What you’ll learn in this article…
- U.S. nursing programs turned away over 65,000 qualified applicants in a recent year largely because of insufficient faculty.
- Nurse educators earn a national median roughly 20% to 40% less than nurse practitioners or CRNAs in clinical practice.
- BLS projects about 17.9% job growth for postsecondary nursing instructors from 2023 to 2033, well above the overall teaching average.
- Federal loan forgiveness, state incentive grants, and flexible online teaching roles are expanding pathways into nurse education careers.
Hospitals post record nursing vacancies while nursing schools turn away tens of thousands of qualified applicants each year, not for lack of interest but for lack of faculty to teach them. The bottleneck is structural: retirements outpace new hires, doctoral pipelines stay narrow, and clinical salaries pull experienced nurses away from the classroom.
That gap between demand for nurses and the capacity to educate them is widening. National vacancy rates for full-time nursing faculty hover near 7 to 8%, with some states reporting double that figure. Until schools can staff enough sections, clinical workforce shortages will persist regardless of how many candidates apply. For nurses weighing whether to step into this gap, understanding why nurses become nurse educators is a practical first step toward a career that directly shapes the profession's future.
How Severe Is the Nurse Educator Shortage?
The nurse educator shortage refers to the nationwide deficit of qualified faculty teaching in nursing schools, spanning from bachelor's to doctoral programs. While many industries face workforce gaps, this shortage carries a unique weight: it directly limits the number of nurses the country can train at a time when demand for healthcare services is climbing.
A National Shortage in Numbers
According to the American Association of Colleges of Nursing (AACN), the 2025-2026 faculty vacancy rate for nursing programs across the U.S. stood at 7.2%.1 That translates to 1,588 full-time faculty positions left unfilled out of roughly 22,000 budgeted roles.2 Even more telling is the downstream effect on prospective students: in 2024, over 80,000 qualified applicants were turned away from nursing schools, with insufficient faculty cited as a top barrier to expanding enrollment.1 For a deeper look at what this means for career prospects, see our overview of nurse educator demand.
A Persistent and Worsening Trend
This isn't a one-year spike. Over the past decade (2015-2024), the average vacancy rate was 7.64%, showing that the problem has remained stubbornly high with only minor fluctuations.4 Long-term vacancies, positions that go unfilled for extended periods, numbered 471 in the latest survey, indicating that many schools struggle to fill roles even after prolonged searches.3
Impact Beyond Bachelor's Programs
The shortage reaches all levels of nursing education. While the spotlight often falls on BSN programs, graduate programs are equally strained. In 2023, more than 5,400 qualified applicants to master's nursing programs and over 4,400 to doctoral programs were turned away, frequently because there weren't enough faculty to mentor them.1 This bottleneck doesn't just delay individual careers; it curtails the pipeline of future nursing educators, researchers, and leaders. Programs like affordable nurse educator DNP programs and affordable online nurse educator MSN programs can help address this gap by making advanced education more accessible.
Regional Disparities
The burden isn't evenly distributed. In 2024-2025, the West region reported a 9.8% vacancy rate, followed by the South at 8.6% and the Northeast at 7.8%. The Midwest fared slightly better at 5.6%.3 These regional variations underscore the uneven playing field nursing schools face, often mirroring the very geographic regions already struggling to meet clinical nursing demand.
