What you’ll learn in this article…
- The NGN launched in April 2023 with eight new item types scored using polytomous partial credit instead of all or nothing.
- Clinical judgment accounts for roughly 46 percent of entry level nursing tasks tested on the current NCLEX.
- BLS projects postsecondary nursing instructor employment will grow notably through 2034, reinforcing demand for qualified faculty.
- Programs that sustain faculty development and curriculum audits over multiple semesters report the strongest NGN pass rate improvements.
Every U.S. nursing program now prepares students for a licensure exam that looks nothing like the test many faculty members took themselves. The Next Generation NCLEX (NGN), launched in April 2023, replaced simple multiple-choice recall with layered clinical judgment scenarios and partial-credit scoring. Three years of national pass-rate data now show which instructional approaches actually translate to exam success, and which leave students unprepared.
For nurse educators, the NGN is not a distant administrative change. It directly shapes the items you write, the classroom strategies you choose, and the way you evaluate student readiness. The programs seeing the strongest results are those where faculty have moved past surface-level item familiarization and committed to teaching clinical judgment as a measurable, practiced skill. Whether you are exploring careers in nurse education for the first time or retooling a curriculum you have taught for years, understanding how the NGN works is now essential.
What Changed With the Next Generation NCLEX?
Incremental tweaks versus a fundamental redesign: the National Council of State Boards of Nursing chose the latter when it launched the Next Generation NCLEX in April 2023. Understanding why NCSBN made this decision, and what structural changes followed, helps nurse educators recognize the scope of curriculum and assessment shifts now required.
Why NCSBN Overhauled the Exam
For years, healthcare employers reported that new graduate nurses struggled with complex patient situations despite passing the NCLEX. Internal NCSBN research confirmed the concern: traditional multiple-choice items measured content recall effectively but failed to capture higher-order clinical reasoning. Meanwhile, patient-safety incident data pointed to judgment errors, not knowledge gaps, as a primary contributor to sentinel events among novice nurses. The disconnect became untenable. NCSBN concluded that entry-level competence must be defined by the ability to think through evolving clinical scenarios, not simply retrieve memorized facts.
April 2023 Launch and the Scoring Shift
The NGN rollout replaced the legacy exam structure with a model built around the Clinical Judgment Measurement Model. Rather than awarding one point per correct answer, the new format introduced partial-credit scoring. Candidates earn credit proportional to how much of the correct response they identify, which rewards nuanced reasoning while penalizing random guessing. Case-study clusters now present evolving patient vignettes that require synthesizing information across multiple screens. Item complexity increased substantially: drag-and-drop prioritization, highlight-and-select, matrix grids, and extended multiple-response formats all demand deeper cognitive engagement than the four-option recall questions that once dominated.
From Knowledge Recall to Clinical Judgment
The organizing principle of the exam shifted from "does the candidate know the right answer?" to "can the candidate recognize cues, analyze hypotheses, prioritize interventions, and evaluate outcomes?" This reframing has direct implications for how nursing programs teach and test. Courses designed around memorizing lab values or medication side effects no longer align with the competencies the licensure exam assesses. For faculty weighing whether the classroom is the right next step, these shifts also reshape what being a nurse educator looks like day to day.
Post-NGN Pass-Rate Trends: 2023 to 2025
Early data showed an initial surge in pass rates as programs intensified test-prep efforts, followed by a normalization phase.1 In 2023, the first-time pass rate for U.S.-educated NCLEX-RN candidates reached 88.6 percent nationally.2 By 2025, the all-candidates rate (including repeat and internationally educated test-takers) settled at 69.1 percent nationally, while first-time U.S.-educated PN candidates held steady at 86.6 percent.1 Repeat U.S.-educated RN candidates passed at a notably lower 52.7 percent, highlighting the stakes for students who struggle with clinical-judgment competencies the first time.1 The widening gap between first-time and repeat candidates is one reason the nursing faculty shortage matters so much: programs need experienced educators who can teach judgment, not just content.
These numbers underscore why adaptation cannot wait. Programs that have not integrated NGN-aligned pedagogy and assessment risk widening the gap between their graduates and the exam's expectations.
