What you’ll learn in this article…
- Simulation, flipped classrooms, and case-based learning each improve clinical reasoning scores in published nursing education research.
- About 29 percent of U.S. nursing programs were already using virtual reality for clinical training by 2024.
- You can start with one low-cost active learning technique like think-pair-share before investing in expensive simulation technology.
- A structured evaluation framework linking teaching changes to NCLEX pass rates and student outcomes builds the case for administrative support.
The National League for Nursing has urged faculty to adopt active pedagogies since its 2016 vision statement, yet surveys consistently show that lecture remains the dominant method in most programs.
Simulation-based learning, flipped classrooms, team-based models, and AI-driven case exercises are reshaping the classroom, backed by a growing body of research. Major accrediting bodies now expect programs to demonstrate these innovations. The front line of change is not the evidence base. It is the practical challenge of integrating new strategies into a curriculum that already feels overloaded, a reality compounded by the ongoing nurse educator shortage affecting programs nationwide.
Didactic Vs. Clinical Teaching in Nursing: What's the Difference and Why It Matters
The divide between classroom theory and bedside practice represents nursing education's oldest tension, and innovative teaching strategies exist precisely to close that gap. Understanding how didactic and clinical teaching differ across key dimensions helps you design learning experiences that prepare students for real patient care rather than simply passing exams.
Defining the Two Approaches
Didactic teaching unfolds in classroom or online settings where the primary focus is knowledge acquisition. According to current National League for Nursing guidelines, effective didactic instruction now emphasizes active learning through case-based, problem-based, and team-based approaches, along with unfolding case studies and concept maps.1 The student's role centers on processing information, analyzing scenarios, and building the theoretical foundation that clinical practice requires.
Clinical teaching happens where patients are, whether at the bedside, in simulation labs, or community health settings. The American Association of Colleges of Nursing describes clinical education as structured around competency development, guided reflection, and debriefing.2 Here, students apply theory under supervision, developing hands-on skills and professional judgment through direct care experiences. If you are weighing whether to focus on one domain or the other, understanding the academic vs clinical nurse educator distinction can help clarify the path that fits your strengths.
Comparing Across Key Dimensions
- Learning environment: Didactic settings include classrooms, learning management systems, and lecture halls. Clinical settings span hospitals, clinics, simulation centers, and community sites.
- Primary goal: Didactic teaching builds knowledge and critical thinking frameworks. Clinical teaching develops competency through supervised patient care and scenario practice.
- Assessment methods: Didactic courses use exams, simulation performance, and multi-method evidence tied to progression indicators.2 Clinical evaluation relies on weekly competency-based tools, self-assessment validated by faculty, and rubric-based feedback.3
- Student role: In didactic courses, students engage as active participants in problem-solving exercises. In clinical rotations, students function as developing practitioners under faculty guidance.
- Faculty role: Didactic faculty serve as learning facilitators and co-creators of educational pathways.1 Clinical faculty act as debriefers and practice partners, often requiring specialized professional development in simulation and interprofessional education.3
Where Innovation Bridges the Gap
The strongest nursing programs do not treat didactic and clinical teaching as separate silos. Current NLN and AACN guidance calls for backward design from competencies, curriculum mapping, and shared objectives across courses.2 Classroom exercises can mirror clinical documentation workflows, and pre-clinical conferences connect theoretical content to upcoming patient encounters.4 Interprofessional simulation cases blend didactic concepts with hands-on practice in a controlled environment.5
Innovative strategies like simulation-based learning, flipped classrooms, and technology-enhanced instruction work precisely because they sit at this intersection. They bring clinical realism into the classroom and structured reflection into clinical rotations. When you align didactic blocks with clinical placements and use longitudinal assessment drawing from multiple evidence sources, students experience a coherent progression rather than disjointed learning fragments. That integration, more than any single technique, defines what makes nursing education curriculum effective.