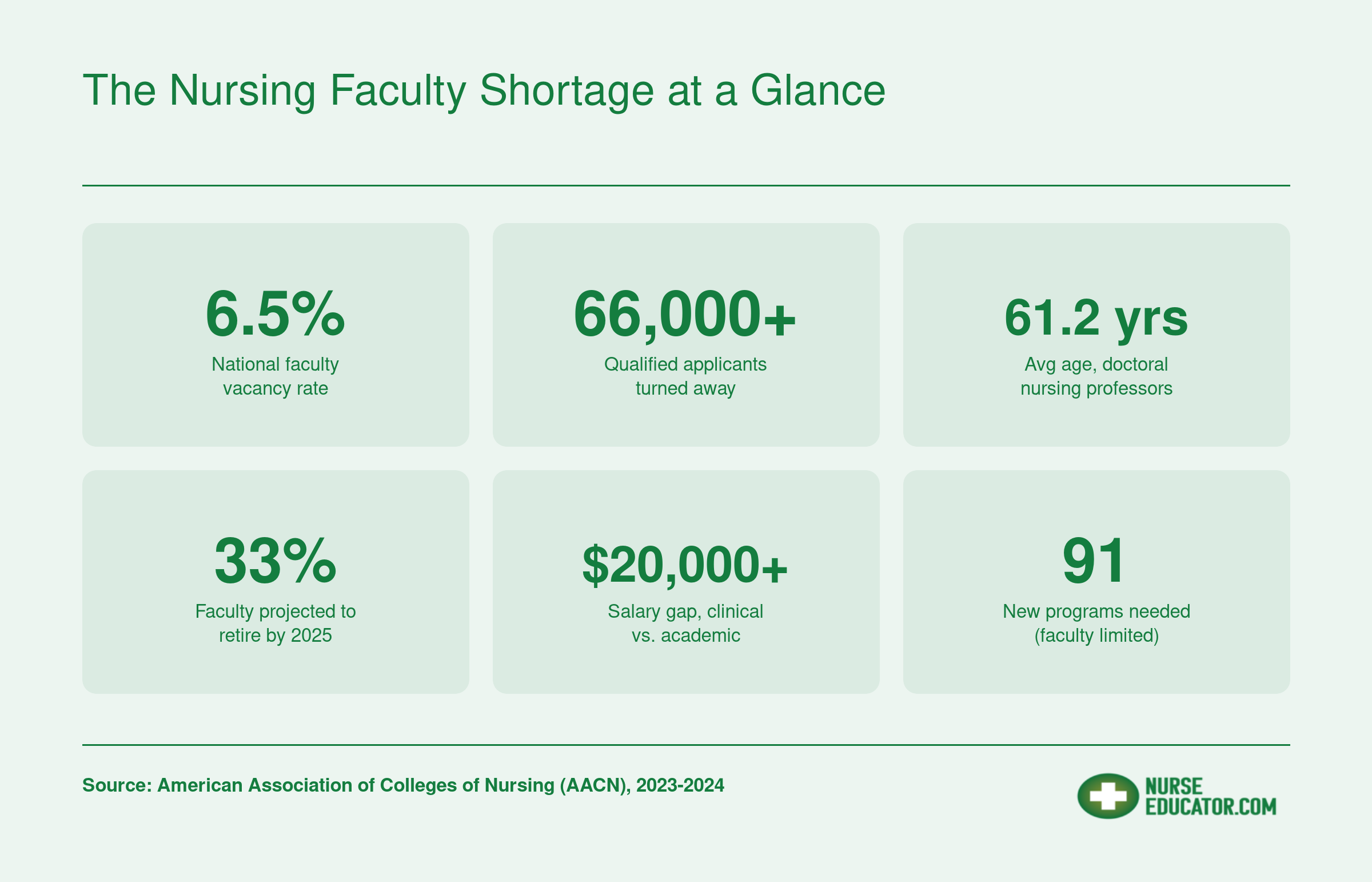
The Nursing Faculty Shortage at a Glance
These figures capture the scope and urgency of the nursing faculty crisis. Each stat underscores why recruiting clinical nurses into academic roles is essential for the profession's future.
What's Causing the Nursing Faculty Shortage?
The nursing faculty shortage is not a mystery: it is the predictable result of pay that cannot compete with clinical practice, a doctoral pipeline too small to refill the bench, and an aging workforce burning out faster than it can be replaced. Each cause feeds the next, which is why the problem has proven so durable.
The Salary Gap Makes Academia Financially Irrational
For most clinically active nurses, taking a faculty job means accepting a substantial pay cut. Nurse practitioners and certified registered nurse anesthetists working in hospitals or outpatient settings routinely out-earn assistant and associate professors by $40,000 to $80,000 or more annually, and CRNAs at the top of the market can double a faculty salary. When a master's-prepared NP can earn six figures at the bedside, asking them to teach for less while also pursuing a doctorate is a hard sell. The nurse educator salary by state comparison later in this guide shows just how wide that gap runs.
The Doctoral Pipeline Is a Bottleneck
AACN data shows that roughly 80.9% of faculty vacancies in 2025 require or strongly prefer a doctoral degree.1 PhD and DNP programs, however, are small, expensive, and slow, often taking three to five years beyond a master's. The same shortage of faculty that drives vacancies also limits doctoral program capacity, so the pipeline cannot scale quickly. In 2023 alone, nursing schools turned away 4,461 qualified applications to doctoral programs, choking off the very workforce needed to teach the next generation.1
Faculty Are Aging Out Faster Than They Are Replaced
The average full-time nursing faculty member is in their mid-to-late 50s, with many doctorally prepared professors past 60. A retirement wave is already underway, and because doctoral preparation takes years, each retirement creates a vacancy that cannot be filled on short notice. Schools end up running with empty lines for one, two, or three academic cycles. For nurses exploring faster re-entry points, a post-master's certificate in nursing education can shorten the path to the classroom.