NGN Item Types Every Nurse Educator Should Know
Eight new item types now drive the clinical judgment focus of the Next Generation NCLEX, and each one uses polytomous partial-credit scoring rather than the all-or-nothing logic that defined the legacy exam.1 If your test bank still rewards students only for getting the entire question right, your assessments are no longer mirroring what licensure looks like.
The Eight Item Types at a Glance
NCSBN built these formats to measure the layered reasoning nurses use at the bedside.2 Each one targets a different slice of the Clinical Judgment Measurement Model:
- Extended drag-and-drop: Students pull response options into blanks or answer targets to complete a clinical statement. Correct placements earn credit, and incorrect placements may reduce the score depending on the keyed answer set.
- Cloze (drop-down): Embedded drop-down menus inside a sentence or scenario let candidates fill in clinical decisions. When multiple blanks appear, each correct selection contributes independently to the item score.
- Matrix multiple response: A grid where more than one cell per row can be correct. Students earn credit for each correctly identified cell, so partial accuracy still yields partial points.
- Matrix multiple choice: A grid where each row has a single best answer across a fixed set of options. Credit accumulates row by row.
- Enhanced hot spot: Candidates highlight relevant text in a chart, record, or image, such as abnormal lab values in a flow sheet. Each correctly selected element adds to the polytomous score.
- Bow-tie: A central problem with cause, action, and outcome options branching left and right. Rationale-based scoring awards points for each logically matched link, even if not every choice is correct.
- Trend: Sequential data (vitals, labs, status changes) presented over time, with multiple response points reflecting how the patient is evolving.
- Unfolding case studies: A patient scenario that develops across roughly six linked questions, with later items building on earlier findings. Points distribute across the case rather than collapsing into one verdict.
Why the Scoring Shift Matters for Faculty
NGN uses three scoring models: 0/1, +/- (where wrong answers can subtract), and rationale scoring (used in bow-tie items). That means item writing in your course exams now has to account for how partial credit is keyed, not just which option is correct. Faculty who also hold certified nurse educator credentials will recognize this as a fundamental shift in assessment design philosophy.
When you rebuild a quiz, ask whether each question rewards the reasoning steps a nurse actually takes, or whether it still treats clinical judgment as a single yes/no decision. The item types are the surface; the scoring philosophy is the real change.