Simulation-Based Learning: Building Clinical Judgment Before the Bedside
For decades, nursing programs relied almost exclusively on direct patient care hours to build clinical competency. That hands-on model remains indispensable, but it cannot guarantee exposure to the full spectrum of patient conditions, particularly rare, high-stakes emergencies like malignant hyperthermia or maternal hemorrhage. Simulation-based learning closes this gap by recreating such scenarios in controlled settings where students can practice assessment, intervention, and communication without risking patient safety. This deliberate practice transforms theoretical knowledge into clinical judgment, bridging the classroom-to-bedside transition that challenges so many new graduates.
The Evidence Behind Simulation Success
The most influential research comes from the National Council of State Boards of Nursing (NCSBN), whose multi-year simulation study followed students into practice and monitored NCLEX outcomes. Updated data through 2024 confirmed that substituting up to half of traditional clinical hours with high-quality simulation produces comparable or improved pass rates and clinical performance. Many programs that adopted this model now report first-time NCLEX pass rates climbing beyond 90%, a testament to simulation rigor when implemented correctly. Peer-reviewed studies in CINAHL and PubMed further document enhanced critical thinking scores, better time management in care delivery, and fewer medication errors during simulation-based assessments.
Aligning with National Standards
Two organizations set the bar for simulation excellence. The INACSL Healthcare Simulation Standards of Best Practice detail step-by-step criteria for simulation design, prebriefing, facilitation, debriefing, and evaluation. Adhering to these standards ensures that every simulation runs with clear learning objectives, psychological safety, and structured debriefing that deepens understanding. The NCSBN complements this with prelicensure simulation guidelines that were refined in recent policy updates to reflect evolving clinical placement challenges and advances in technology. Together, these frameworks help programs determine appropriate simulation-to-clinical ratios and outline faculty qualifications; most recommend that simulation instructors hold formal training through courses like those offered by the Society for Simulation in Healthcare. The growing demand for qualified simulation faculty also highlights the broader nursing faculty shortage affecting programs nationwide.
Implementing Simulation Across the Curriculum
Effective integration starts with mapping simulation experiences to course and program outcomes. A fundamentals course might use low-fidelity task trainers for catheter insertion, while a capstone course deploys high-fidelity manikins for unfolding sepsis scenarios. Virtual reality and augmented reality tools are gaining traction for mental health simulations and mass casualty triage, offering immersive decision-making practice without the resource demands of full manikin labs. Whatever the modality, debriefing remains the linchpin: facilitated reflection on what happened, why actions were taken, and how to improve next time. Programs that invest in faculty debriefing skills see the greatest student gains.
Measuring Impact Beyond the NCLEX
School-level data, often published in accreditation self-studies, reveal that simulation correlates with increased student confidence and employer satisfaction. Hospitals note that new graduates from simulation-heavy programs transition more smoothly to practice, requiring less orientation time in high-acuity settings. As the evidence base expands, nurse educators are finding that simulation does not merely supplement clinical hours. It actively builds the clinical reasoning and decision-making muscle that separates task-focused nurses from true critical thinkers.
Questions to Ask Yourself
Flipped Classroom and Active Learning Models That Work
The core tension in nursing education is time: there is never enough of it to cover foundational content and develop the clinical reasoning skills students actually need at the bedside. The flipped classroom addresses that tradeoff directly by shifting content delivery out of the classroom and reclaiming in-person hours for the harder work of application, analysis, and judgment.
How the Flipped Classroom Works in Nursing
In a traditional lecture, students receive information in class and are expected to apply it later, alone, at home. The flipped model inverts that sequence. Students engage with pre-recorded video lectures, assigned readings, or narrated slides before they arrive, so class time opens up for case discussions, skills practice, and problem-solving with peers and the instructor present.
This structure suits nursing education well because the profession demands higher-order thinking, not just recall. When a patient deteriorates, a nurse cannot pause and look up a protocol from first principles. Classroom time spent on application, debate, and guided clinical reasoning builds exactly the mental flexibility that kind of moment requires.