Burnout and Workload Drive Out the Ones Who Stay
Faculty surveyed by the NLN and in studies published in Nursing Outlook and the Journal of Nursing Education consistently cite burnout, heavy workloads, and inadequate institutional support as the top reasons for leaving academia.2 Educators juggle didactic teaching, clinical site supervision, scholarship expectations, advising, and committee service, often with less administrative support than their clinical peers receive. NIH-published research has confirmed that burnout directly predicts turnover intent among nursing faculty shortage populations.3
The loop is self-reinforcing: fewer faculty means fewer graduates, which means a smaller pool of nurses who might one day return to teach. Breaking that cycle requires intervention at every link.
Questions to Ask Yourself
Nurse Educator Salaries Vs. Clinical Nursing Roles by State
The compensation gap between academic nursing roles and clinical practice is one of the strongest drivers of the faculty shortage. The table below compares state-level median salaries for health specialties teachers (the BLS category that includes nurse educators) against the 2024 national median for nurse practitioners ($129,210) and nurse anesthetists ($223,210). Keep in mind that clinical salaries vary by state as well, so the actual gap in your region may be wider or narrower than these national benchmarks suggest.
| State | Health Specialties Teachers, Postsecondary (State Median) | NP National Median (2024) | CRNA National Median (2024) |
|---|---|---|---|
| Arkansas | $178,830 | $129,210 | $223,210 |
| District of Columbia | $161,830 | $129,210 | $223,210 |
| Utah | $136,030 | $129,210 | $223,210 |
| Washington | $135,510 | $129,210 | $223,210 |
| Mississippi | $132,630 | $129,210 | $223,210 |
| North Carolina | $130,110 | $129,210 | $223,210 |
| Massachusetts | $130,000 | $129,210 | $223,210 |
| New Mexico | $129,170 | $129,210 | $223,210 |
| New York | $127,370 | $129,210 | $223,210 |
| Texas | $125,000 | $129,210 | $223,210 |
| Oregon | $124,890 | $129,210 | $223,210 |
| Colorado | $124,790 | $129,210 | $223,210 |
| West Virginia | $106,940 | $129,210 | $223,210 |
| Maryland | $106,130 | $129,210 | $223,210 |
| Iowa | $106,060 | $129,210 | $223,210 |
| Connecticut | $105,730 | $129,210 | $223,210 |
| Michigan | $104,770 | $129,210 | $223,210 |
| New Jersey | $104,760 | $129,210 | $223,210 |
| Georgia | $104,610 | $129,210 | $223,210 |
| Vermont | $104,600 | $129,210 | $223,210 |
| California | $103,500 | $129,210 | $223,210 |
| Pennsylvania | $103,400 | $129,210 | $223,210 |
| Virginia | $102,600 | $129,210 | $223,210 |
| Kansas | $99,790 | $129,210 | $223,210 |
| Minnesota | $99,620 | $129,210 | $223,210 |
| Montana | $99,490 | $129,210 | $223,210 |
| Illinois | $99,270 | $129,210 | $223,210 |
| Rhode Island | $98,640 | $129,210 | $223,210 |
| North Dakota | $98,090 | $129,210 | $223,210 |
| Tennessee | $96,030 | $129,210 | $223,210 |
| Arizona | $95,960 | $129,210 | $223,210 |
| Delaware | $94,700 | $129,210 | $223,210 |
| Nevada | $83,590 | $129,210 | $223,210 |
| Louisiana | $82,820 | $129,210 | $223,210 |
| Alabama | $82,810 | $129,210 | $223,210 |
| Indiana | $81,970 | $129,210 | $223,210 |
| Missouri | $81,920 | $129,210 | $223,210 |
| New Hampshire | $81,700 | $129,210 | $223,210 |
| Wisconsin | $81,410 | $129,210 | $223,210 |
| Nebraska | $81,380 | $129,210 | $223,210 |
| Idaho | $79,870 | $129,210 | $223,210 |
| South Carolina | $79,770 | $129,210 | $223,210 |
| Ohio | $79,130 | $129,210 | $223,210 |
| Kentucky | $78,630 | $129,210 | $223,210 |
| Wyoming | $72,700 | $129,210 | $223,210 |
| Alaska | $71,190 | $129,210 | $223,210 |
| Oklahoma | $70,730 | $129,210 | $223,210 |
| South Dakota | $68,570 | $129,210 | $223,210 |
Nurse Educator Vacancies and Demand by State
The table below combines BLS employment figures for health specialties teachers (postsecondary) with available vacancy, incentive, and policy data to help you gauge where the need for nurse educators is greatest. States in the West region carry a collective vacancy rate of roughly 9.8%, while the Midwest sits closer to 5.6%. Delaware stands out with the highest single-state vacancy rate reported at 12.3%. Several states now offer tax incentives for clinical educators, and others have introduced similar legislation. California has invested $6 million through its Residency in Education, Teaching and Instruction in Nursing initiative. Colorado and Maryland have launched substantial funding programs of their own. If you are weighing where to launch or relocate a nurse educator career, these data points can help you prioritize states with both high demand and meaningful financial support.