Questions to Ask Yourself
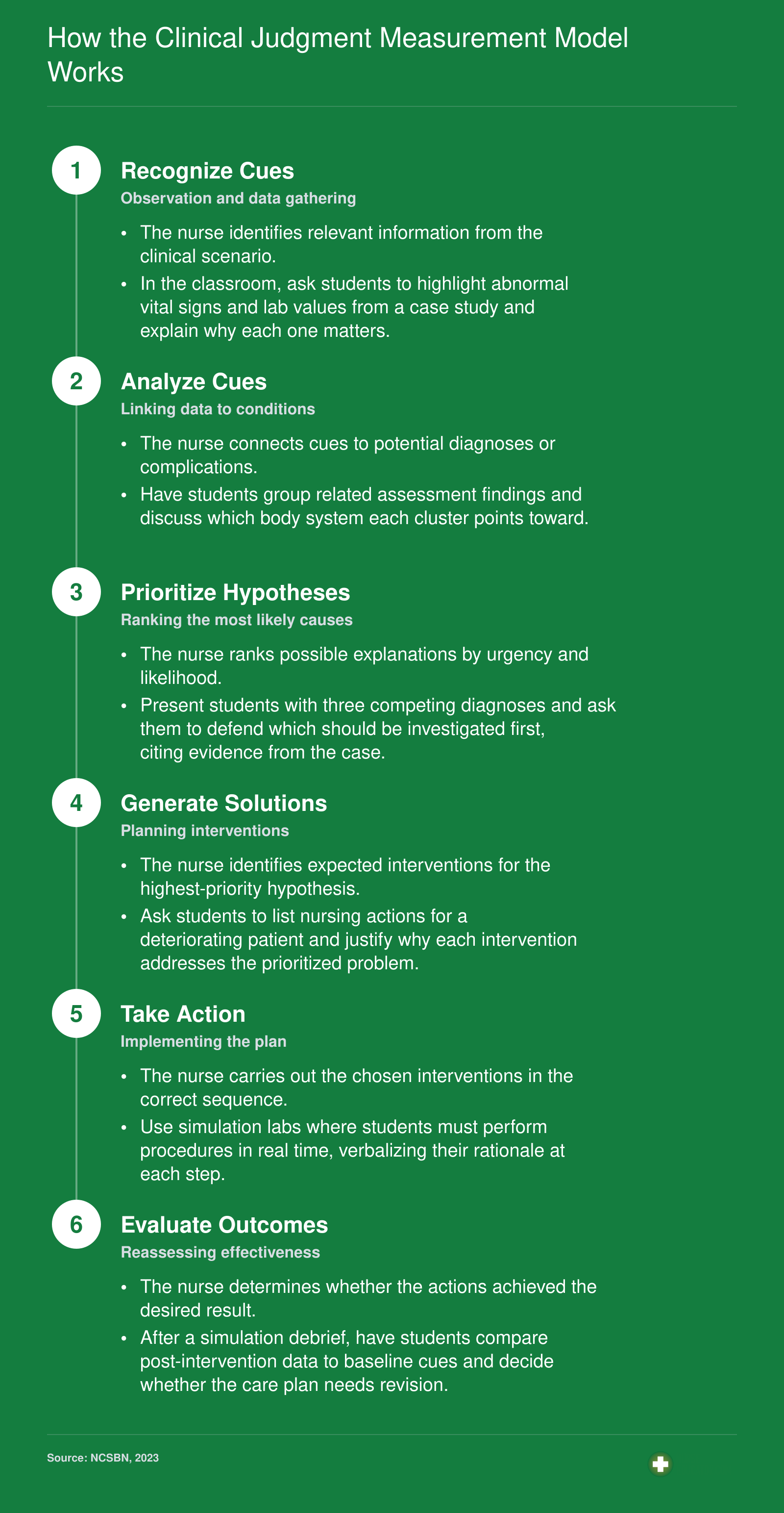
How the Clinical Judgment Measurement Model Works
The NCSBN's Clinical Judgment Measurement Model is a layered measurement framework, not a replacement for the nursing process. Three surrounding layers (Client Needs, Environment, and Individual) shape every test item by contextualizing the clinical scenario from broadest context down to the specific nurse. Inside those layers, six cognitive operations form the sequential core that NGN items are designed to measure.
Teaching Strategies That Build Clinical Judgment
Clinical judgment now accounts for 46 percent of entry-level nursing tasks, making it the single most tested competency on the NGN.1 Faculty who embed deliberate clinical judgment practice into every course give students a measurable edge. The strategies below move from high-yield, resource-intensive approaches to low-cost daily habits you can start tomorrow.
Unfolding Case Studies: The Highest-Yield Strategy
An unfolding case study presents an evolving patient scenario across time, forcing students to recognize new cues, revise hypotheses, and reprioritize actions as conditions change. A 2026 quasi-experimental study found that students exposed to unfolding cases outperformed peers on cue recognition and prioritization tasks when assessed with the Lasater Clinical Judgment Rubric.2 Structure matters: begin with a focused chief complaint in the first semester, then layer in comorbidities, family dynamics, and system failures as students advance. By the final clinical course, cases should mirror the complexity of NGN bowtie or trend items, where learners must synthesize data from multiple time points.
High-Fidelity Simulation and Structured Debriefing
Simulation hours alone do not guarantee clinical judgment gains; the debrief is where learning solidifies. A 2023 systematic review confirmed that simulation paired with structured debriefing protocols targeting specific Clinical Judgment Measurement Model operations (recognizing cues, analyzing cues, prioritizing hypotheses, generating solutions, taking action, evaluating outcomes) produced significant improvements on the Lasater Clinical Judgment Rubric and similar instruments.3 Video-assisted debriefing, in particular, helps students see gaps in their own reasoning they might otherwise miss.1
Integrate simulation at least twice per clinical course, and train faculty to ask CJMM-aligned questions during debrief: "What cue prompted you to change your hypothesis?" or "How did you know your intervention was working?"