Two 2024 randomized studies support the approach. A randomized study on flipped classroom use in community health nursing found statistically significant gains in both academic performance (p = 0.005) and community nursing competence (p = 0.012), along with high reported satisfaction and engagement.1 A separate randomized controlled trial focused on patient safety training showed statistically significant improvements in patient safety competency, with positive gains in both knowledge and skill subscales and higher satisfaction scores compared to control groups.2 No large meta-analysis specific to nursing flipped classrooms has been published as of 2026, but the accumulating trial-level evidence points consistently in the same direction.
Three Active Learning Techniques Worth Using Now
- Think-pair-share: Pose a clinical scenario (for example, a patient presenting with signs of early sepsis), give students two minutes to form an independent response, then have them compare reasoning with a partner before opening a full class discussion. The peer exchange surfaces different reasoning paths students would not encounter working alone.
- Muddiest point: At the end of a unit on pharmacology or fluid balance, ask every student to write down the single concept that still feels unclear. Collect the cards, review them between sessions, and open the next class by addressing the top two or three. This takes five minutes but gives you real-time data on where comprehension is breaking down.
- Concept mapping: Rather than outlining a disease process in linear notes, students draw a visual map connecting pathophysiology, assessment findings, nursing interventions, and expected outcomes. Concept mapping is particularly effective for complex conditions like heart failure or diabetic ketoacidosis, where multiple systems interact and students need to see relationships rather than memorize isolated facts.
A Practical Starting Point
The most common mistake educators make when adopting the flipped model is trying to flip an entire course at once. The workload of recording or curating pre-class content, redesigning in-class activities, and communicating the shift to students can become overwhelming quickly. Start by flipping one unit, one that you already know generates confusion in lectures, and assess how students respond before expanding. Developing this kind of adaptable, student-centered approach is one of the qualities of a good nurse educator that distinguishes effective teaching from routine content delivery. A single well-designed flipped unit gives you evidence to evaluate the approach on your own terms before committing to a larger redesign.
Team-Based and Interprofessional Learning: Teaching Nurses to Collaborate
How do you teach nursing students to function as part of a healthcare team before they ever set foot in one? Team-based learning (TBL) and interprofessional education (IPE) provide structured frameworks that replicate real-world collaboration in the classroom, preparing students to communicate across disciplines and reduce clinical errors from day one.
What Makes Team-Based Learning Different from Group Work
Team-based learning follows a specific sequence that distinguishes it from generic group projects.5 Students first complete individual pre-class preparation, then take an individual readiness assurance test (iRAT) to verify understanding of foundational content. Immediately after, teams retake the same assessment as a group (team readiness assurance test, or tRAT), discussing answers and reaching consensus. The session culminates in application exercises where teams apply concepts to complex clinical scenarios. This structure builds social capital, clarifies roles, and fosters mutual trust, outcomes that unstructured group work rarely achieves. Students learn to articulate their reasoning, defend evidence-based choices, and negotiate decisions under time pressure, mirroring the fast-paced dialogue of a hospital unit.
Interprofessional Education: Learning With, From, and About Other Professions
Interprofessional education brings nursing students together with peers from pharmacy, social work, medicine, and other health professions to tackle shared patient cases.1 The World Health Organization has identified interprofessional collaboration as one of the most promising solutions for strengthening health systems and improving patient safety.4 The Interprofessional Education Collaborative's 2023 Core Competencies (Version 3) outline four domains: values and ethics, roles and responsibilities, interprofessional communication, and teams and teamwork.3 The updated framework now emphasizes health equity, diversity, inclusion, systems-based practice, and population health, reflecting the evolving demands on healthcare teams. When nursing students collaborate with pharmacy students on medication reconciliation or work alongside social work students to address social determinants of health, they experience the communication dynamics and role clarity essential to preventing errors and coordinating care.
Evidence links both TBL and IPE to measurable improvements in communication skills and reduced clinical errors. The American Association of Colleges of Nursing and the Agency for Healthcare Research and Quality recommend structured approaches like interprofessional education for nursing through TeamSTEPPS (originally developed by AHRQ and the Department of Defense) to teach communication and safety tools systematically.2 Studies documented through 2024 and 2025 continue to show gains in teamwork competency and interprofessional communication after IPE interventions.