| State | BLS Employment (Health Specialties Teachers) | Median Annual Salary | Notable Vacancy or Demand Indicator | State Incentive or Policy |
|---|---|---|---|---|
| California | 9,030 | $103,500 | West region vacancy rate: 9.8% | $6M Residency in Education, Teaching and Instruction in Nursing program |
| Texas | 22,840 | $125,000 | Large workforce with high replacement demand | N/A |
| New York | 21,020 | $127,370 | Tax incentive legislation introduced | Tax incentive bill introduced (2024) |
| Pennsylvania | 20,030 | $103,400 | N/A | N/A |
| North Carolina | 10,530 | $130,110 | N/A | N/A |
| Massachusetts | 11,420 | $130,000 | N/A | N/A |
| Colorado | 7,400 | $124,790 | West region vacancy rate: 9.8% | Tax incentive for clinical educators; substantial state funding initiative |
| Maryland | 7,470 | $106,130 | N/A | Tax incentive for clinical educators; substantial state funding initiative |
| Virginia | 5,630 | $102,600 | N/A | Tax incentive for clinical educators |
| Georgia | 4,770 | $104,610 | N/A | Tax incentive for clinical educators |
| South Carolina | 1,090 | $79,770 | N/A | Tax incentive for clinical educators |
| Hawaii | Not reported | $48,090 | West region vacancy rate: 9.8% | Tax incentive for clinical educators |
| Delaware | 280 | $94,700 | Highest single-state vacancy rate: 12.3% | N/A |
| Oregon | 4,250 | $124,890 | West region vacancy rate: 9.8% | Tax incentive legislation introduced |
| New Mexico | 1,630 | $129,170 | West region vacancy rate: 9.8% | Tax incentive legislation introduced |
| Rhode Island | 450 | $98,640 | N/A | Tax incentive legislation introduced |
| Illinois | 7,770 | $99,270 | Midwest region vacancy rate: 5.6% | N/A |
| Ohio | 8,620 | $79,130 | Midwest region vacancy rate: 5.6% | N/A |
| Missouri | 5,860 | $81,920 | Midwest region vacancy rate: 5.6% | N/A |
| Arizona | 3,530 | $95,960 | West region vacancy rate: 9.8% | N/A |
| Washington | 4,370 | $135,510 | West region vacancy rate: 9.8% | N/A |
How the Shortage Impacts Nursing Students and Patient Care
The nursing faculty shortage is no longer a future risk; it is actively reshaping who gets into nursing school and how well-prepared those graduates are when they reach the bedside. The consequences ripple outward from the classroom to every hospital unit, clinic, and long-term care facility in the country.
Qualified Applicants Turned Away at the Door
According to AACN data, U.S. nursing schools turned away over 65,000 qualified applicants from baccalaureate and graduate programs in a single recent admissions cycle, and insufficient faculty was cited as the primary reason by the majority of responding schools. That figure does not capture the thousands more denied entry at associate-degree programs tracked separately by the National League for Nursing. Each rejected applicant represents a potential bedside nurse who never enters the pipeline, compounding the broader workforce gap year after year.
