What you’ll learn in this article…
- Nurse educators earn a national median near $77,000, while nurse practitioners reach roughly $126,000 according to May 2024 BLS data.
- BLS projects nursing instructor positions to grow 7% or more from 2024 to 2034, well above the national average.
- A master's degree plus the voluntary CNE certification is the most common credential path for aspiring nurse educators.
- California and Texas offer the highest state-level median salaries for postsecondary nursing instructors nationwide.
Nurse educators earn a national median salary roughly $40,000 below that of nurse practitioners, yet they report some of the highest job satisfaction rates in advanced nursing. That gap forces a real question for experienced RNs eyeing a move to the classroom: does teaching mean giving up income, clinical autonomy, or professional influence?
The answer depends on how each role stacks up across multiple dimensions. In the sections that follow, nurse educators are compared side by side with nurse practitioners, clinical nurse specialists, physician assistants, and (for broader context) physicians. The comparison spans compensation, credential requirements, daily responsibilities, career transition paths, and projected job growth through 2034.
At a Glance: Nurse Educator Vs. NP, CNS, PA, and MD
Choosing between a nurse educator career and other advanced healthcare roles means weighing very different daily realities, training investments, and scopes of practice. The table below highlights the key distinctions across five common paths that RNs and healthcare professionals consider. Keep in mind that scope of practice details, especially prescriptive authority, vary by state and practice setting.
| Nurse Educator | Nurse Practitioner (NP) | Clinical Nurse Specialist (CNS) | Physician Assistant (PA) | Physician (MD/DO) |
|---|---|---|---|---|
| MSN (minimum); DNP or PhD preferred for tenure-track faculty roles | MSN or DNP | MSN or DNP with CNS specialization | Master of Physician Assistant Studies (MPAS) | MD or DO, plus residency (3 to 7+ years) |
| Certified Nurse Educator (CNE) credential through NLN; active RN license | APRN/NP state license plus national board certification (e.g., ANCC or AANP) | APRN/CNS state license; specialty certification through ANCC or AACN | NCCPA certification (PA-C) and state license | State medical license and specialty board certification |
| Universities, community colleges, teaching hospitals, simulation labs, online programs | Outpatient clinics, primary care offices, hospitals, specialty practices | Hospitals, health systems, specialty units (e.g., cardiac, oncology) | Hospitals, outpatient clinics, surgical teams, urgent care centers | Hospitals, clinics, private practice, academic medical centers |
| No | Yes (authority varies by state; some states grant full practice authority) | Varies by state; many states grant limited prescriptive authority | Yes (under physician collaboration or supervision, depending on state) | Yes, full independent prescriptive authority |
| Curriculum design, classroom and clinical instruction, student mentorship, scholarly research, program accreditation | Diagnose and treat acute and chronic conditions, order diagnostics, prescribe medications | Evidence-based practice improvement, staff education, direct specialty patient care, systems-level outcomes | Diagnose, treat, assist in surgery, prescribe medications under a collaborative practice model | Comprehensive diagnosis and disease management, surgical and procedural interventions, independent medical decision-making |
| Approximately $79,940 for postsecondary nursing instructors | Approximately $129,210 | Often reported within the broader RN or APRN categories; BLS does not publish a separate CNS median | Reported separately by BLS; consult the latest Occupational Employment and Wage Statistics for current figures | Among the highest-paid occupations nationally; salary varies widely by specialty |
| Limited; may maintain a clinical practice role part-time or supervise students in clinical rotations | Yes, primary role involves direct patient assessment and treatment | Yes, though often combined with staff development and quality improvement responsibilities | Yes, hands-on patient care is central to the role | Yes, direct patient care is the foundation of daily practice |
Salary Comparison: What Each Role Actually Earns
Compensation is one of the biggest factors nurses weigh when choosing between education and clinical advanced-practice tracks. The table below uses national median figures from the Bureau of Labor Statistics (May 2024 Occupational Employment and Wage Statistics) alongside available salary data for clinical nurse specialists. Keep in mind that individual earnings vary widely by geographic region, employer type, and years of experience, so treat these numbers as benchmarks rather than guarantees.