Socratic Questioning and Think-Aloud Protocols
You do not need a simulation center to build clinical judgment. Socratic questioning and think-aloud protocols cost nothing and fit any classroom. A 2022 doctoral project using discourse analysis showed that guided questioning improved clinical judgment rubric scores when instructors pressed students to articulate each reasoning step.4
Here is a concrete example: during medication calculation practice, pause the class and ask one student to verbalize every mental step aloud, from verifying the order to double-checking units. Classmates listen, then identify where the reasoning could break down. This simple routine surfaces hidden assumptions and reinforces the analyze-cues operation of the CJMM. For more ways to keep students engaged, explore innovative teaching strategies in nursing education.
Reflective Journaling and Concept Mapping
Metacognitive tools help students internalize the final CJMM operation: evaluate outcomes. Reflective journaling after clinical shifts prompts learners to ask, "Did my intervention achieve what I expected? What would I do differently?" A 2024 integrative review found that concept mapping increases deep learning and facilitates clinical judgment by making invisible thought processes visible.5 Assign post-simulation concept maps that trace a patient's trajectory from initial cues through outcomes, and provide feedback on the logical connections students draw.
NGN-Style Formative Assessments as Teaching Tools
Partial-credit practice questions are not just evaluation instruments; they are learning experiences. When students see that selecting three correct cues earns more credit than selecting one, they learn to weigh evidence carefully rather than guess. Build low-stakes NGN-style quizzes into weekly modules and review scoring rationale in class. This approach normalizes the item formats and reduces test anxiety before high-stakes exams. Faculty looking to deepen their pedagogical toolkit may also consider how teaching emotional intelligence to nursing students complements clinical judgment development.
NGN Remediation: Supporting At-Risk Students
The shift to the Next Generation NCLEX has exposed a remediation gap in many nursing programs: traditional content review no longer prepares students for the clinical judgment demands of the new exam. Remediation that once focused on knowledge deficits must now prioritize how students think through clinical scenarios. For nurse educators, the priority is replacing last-minute cramming with a systematic, data-driven approach that identifies struggling students early and builds the reasoning skills NGN items require.
Identifying At-Risk Students Early
The first step in effective NGN remediation is catching students before they fail. Formative assessments using NGN-style items provide early warning signals. Incorporate unfolding case studies, bow-tie items, and clinical judgment matrix questions into unit exams. Pair these with rubrics aligned to the NCSBN Clinical Judgment Measurement Model (CJMM) operations: recognize cues, analyze cues, prioritize hypotheses, generate solutions, take action, and evaluate outcomes. A student who consistently struggles with "analyze cues" or "prioritize hypotheses," for example, needs targeted help long before the final exam. Use analytics from NCLEX prep platforms to track performance by CJMM step, not just by content area.
A Tiered Remediation Framework for NGN Readiness
Remediation succeeds when it matches the depth of the student's difficulty. A tiered model allows efficient resource use while giving intensive support where needed.
- Tier 1 (Targeted Practice): Assign focused NGN-style question sets that drill the specific CJMM operation where the student scored lowest. If a student can't identify relevant cues, they practice stand-alone items with complex lab values and assessment findings. Immediate feedback explaining why cues matter is essential.
- Tier 2 (Small-Group Case Workshops): For students who fail a unit or fall below a benchmark, convene groups of four to six to work through unfolding case studies aloud. A facilitator asks "What matters most right now?" and "What would you do next?" to externalize clinical reasoning.
- Tier 3 (One-on-One Coaching): Students with persistent gaps meet with a clinical faculty coach who uses think-aloud protocols. The coach observes the student reasoning through a scenario, interrupts at decision points, and models expert thinking. This cognitive apprenticeship directly shapes how the student processes clinical information.
Shifting from Content Review to Cognitive Coaching
Drilling facts about disease processes will not close the clinical judgment gap. NGN items require layered thinking, not recall. Remediation must shift from "do you know this?" to "how would you handle this?" Replace content reconsumption assignments with clinical reasoning exercises. For example, instead of rereading a cardiac chapter, give the student a scenario where a patient's vital signs change, and ask them to articulate their next steps and rationale. This shift is uncomfortable for students accustomed to reviewing lecture slides, but it is the only pathway to improved NGN performance. Faculty who are exploring broader pedagogical approaches may find value in examples of innovative teaching strategies in nursing that complement this cognitive coaching model.