Eroding Training Quality for Those Who Do Get In
Students who secure a seat are not immune to the shortage's effects. Programs stretched thin by vacancies often respond with larger lecture sections, fewer one-on-one faculty interactions, and reduced access to clinical placement sites. When clinical slots are scarce, schools lean more heavily on simulation labs. Simulation is a valuable teaching tool, but it cannot fully replicate the complexity of real patient encounters, including the unpredictability of human responses, interdisciplinary communication under pressure, and the emotional weight of caring for someone in crisis. Teaching emotional intelligence to nursing students requires repeated, authentic patient interactions that simulation alone cannot provide. Overreliance on simulation risks producing graduates who are technically competent in controlled settings yet less confident navigating chaotic, high-acuity environments.
The Domino Effect on Patient Care
Fewer nursing graduates mean fewer nurses at the bedside, and the consequences are well documented. Hospitals operating with higher nurse-to-patient ratios consistently report longer emergency department wait times, increased rates of medication errors, and higher incidence of hospital-acquired infections. Research published in peer-reviewed journals, including landmark studies by Linda Aiken and colleagues, has found that each additional patient added to a hospital nurse's workload is associated with a measurable increase in patient mortality and failure-to-rescue rates. One widely cited study estimated a roughly seven percent rise in the odds of patient death for each additional patient per nurse.
These are not abstract statistics. They translate into preventable harm:
- Patients waiting longer for pain management, repositioning, and routine assessments.
- Higher rates of falls and pressure injuries in understaffed units.
- Greater burnout among remaining nurses, which drives more clinicians out of the profession entirely, further tightening the cycle.
A Self-Reinforcing Crisis
The pattern feeds on itself. Too few faculty leads to too few graduates, which leads to understaffed clinical settings, which leads to worse working conditions, which discourages experienced nurses from staying in practice or pursuing teaching careers. Breaking this loop requires intentional investment at the education level, something explored in the solutions section that follows. For nurses weighing a move into academia, understanding these stakes underscores why becoming a nurse educator has never been more consequential.
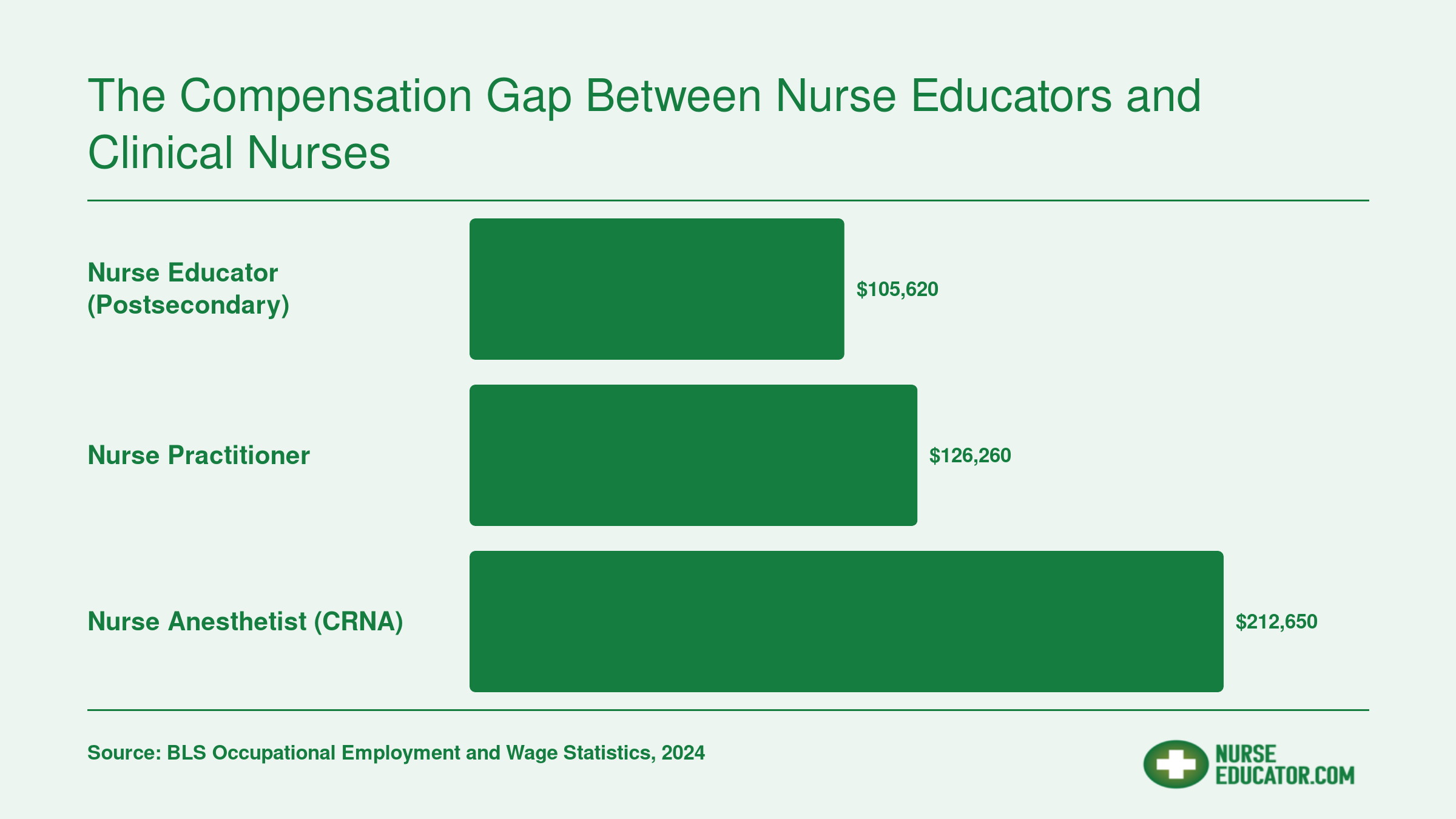
The Compensation Gap Between Nurse Educators and Clinical Nurses
One of the most persistent drivers of the nursing faculty shortage is the salary gap between academic and advanced-practice clinical roles. The comparison below puts three national median salaries side by side, illustrating why many doctorally prepared nurses choose clinical practice over teaching.
Solutions: Federal Programs, State Policies, and Institutional Strategies