| Role | BLS SOC Code | National Median Salary | 25th Percentile | 75th Percentile | Total U.S. Employment |
|---|---|---|---|---|---|
| Nursing Instructor / Postsecondary Teacher | 25-1072 | $79,940 | $62,210 | $102,020 | 74,250 |
| Registered Nurse | 29-1141 | $93,600 | $78,610 | $107,960 | 3,282,010 |
| Clinical Nurse Specialist | 29-1141 (subset) | $93,600 | N/A | N/A | N/A |
| Nurse Practitioner | 29-1171 | $129,210 | $109,940 | $149,570 | 307,390 |
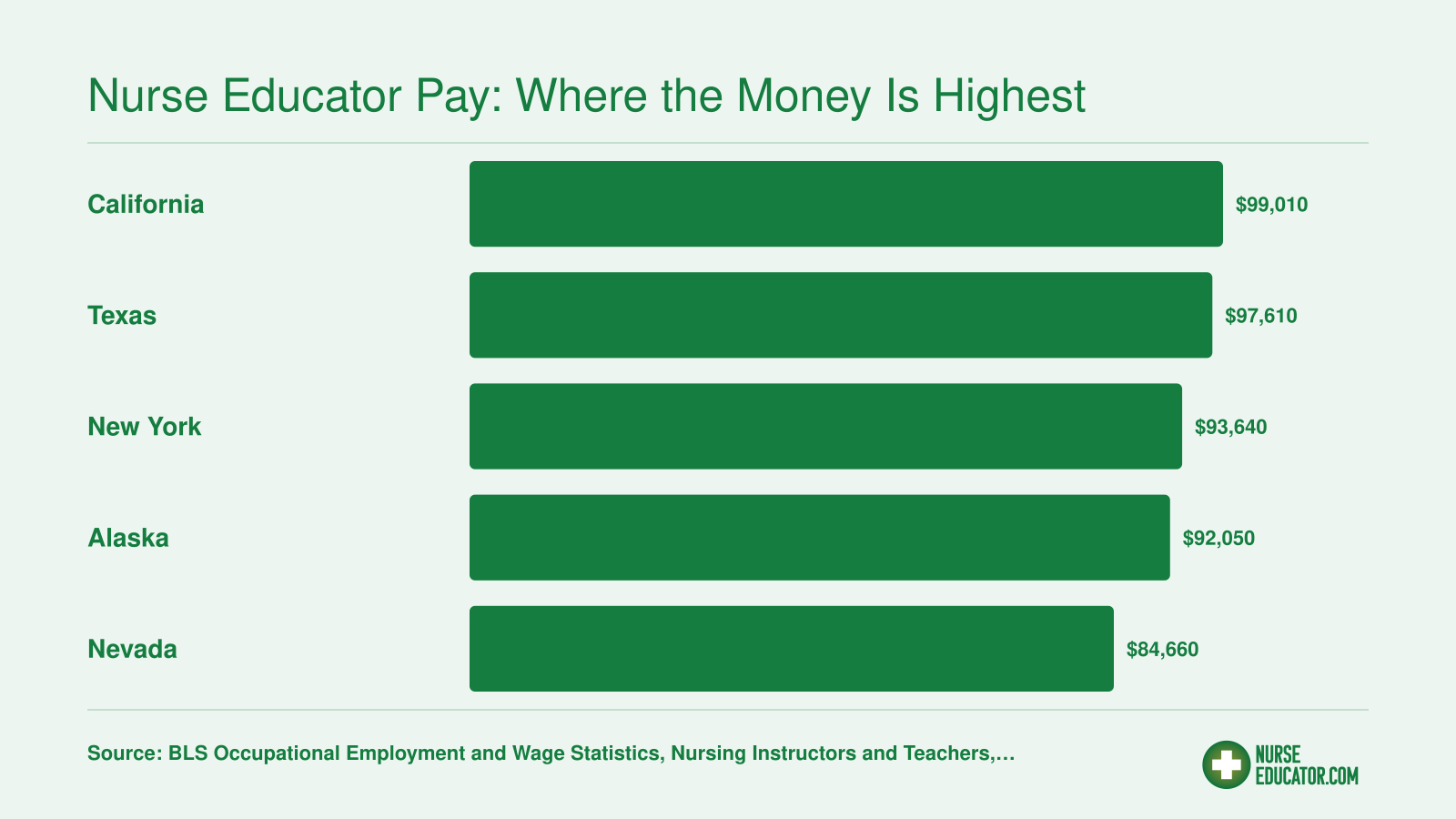
Nurse Educator Pay: Where the Money Is Highest
California and Texas lead the nation in nurse educator compensation, with median salaries well above the national median of roughly $77,000 for nursing instructors and teachers (postsecondary). Here is how the top five highest-paying states compare based on BLS state-level data.
Education and Credential Requirements by Role
How much school do you actually need to become a nurse educator, and how does that compare to becoming an NP, PA, or physician?
The short answer: nurse education has a flexible degree ladder, a voluntary certification layer, and a much shorter runway to practice than medicine, though expectations have risen considerably in the past decade.