Implementing TBL and IPE in Your Classroom
Designing a TBL readiness assurance test requires clarity and brevity. Limit the iRAT and tRAT to 10 to 15 multiple-choice questions covering the most critical concepts from assigned readings. Avoid obscure details; focus on principles students will apply in the application phase. Provide immediate answer feedback during the tRAT so teams learn from their discussion in real time.
Coordinating IPE sessions across departments demands early planning and administrative buy-in. Start by identifying a shared competency goal, such as care transitions or pain management, then recruit faculty champions from pharmacy, social work, or medicine. Schedule sessions during overlapping class times, use a common case template, and assign mixed-discipline teams of four to six students. Debrief together, asking each profession to articulate their unique contributions and identify communication gaps. This reflective close reinforces the IPEC competencies and prepares students for the realities of collaborative practice. Building these facilitation skills is part of what makes teaching emotional intelligence to nursing students so critical alongside interprofessional strategies.
About 29 percent of U.S. nursing programs were using virtual reality for clinical training in 2024, according to industry surveys. That number is expected to climb sharply as schools seek immersive ways to build student competence before patient contact. The technology shift is accelerating faster than many educators anticipated.
Technology-Driven Strategies: VR, AR, and AI Tools Reshaping Nursing Classrooms
Passive screen-based modules on one end, fully immersive AI-driven simulations on the other: the spectrum of technology available to nurse educators in 2026 is wider than ever, and knowing where each tool fits is key to using it well. The real shift is not just better hardware; it is the arrival of artificial intelligence that adapts in real time to each learner's decisions, filling a content gap that VR and AR alone cannot address.
VR and AR: Stepping Inside the Patient
Virtual-reality platforms such as UbiSim place students inside a headset where they assess, intervene, and communicate with digital patients in realistic clinical environments.1 Rather than watching a demonstration, the learner physically moves through a room, selects equipment, and responds to deteriorating vitals, all while the scenario branches based on their choices. Augmented-reality tools overlay anatomical structures onto physical mannequins or even a student's own arm, turning a standard lab into a virtual anatomy session that rivals cadaver dissection for spatial understanding.
Early outcome data from programs using VR simulations show improvements in clinical judgment scores and student confidence before learners ever reach a real bedside. The immersive format also lets faculty safely expose students to high-acuity events (cardiac arrest, anaphylaxis, obstetric emergencies) that they might encounter only rarely during traditional clinical rotations.
AI-Powered Tools: Where the Biggest Changes Are Happening
AI is the faster-moving frontier. Several tools are reshaping how nursing students learn and how faculty design instruction.2
- Shadow Health: Offers digital standardized patients that respond to interview questions, physical assessment maneuvers, and clinical reasoning in a conversational interface. Students practice health histories and focused exams with an AI patient whose responses adapt based on the questions asked, building diagnostic thinking one encounter at a time.
- Lippincott CoursePoint+: Functions as an AI tutor embedded within course content. It identifies knowledge gaps from quiz performance and reading patterns, then serves targeted remediation so each student works on what they actually need.
- Lippincott Ready for NCLEX: An adaptive learning platform used across US pre-licensure programs that adjusts question difficulty and topic focus in real time, mirroring the computerized adaptive testing format of the NCLEX itself.
- Nursify AI: A study platform integrated into nursing programs that uses AI to generate practice questions, explain rationales, and track mastery across content areas.
- Anthology Blackboard AI: An LMS-level integration that brings AI-assisted analytics and content recommendations directly into the learning management system many nursing programs already use.
Beyond these named platforms, AI standardized patients with adaptive branching are gaining traction. These virtual patients do not follow a static script; they escalate symptoms, add new complaints, or respond emotionally based on how the student communicates, pushing clinical reasoning in ways a multiple-choice question never could.
Generative AI is also entering the faculty toolkit. Educators are using it to draft realistic case studies, build custom NCLEX-style item sets, and generate personalized written feedback on student care plans.3 A 2025 systematic review found that AI tools in nursing education had positive effects on both knowledge acquisition and clinical reasoning, with high levels of student satisfaction reported across studies.
