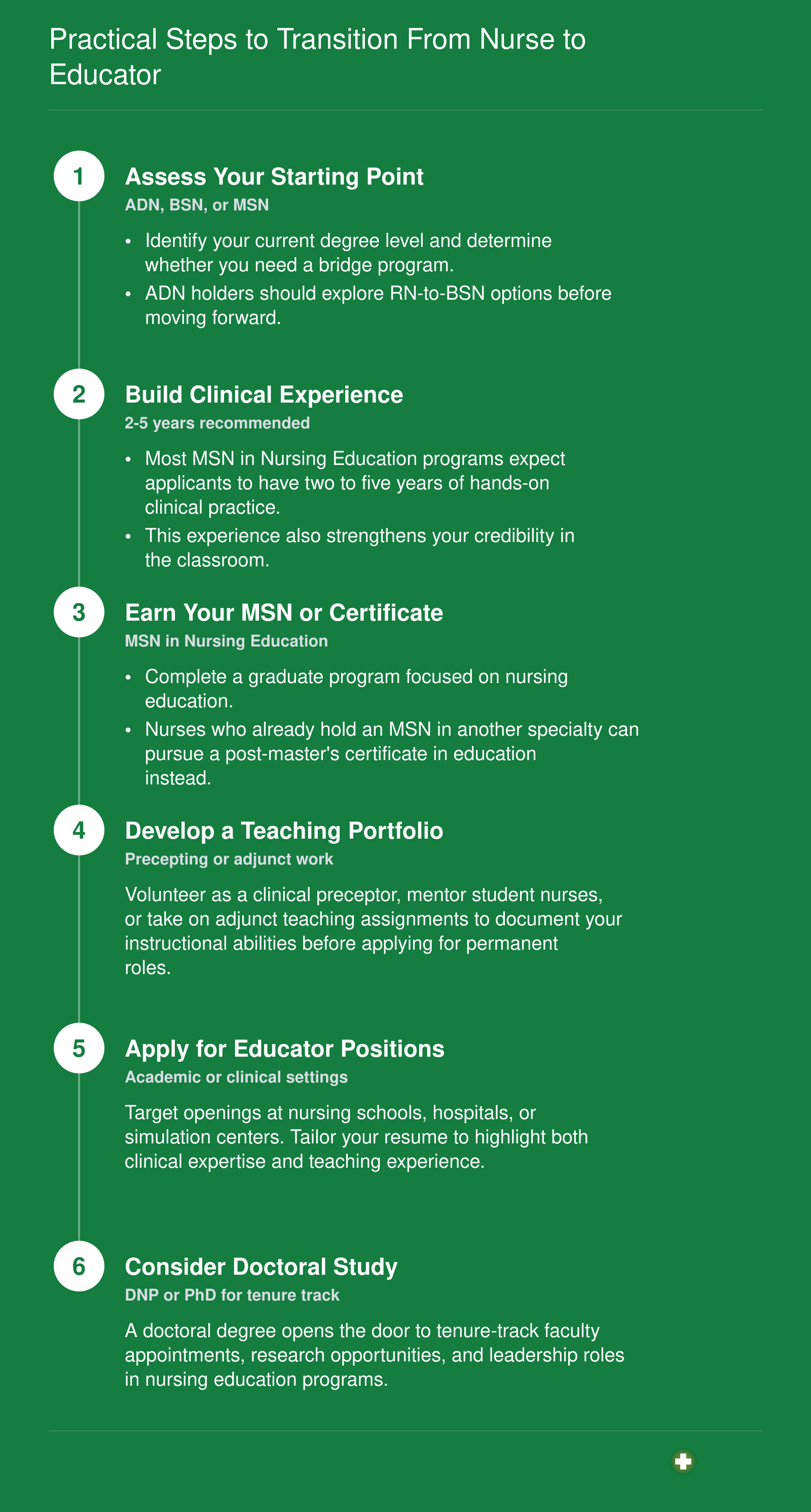
Practical Steps to Transition From Nurse to Educator
Moving from bedside care to the front of a classroom is a structured process, not a leap of faith. The timeline below maps out the major milestones. If you hold an ADN, you will likely need to complete a BSN bridge program before entering a graduate nursing education track; BSN holders can typically apply to MSN in Nursing Education programs directly.
Frequently Asked Questions About Becoming a Nurse Educator
Nurses considering the move into education often share the same set of practical questions. Below are direct, actionable answers to the topics that come up most often in advising sessions and hiring interviews.