Federal loan forgiveness programs remain the most direct lever for attracting nurses into faculty roles, yet uptake has consistently fallen short of available funding because eligibility requirements and service commitments create friction that generic calls for "more money" cannot solve.
NURSE Corps and Federal Loan Programs
The NURSE Corps Loan Repayment Program stands as the flagship federal incentive for prospective nurse educators. Through its Faculty Track, participants can receive 60 percent of their qualifying student loan balance canceled after a two-year service commitment, with an additional 25 percent forgiven for a third year of service (bringing the total to 85 percent).1 Eligibility requires full-time employment at an accredited school of nursing and current, unencumbered licensure.
The Nurse Faculty Loan Program takes a different approach, offering low-interest loans during graduate study rather than repaying existing debt. Participants who complete four years of full-time teaching after graduation can have up to 85 percent of their NFLP loans canceled.1 The Faculty Loan Repayment Program provides up to $40,000 in loan repayment for a two-year teaching commitment, targeting nurses from disadvantaged backgrounds.1
Despite these offerings, participation rates lag behind need. The AACN reports roughly 10,000 vacant seats in master's and doctoral nursing programs, yet fewer than half of eligible nursing schools actively promote these federal options to prospective faculty.1 Structural barriers persist: part-time instructors often do not qualify, and the commitment timeline discourages mid-career clinicians weighing opportunity costs. For nurses exploring careers in nurse education, understanding these financial incentives early can shape degree and career planning.
Legislative Momentum
The Nurse Faculty Shortage Reduction Act, introduced in January 2024 and reintroduced in January 2026 with bipartisan support from Senators Dick Durbin and Lisa Murkowski, would expand Title VIII funding specifically for faculty development.2 While the bill has not yet passed, its reintroduction signals growing congressional recognition that workforce development programs need dedicated faculty provisions rather than lumping educators into general nursing buckets.
The Department of Labor's Nursing Expansion Grant Program allocated $80 million in 2022, including a Nurse Education Professional Track designed to grow the pipeline of qualified instructors.1 Early results from grantee institutions suggest that targeted faculty recruitment embedded within broader nursing expansion initiatives outperforms standalone recruitment campaigns.
State-Level Strategies That Work
Several states have moved beyond passive recruitment into active salary intervention. Georgia's Faculty Salary Supplement program provides direct payments to nursing faculty at public institutions, partially closing the gap with clinical wages. North Carolina operates a similar supplement through its Area Health Education Centers, specifically targeting rural nursing programs where recruitment challenges are most acute.