What National Organizations Are Saying
Both the AACN and the NLN have issued guidance emphasizing AI literacy and ethical use as core competencies for nursing graduates and faculty alike.5 The AACN's 2026 guidance stresses a "patients first" framework: any AI integration should demonstrably serve patient safety and learning outcomes, not simply digitize existing content.6 That framing is a useful anchor when you are evaluating whether a new tool belongs in your curriculum.
Addressing Faculty Concerns
Adoption across nursing programs remains rapid but uneven, and three concerns come up consistently. For educators weighing a move into the classroom, understanding what the nurse educator career advancement path looks like can help contextualize where technology skills fit into professional growth.
- Cost: VR headsets and platform licenses can strain department budgets. Start by piloting one tool in a single course before committing to a program-wide rollout, and look for institutional site licenses that reduce per-student costs.
- Learning curve: Faculty need protected time and hands-on training, not just a vendor webinar. Pair each technology adoption with a faculty development session that connects the tool to specific learning objectives.
- Pedagogical intent: The most common misstep is layering technology onto a lesson without rethinking the lesson itself. A VR scenario works best when it replaces a less effective activity (like a static case study for a high-acuity event), not when it is added on top of an already-packed schedule.
Technology should sharpen the pedagogy you have already designed, not substitute for it. When you match the right tool to a clear learning gap, VR, AR, and AI stop being novelties and become some of the most effective strategies in your teaching repertoire.
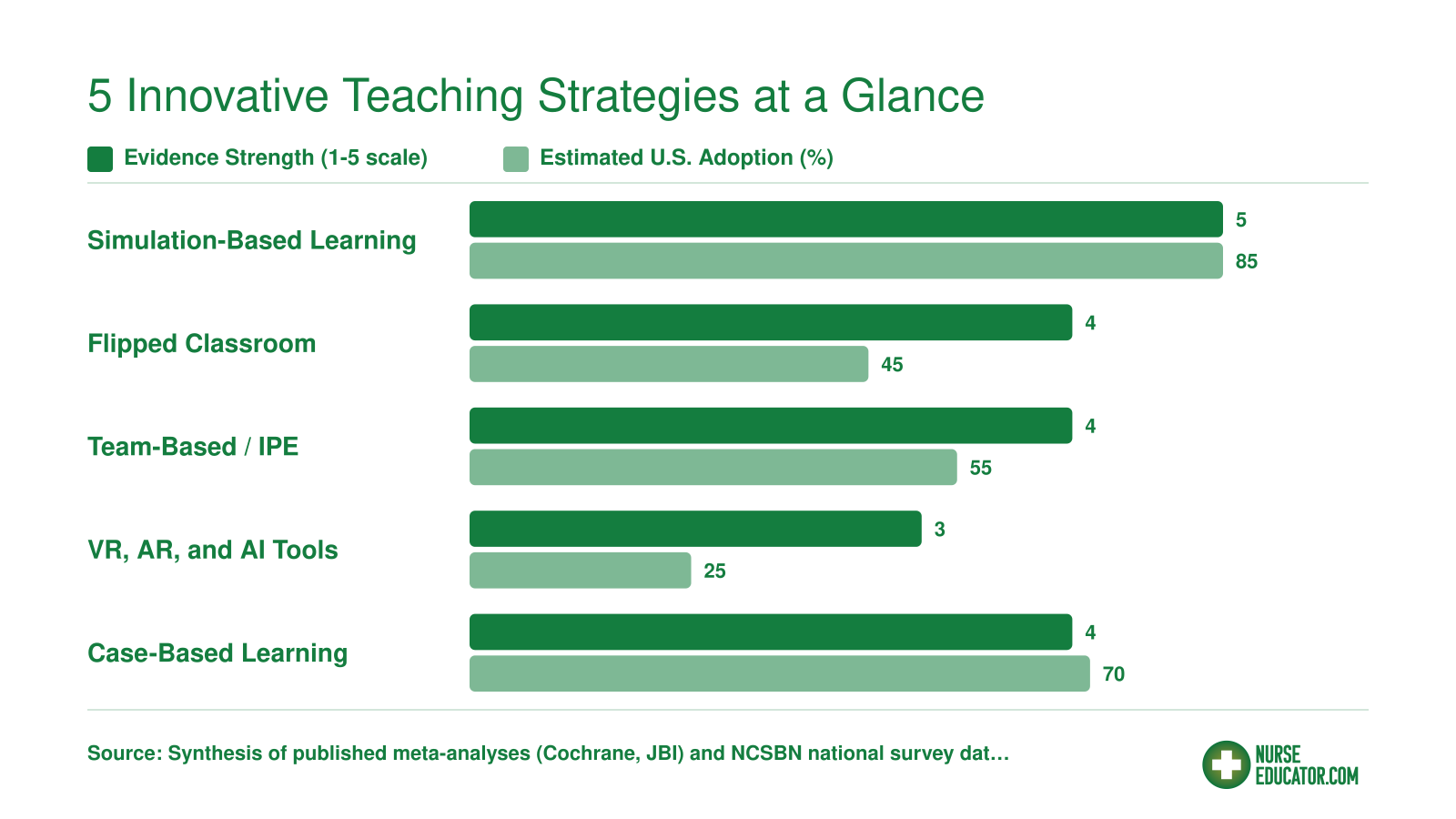
5 Innovative Teaching Strategies at a Glance
How do the most promising teaching strategies stack up? This chart compares five evidence-based approaches across two dimensions: the strength of the research supporting them (rated on a 1 to 5 scale based on published meta-analyses and effect sizes) and their estimated adoption rate among U.S. pre-licensure nursing programs.
Case-Based Learning and Clinical Reasoning Exercises
Case-based learning (CBL) is one of the most reliable ways to teach clinical reasoning because it mirrors the structured decision-making nurses perform every shift. While it shares DNA with problem-based learning (PBL), CBL offers a more guided framework: faculty present a defined patient scenario, supply targeted questions, and steer students through data interpretation rather than leaving them to discover the problem independently. That added structure makes CBL especially effective for pre-licensure students who are still building foundational knowledge and can feel lost in a fully open-ended PBL exercise.
Anatomy of a Strong Case