Leveraging Technology for Targeted Practice
Adaptive learning platforms and NCLEX prep tools now offer NGN-format practice with real-time analytics. Platforms like ATI, Kaplan, UWorld, and HESI include item types that mirror the new exam, such as highlight tables, trend items, and dynamic multiple response. These tools can generate individualized study plans based on CJMM performance. Use the analytics to assign remediation by domain weakness, and monitor progress longitudinally. Many also provide cohort reports that help faculty identify curriculum-level gaps worth addressing in class. For programs with limited remediation time, technology delivers efficient, data-informed practice that maximizes impact.
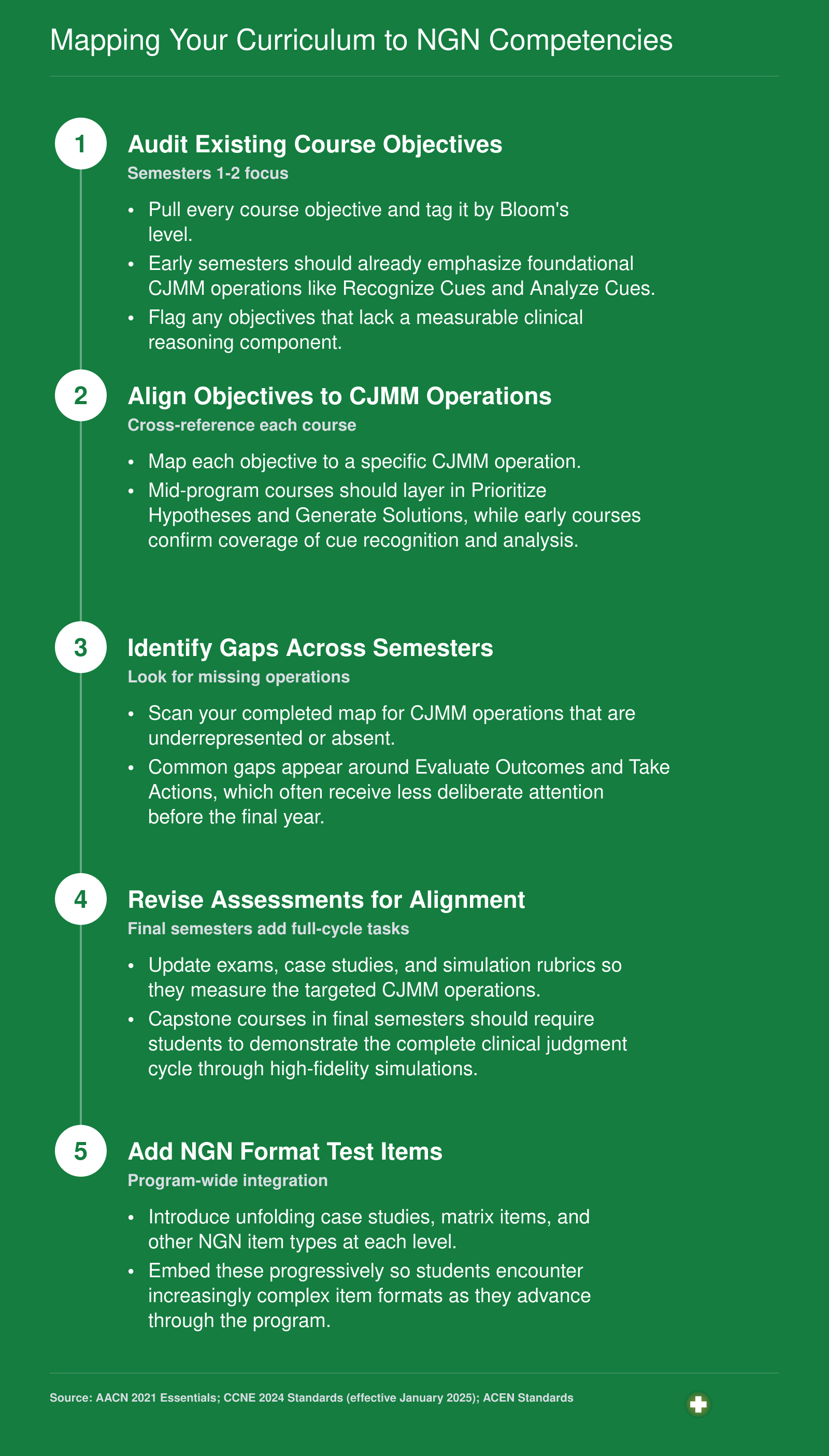
Mapping Your Curriculum to NGN Competencies
Curriculum mapping is the bridge between knowing what the Clinical Judgment Measurement Model (CJMM) demands and actually delivering it across your program. Both CCNE (aligned to the AACN 2021 Essentials, which names clinical judgment as a core competency) and ACEN increasingly expect documented evidence that programs prepare graduates for competency-based, safe-practice outcomes. Neither body offers a checklist-style template, so building your own systematic map creates the paper trail accreditation reviewers want to see.