California's Song-Brown Health Care Workforce Training Program funds nursing education sites and provides faculty development grants, with priority given to programs serving underserved communities. Texas established the Nursing Shortage Reduction Program to support faculty positions at public and private nursing schools, recognizing that capacity limits at the instructor level create downstream workforce shortages.3
These state programs share a common thread: direct salary support tied to measurable outcomes rather than block grants that institutions can redirect.
Institutional Strategies With Evidence
Practice-academic partnerships have emerged as the most promising institutional model. Joint clinical-faculty appointments allow hospitals to subsidize educator salaries while benefiting from stronger clinical training pipelines. Banner Health's partnership with Arizona nursing programs, for example, embeds faculty within hospital systems, reducing the financial burden on academic institutions while giving educators ongoing clinical exposure.
Phased retirement programs retain experienced faculty longer by allowing gradual workload reductions rather than abrupt departures. Competitive adjunct pay, while seemingly obvious, remains rare: most adjunct nursing instructors earn less per course than they would working a single clinical shift, creating a disincentive that no amount of mission-driven rhetoric can overcome.
What has not worked is broad, unfocused advocacy for "increased funding" without structural reform. Programs that simply add budget lines without addressing salary compression, clinical practice maintenance, or workload distribution tend to produce marginal gains at best. The evidence points toward targeted interventions, whether federal loan forgiveness, state salary supplements, or nursing faculty shortage solutions like practice partnerships, that directly address the economic calculus nurses face when considering a teaching career.
Career Pathways to Become a Nurse Educator: MSN Vs. DNP Vs. PHD
Choosing the right academic pathway shapes your teaching role, institutional fit, and long-term career trajectory. Three primary degrees prepare you for nursing education: the Master of Science in Nursing (MSN), the Doctor of Nursing Practice (DNP), and the Doctor of Philosophy (PhD) in Nursing. Each opens different doors.
Understanding the Three Pathways
All three pathways can lead to a nurse educator career, but they differ sharply in focus, time commitment, and scope of teaching eligibility. Here's a quick comparison.
- MSN: Focused on advanced clinical practice and education. Typically takes 2 years post-BSN. Prepares you for clinical instructor and community college faculty roles.1
- DNP: Practice-oriented terminal degree emphasizing clinical leadership and evidence-based practice improvement. Typically 3 to 4 years post-BSN or 1 to 2 years post-MSN. Qualifies you for clinical faculty, program director, and some tenure-track positions.2
- PhD: Research-intensive degree designed to produce new knowledge. Generally 4 to 6 years post-BSN or post-MSN. The traditional credential for tenure-track and research-intensive faculty roles.3
Salary expectations vary by degree, institution, and geography. Nurse educators with a doctoral degree (DNP or PhD) often earn above the national median for postsecondary nursing instructors, though the premium depends on whether the role is clinical or research-focused.
MSN: The Fastest Route to the Classroom
For a clinical nurse eager to start teaching, the MSN is the most direct path. Many programs offer a nurse educator track or concentration that blends advanced clinical content with curriculum design, assessment, and teaching practicums. Because it requires less time than a doctorate, the MSN is ideal if you want to teach in associate degree or practical nursing programs, or serve as a clinical instructor for hospital-based education.
An MSN-prepared nurse can secure adjunct or full-time clinical nurse educator role positions at many schools of nursing. While tenure-track positions at research universities typically require a doctorate, community colleges and teaching-focused institutions often hire MSN-prepared faculty for their clinical expertise. If you already hold an MSN without an education focus, a post-master's certificate in nursing education can fill the gap in as little as 12 to 18 months, adding teaching competencies without committing to a full doctoral program.
DNP: Bridging Clinical Leadership and Teaching
The DNP is increasingly accepted as a credential for academic nurse educators, especially in programs that value practice scholarship.2 DNP graduates bring deep clinical expertise and quality improvement skills to the classroom, making them strong candidates for clinical faculty and program leadership roles. Many DNP programs include coursework in evidence-based teaching, and some offer dedicated educator tracks.
In the job market, the DNP opens doors that an MSN alone may not. It qualifies you for faculty positions in BSN and graduate programs, as well as administrative roles like program coordinator or director. While it is not the traditional research doctorate, many universities now appoint DNP-prepared faculty to tenure-track lines, though this varies by institution. If your goal is to shape nursing practice through teaching and system-level change rather than original research, the DNP may be your best fit.