A well-designed case walks students through the same cognitive arc they will encounter on the NCLEX Clinical Judgment Measurement Model and, more importantly, at the bedside. Understanding how the Next Generation NCLEX affects nurse educators can help you align your cases with current exam standards. A practical template includes five stages:
- Patient presentation: A brief narrative with demographics, chief complaint, vitals, and relevant history. Keep it realistic but concise enough to read in five minutes.
- Guiding questions: Focused prompts that direct students to recognize cues and prioritize information ("Which assessment finding requires immediate follow-up?").
- Data interpretation: Lab results, imaging summaries, or medication lists that students must analyze and connect to the clinical picture.
- Nursing interventions: Students propose and justify actions, from positioning and medication administration to delegation and escalation.
- Reflection: A brief debrief asking what went well, what was missed, and how the case connects to broader course concepts.
Each stage maps directly to a dimension of clinical judgment: recognizing cues, analyzing information, prioritizing hypotheses, generating solutions, taking action, and evaluating outcomes.
Scaffolding Complexity Across a Semester
Rather than dropping students into a multi-system crisis on week one, design your case library so difficulty builds intentionally. Early in the semester, use single-system cases with clear-cut answers, such as a straightforward heart failure exacerbation. By midterm, layer in co-morbidities, conflicting lab trends, or communication challenges with the healthcare team. Toward the end of the course, introduce ethical dilemmas, ambiguous data, or interprofessional conflicts that force students to weigh competing priorities. This progression keeps learners in the productive zone of challenge without overwhelming them before they have the tools to cope.
Low-Tech to High-Tech: Accessibility Matters
One of the greatest strengths of CBL is that it does not require a six-figure simulation lab. Paper-based cases distributed as handouts or PDFs work perfectly well in a classroom, small-group study room, or asynchronous online discussion board. Faculty at resource-limited programs can build robust case libraries using free templates and real (de-identified) clinical scenarios. If you are becoming a nurse educator and transitioning from clinical practice, your own patient experiences are an excellent source of realistic case material. If your institution does have access to interactive platforms or learning management system plugins that let students click through branching patient timelines, those tools add engagement, but they are enhancements rather than requirements. The pedagogical power lives in the questions you ask and the reasoning you demand, not the technology delivering them.