Related Articles
Faculty Readiness: Assessing and Closing the Gap
NCSBN's own survey data found that a significant portion of nursing faculty entered the NGN era without hands-on experience writing the new item types, making structured faculty development a program-level priority rather than an individual nice-to-have.
Start With an Honest Self-Assessment
Before building a development plan, each faculty member benefits from rating their current comfort across four concrete dimensions:
- CJMM fluency: Can you explain the six cognitive skills of the Clinical Judgment Measurement Model and connect them to your course objectives without looking at your notes?
- Item-writing ability: Have you successfully written at least one each of the standalone and bowtie NGN item formats, and received peer feedback on them?
- Unfolding case facilitation: Do you regularly design or facilitate case studies that evolve across multiple patient encounters, prompting students to revisit and revise their reasoning?
- Partial-credit scoring: Are you comfortable explaining to students how partial-credit scoring differs from traditional right-or-wrong scoring, and how it affects their preparation strategy?
Honest answers reveal the specific gaps, which makes the training roadmap far more targeted.
A Four-Stage Training Roadmap
Programs that have moved through the NGN transition successfully tend to follow a layered approach:
1. NCSBN's free NGN educator resources are the logical starting point. The organization publishes case study templates, item-writing guides, and recorded webinars at no cost. 2. Peer-led item-writing workshops, held in small groups of three to five faculty, accelerate skill-building faster than solo study because colleagues can identify gaps in clinical reasoning alignment that the writer cannot see. 3. Simulation certification courses deepen the unfolding-case facilitation skills that structured workshops alone do not address. Faculty pursuing formal credentials may want to compare the CNE vs. CNEcl certification comparison to determine which pathway aligns with their teaching role. 4. Ongoing faculty learning communities, meeting monthly or quarterly, sustain momentum after initial training ends and create a space to troubleshoot live course challenges.
Reaching Adjunct and Part-Time Faculty
Adjunct and part-time instructors consistently miss synchronous development days, which creates uneven NGN implementation across a curriculum. The practical fix is a curated library of asynchronous NGN modules that faculty can complete on their own schedule, paired with a mentorship arrangement that connects each adjunct to a full-time faculty member for item-review and question-and-answer support.
This pairing model matters because adjuncts often teach high-enrollment clinical or lab sections, exactly the courses where NGN-style thinking needs to be reinforced consistently. Understanding the distinct responsibilities of the clinical nurse educator role can help programs match mentors with the adjuncts who need the most support.
Benchmarks Worth Setting
Vague goals do not move faculty development forward. Two concrete targets help programs track progress:
- By the end of Year 1, every faculty member, full-time and adjunct alike, should be able to write at least two distinct NGN item types that pass peer review.
- By the end of Year 2, every course in the nursing curriculum should include at least one NGN-format assessment, whether a standalone item set or a full unfolding case study with scored clinical judgment components.
Progress toward these benchmarks belongs in annual faculty evaluations and program review documents, not just in committee meeting minutes.
NGN readiness is not a one-time workshop. Programs that embed clinical judgment development into ongoing faculty development, peer review, and curriculum audits consistently report stronger pass rates and smoother accreditation reviews. Institutional commitment, sustained over semesters, separates successful transitions from superficial compliance.