PhD: The Path to Tenure and Research
The PhD in Nursing is designed for those who want to generate new knowledge through scientific inquiry.3 This degree is still considered the gold standard for research-intensive academic roles and tenure-track appointments at major universities. PhD programs emphasize theory development, statistics, and research methods, culminating in a dissertation.
As a PhD-prepared faculty member, you'll typically teach at the graduate level, mentor doctoral students, and lead funded research programs. Salaries for research-active, tenured professors are generally higher than for clinical faculty, though the timeline to degree is longer. If you envision a career combining teaching, research, and academic service, the PhD is the most established route. You can explore related nurse educator career advancement options to see how each degree maps to specific roles.
Post-Master's Certificates: A Strategic Bridge
Nurses who already hold an MSN or DNP but lack formal teaching preparation can add a post-master's certificate in nursing education. These certificates focus on nursing education curriculum, instructional strategies, and assessment, and can often be completed online in 1 to 2 years. They are an efficient way to transition from practice to teaching without starting a new degree from scratch.
The Outlook for Online Nurse Educator Roles
Postsecondary nursing instructors and teachers are projected to see roughly 17.9% job growth from 2023 to 2033, according to Bureau of Labor Statistics employment projections.1 That rate far outpaces the 7% growth projected for postsecondary teachers overall during a comparable window.2 Within that expanding demand, online teaching roles represent one of the fastest-growing subsets, fueled by changes that took root during the pandemic and have since become permanent fixtures across nursing education.
Why Online Faculty Demand Keeps Rising
When COVID-19 forced nursing programs to shift didactic coursework online, many discovered that virtual delivery worked well for theory-heavy courses like pathophysiology, health policy, evidence-based practice, and nursing research. Rather than reverting entirely to in-person instruction, a large number of programs have maintained hybrid or fully online formats for these courses. The result is a steady, structural need for faculty who are comfortable teaching in digital learning environments.
This trend aligns with the broader growth of online nursing degree programs, particularly at the MSN and DNP levels, where working nurses enroll while maintaining clinical employment. Schools that want to attract and retain these students need qualified educators who can deliver rigorous content asynchronously or through live virtual sessions. If you are weighing the pros and cons of this route, exploring the benefits of online nurse educator program options is a useful starting point.
What Online Faculty Roles Typically Look Like
Online teaching positions often differ from traditional tenure-track appointments in a few important ways:
- Contract structure: Many online roles are adjunct or per-course, meaning you are hired on a semester-by-semester or course-by-course basis rather than as a salaried, full-time faculty member.
- Flexibility: Because you set your own schedule around asynchronous modules, discussion boards, and virtual office hours, online teaching fits naturally alongside part-time or even full-time clinical practice.
- Compensation: Adjunct pay varies widely by institution but is generally lower per course than what a full-time faculty member earns on a prorated basis. The tradeoff is scheduling freedom.
For clinical nurses who want to test the waters of academia without leaving the bedside entirely, an adjunct online role can serve as a low-risk entry point. You gain teaching experience, build a faculty record, and discover whether education feels like the right long-term path.
Honest Limitations
Online roles only partially address the nursing faculty shortage. Clinical rotations, simulation labs, and skills check-offs still demand in-person oversight from experienced nurse educators. No amount of virtual instruction can replace a faculty member guiding a student through their first IV insertion or patient assessment. Programs therefore need both online and on-site faculty, and the most acute shortages tend to cluster around the clinical side, a dynamic explored in more detail when comparing the academic vs clinical nurse educator tracks.
Additionally, heavy reliance on adjunct contracts can create instability for educators and inconsistency for students. Schools that lean too far into course-by-course hiring may struggle with faculty retention and continuity of instruction.
Getting Started
If you are a practicing nurse curious about teaching, consider starting with a single online course at a local or regional nursing program. Most schools require at least an MSN for didactic instruction, so verify that your credentials meet the minimum. For nurses who already hold an MSN but want a research-focused credential, an affordable online nurse educator PhD can open doors to tenure-track positions. The career pathways section of this article breaks down how MSN, DNP, and PhD degrees map to different faculty roles. From there, you can decide whether to deepen your commitment to education, pursue a doctoral degree, or continue blending clinical work and part-time teaching in a way that fits your life.
Frequently Asked Questions About the Nurse Educator Shortage
The nursing faculty shortage raises questions for nurses considering a move into education, for students waiting to get into nursing programs, and for healthcare systems feeling the downstream effects. Below are concise answers to the questions we hear most often.