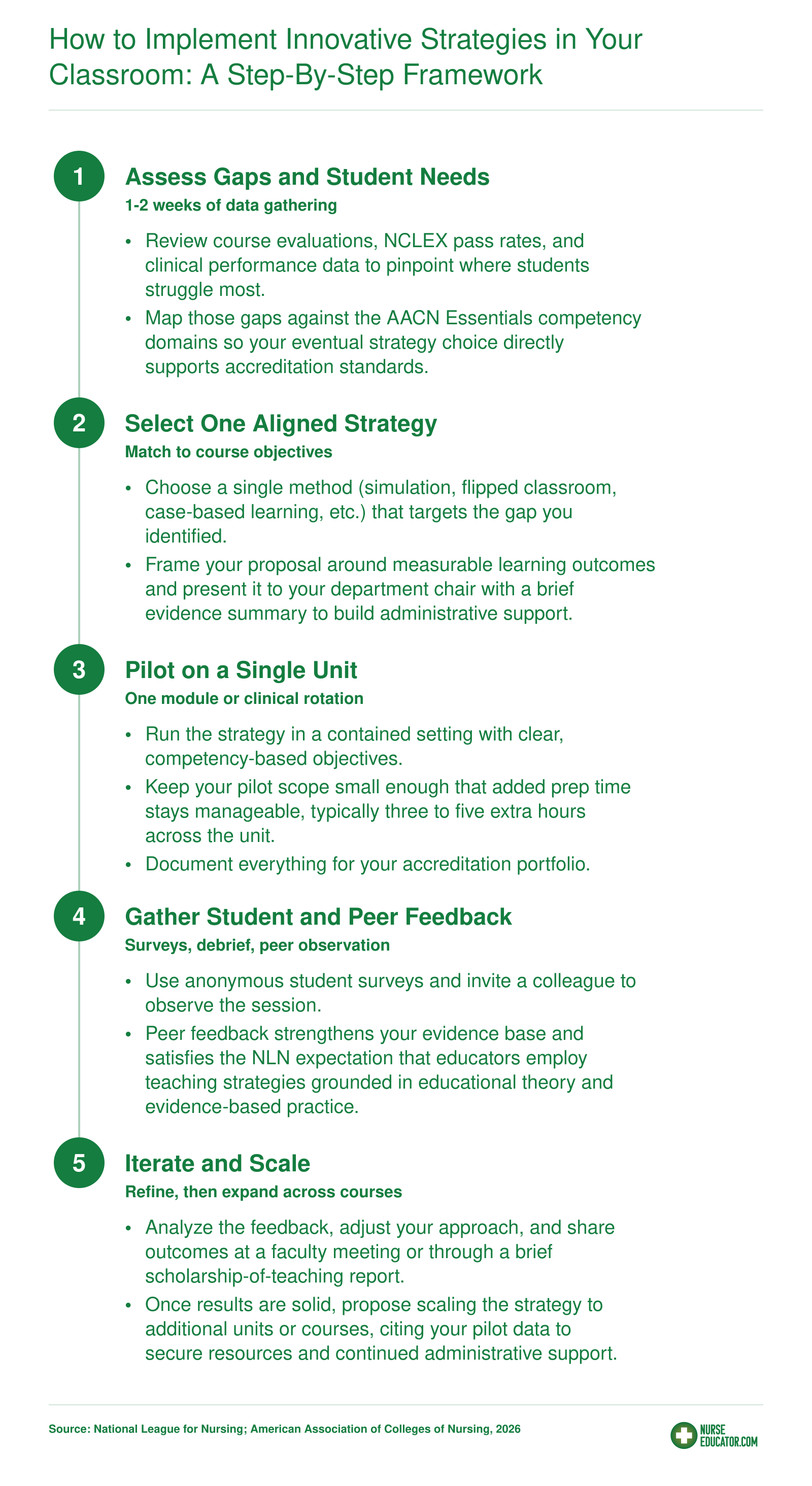
How to Implement Innovative Strategies in Your Classroom: A Step-By-Step Framework
Adopting a new teaching method does not have to mean overhauling your entire course at once. The framework below breaks implementation into manageable phases so you can demonstrate results, earn administrative buy-in, and stay aligned with accreditation expectations. The NLN's Core Competencies for Academic Nurse Educators call on faculty to function as change agents and pursue continuous quality improvement, and this process puts both competencies into action.