Lessons Learned: Programs That Successfully Transitioned to NGN
Programs that openly shared their NGN transition journeys reveal actionable patterns for curriculum redesign, faculty development, and pass-rate improvement. Rather than starting from scratch, nurse educators can tap into a growing body of documented experiences, both published and informal, to see what worked, what didn't, and how timelines played out.
Where to Find Published Case Studies
Start with the National Council of State Boards of Nursing (NCSBN) website, where official research reports and NGN implementation summaries are freely available. These documents often include anonymized pilot data and faculty readiness findings. Next, browse the National League for Nursing (NLN) Education Summit archives and conference proceedings; many presentations share specific curriculum mapping timelines, item-writing strategies, and post-NGN NCLEX pass rates. Peer-reviewed journals like Nurse Educator also publish detailed accounts from individual schools. Search their back issues for terms like "NGN transition" or "clinical judgment curriculum" to find BSN and ADN programs that documented their redesign process step by step.
Key Themes from Successful Transitions
After reviewing multiple sources, several common lessons emerge:
- Start early with faculty development. Programs that began NGN item-writing workshops 12 to 18 months before the exam change reported smoother adoption and less last-minute stress.
- Integrate clinical judgment across the entire curriculum, not just in a capstone course. Successful programs wove NGN-style questions into every clinical and theory course, using unfolding case studies and stand-alone items from the first semester.
- Use data to drive remediation. Many programs tracked student performance on NGN-style assessments in ATI, HESI, or UWorld to identify at-risk learners early, then provided targeted remediation using clinical judgment frameworks.
- Share openly with peer institutions. Some community colleges and university-based programs posted their curriculum maps, sample syllabi, and even NGN readiness checklists on their public websites, resources that other faculty can adapt.
How to Connect with Program Leaders and Organizations
Not all successful transition stories make it into journals. Reach out directly to state boards of nursing, which often collect informal reports from schools in their jurisdiction. Professional associations like the American Association of Colleges of Nursing (AACN) and the NLN may share member-only resources or unpublished white papers upon request. The ongoing nursing faculty shortage makes collaboration even more critical, as programs with limited staffing benefit most from borrowing proven frameworks rather than building their own. When attending regional or national conferences, ask presenters for their slides or a brief follow-up call. Many faculty are willing to share templates and timelines if you approach them collaboratively.
Finally, keep an eye on broader outcome indicators. While the Bureau of Labor Statistics (BLS) does not track NCLEX pass rates, its employment projections and wage data, such as nurse educator salary by state, can help you gauge the long-term return on your program's NGN readiness investment. Combining these sources gives you a comprehensive picture of what it takes to support students through the Next Generation NCLEX successfully.
Nurse Educator Salaries and Career Outlook
Nursing education is one of the fastest growing segments of postsecondary teaching, and the demand for qualified faculty continues to outpace supply. According to BLS employment projections for 2024 to 2034, postsecondary nursing instructors and teachers are expected to see job growth of 16.8%, well above the average for all occupations. With roughly 8,600 annual openings projected and a significant share of current faculty approaching retirement age, nurse educators who build NGN readiness into their skill set will be especially well positioned in the job market.
| Metric | National Data (Postsecondary Nursing Instructors, SOC 25-1072) |
|---|---|
| Total Employment (2024) | 91,600 |
| Projected Job Growth Rate (2024 to 2034) | 16.8% |
| Projected Annual Openings (2024 to 2034) | 8,600 |
| National Median Annual Salary (BLS, May 2023) | $79,940 |
| National 25th Percentile Salary | $62,210 |
| National 75th Percentile Salary | $102,020 |
| National Mean Annual Salary | $87,090 |
| Programs Reporting Difficulty Filling Faculty Positions | 74% |
| Current Faculty Over Age 45 | 70% |
| Qualified Applicants Turned Away From Nursing Programs (2021) | 91,938 |
Common Questions About the NGN and Nurse Educators
Below are the questions nurse educators and nursing students ask most often about the Next Generation NCLEX. Each answer points you toward the relevant part of this article for a deeper dive.