The biggest barrier to innovative teaching is not your budget. It is faculty confidence. You do not need a six-figure simulation lab to start. Pick one low-cost strategy, such as think-pair-share or a single flipped class unit, and try it in your next session. It costs nothing, builds your confidence quickly, and creates momentum for larger changes down the road.
Measuring the Impact of New Teaching Methods
Most nurse educators adopt an innovative strategy, watch students engage more actively, and then struggle to answer the administrator who asks: "But does it actually improve outcomes?" Closing that gap between enthusiasm and evidence is what a structured evaluation approach makes possible, and it does not require a funded research study to get there.
Start With the Kirkpatrick Framework
Adapted widely in healthcare education, the Kirkpatrick model organizes evaluation across four levels: reaction (did learners find the experience valuable?), learning (did knowledge or skill measurably improve?), behavior (are students applying what they learned in clinical settings?), and results (are program-level outcomes trending in the right direction?). Walking through these levels in sequence gives you a defensible narrative when accreditors or curriculum committees ask why you changed your approach.
The reaction level is the easiest entry point. The NLN Student Satisfaction and Self-Confidence in Learning Scale, a 13-item instrument, yields two reliable subscores: satisfaction (Cronbach's alpha 0.94) and self-confidence (0.87).1 Those numbers are strong enough to make the data credible in a faculty meeting. For simulation specifically, the NLN Simulation Design Scale collects student ratings across 20 items on a 5-point scale, covering elements like fidelity, complexity, and debriefing quality.1
At the learning level, pre/post knowledge checks, OSCE scores, and clinical placement evaluations give you concrete before-and-after comparisons. Classroom assessment techniques (CATs) such as the one-minute paper or muddiest-point exercise are low-stakes, formative tools you can deploy within a single class session to spot comprehension gaps in real time.
Tracking Competency Over Time
E-portfolios have gained traction as a way to document growth that a single exam cannot capture. Students curate artifacts across semesters, annotating how their clinical reasoning has developed. This longitudinal evidence maps cleanly onto the behavior level of the Kirkpatrick model, showing that learning transferred beyond the classroom.
For a broader institutional picture, the NLN Educational Practices Questionnaire-Curriculum (EPQ-C) provides a 22-item, 5-point scale with a content validity index of 0.90, making it a solid choice for program-wide curriculum review.1 If you are building or revising an entire nursing education curriculum, mapping the EPQ-C results to your course sequence can highlight where innovative strategies are landing and where gaps remain.
Connecting to Accreditation Metrics
National data from 2024 shows that 83% of nursing programs track course-level and program-level outcomes, 71% align evaluation to accreditation standards, and 59% specifically monitor licensure exam pass rates as outcome indicators.2 That means NCLEX pass rates, graduation rates, clinical evaluation scores, and employer satisfaction surveys are already the common language accreditors expect. Mapping your innovative strategy's results to those same metrics positions your evidence where decision-makers are already looking.
The practical takeaway: a simple pre/post quiz combined with a validated NLN scale and a semester-end NCLEX comparison is often enough to demonstrate impact. You do not need a control group or IRB approval to make a compelling case to skeptical colleagues. You need a clear question, consistent data collection, and the discipline to follow through across at least one full course cycle.
Frequently Asked Questions About Innovative Teaching in Nursing
These are some of the most common questions nurse educators ask when exploring new approaches to teaching. Each answer is designed to give you a practical starting point you can act on right away.