The Degree Ladder for Nurse Educators
The master of science in nursing (MSN) with a nursing education focus remains the most common entry point into academic teaching roles. Community colleges and hospital-based staff educator positions will often hire at this level, making it the practical starting line for most career changers. If cost is a concern, you can find affordable online nurse educator MSN programs that keep tuition manageable without sacrificing accreditation.
A doctor of nursing practice (DNP) is increasingly preferred, and sometimes required, at four-year universities and in practice-focused faculty roles. A PhD in nursing positions you for research-intensive appointments at major universities, where generating scholarship is as central as teaching. An Ed.D. (doctor of education) is a less common but recognized path, particularly for nurses drawn to educational leadership, curriculum design, and administration rather than clinical research.
In practical terms: community college adjunct faculty and staff educators at hospitals often hold an MSN, while tenure-track positions at research universities typically expect a PhD or at least a DNP with a clear scholarly agenda.
CNE and CNEcl Certification from the NLN
The National League for Nursing offers two credentials that define the nurse educator specialty. For a detailed breakdown of the differences, see our CNE vs. CNEcl certification comparison.
The certified nurse educator (CNE) is designed for academic faculty teaching in formal nursing programs. Eligibility requires a master's or doctoral degree in nursing, either with an emphasis in nursing education (or nine or more graduate credits in education coursework), or an alternative pathway: a graduate degree in nursing with a different emphasis, combined with at least two years of employment in a nursing program within the past five years.1 Neither pathway requires a minimum number of clinical hours.1 The 2026 exam fee runs $425 for NLN members and $525 for non-members, with renewal every five years at $350 (member) or $450 (non-member).2 The NLN has not published an official pass rate, though informal estimates circulate around 85 percent.3
The certified nurse educator clinical (CNEcl) targets academic vs. clinical nurse educator roles: clinical instructors, adjunct clinical supervisors, and preceptors working within academic nursing programs. Eligibility mirrors the CNE in degree requirements, with pathways accommodating education-focused graduate preparation or clinical teaching experience in an academic setting.4 No minimum clinical hours are required. The renewal cycle is also five years, and as of 2026 the NLN has not published an official pass rate for this credential either.4
Both certifications are voluntary. However, hiring committees at many nursing programs now treat them as a meaningful differentiator, and some institutions list CNE eligibility as a preferred qualification in faculty postings.
How This Compares to NP, PA, and MD Pathways
The contrast with other advanced roles is sharp.
Nurse practitioners must hold board certification to practice legally in every state. The two major certifying bodies are the American Association of Nurse Practitioners (AANP) and the American Nurses Credentialing Center (ANCC), and certification is tied directly to licensure, not professional distinction.
Physician assistants must pass the PANCE (Physician Assistant National Certifying Exam) before they can obtain a license, and recertification is required every ten years. Physician licensure adds a residency requirement of three to seven years after medical school, representing a post-graduate commitment that dwarfs anything on the nurse educator track.
The key distinction: for NPs, PAs, and physicians, the credential is the legal ticket to practice. For nurse educators, the CNE or CNEcl signals expertise and professional seriousness, but you can teach without it. That gap is narrowing as programs raise their hiring standards, but it remains a meaningful difference in how each credential functions within its field.
Path From Bedside RN to Certified Nurse Educator
Transitioning from clinical nursing to a certified educator role follows a clear sequence. Here is a realistic timeline so you can plan each milestone with confidence.

Day-To-Day Responsibilities: Teaching Vs. Clinical Practice
Shaping future nurses in a classroom versus managing a panel of patients in a clinic: these are two fundamentally different rhythms of work, and the daily calendar of each role reflects that split clearly.
A Typical Day for a Nurse Educator
A full-time academic nurse educator usually structures the week around teaching blocks, prep time, and student support. For a deeper look, see our guide on what a typical work day looks like for a nurse educator. On a given day you might:
- Design and update curriculum: Revise course objectives, build rubrics, align content with NCLEX blueprints, and map assignments to accreditation standards.
- Deliver instruction: Lecture in classrooms, lead seminars, or facilitate small-group case discussions, often for two to four hours of contact time.
- Run simulation labs: Set up high-fidelity manikins, brief students, run the scenario, and debrief, which is where much of the critical-thinking work happens.
- Supervise clinical rotations: Travel to partner hospitals to mentor students at the bedside, evaluate skills checklists, and confer with unit preceptors.
- Engage in scholarly work: Grade, write recommendations, sit on committees, conduct research, or prepare conference presentations.
Office hours, advising, and committee service round out the schedule. Tenure-track faculty also carry publication expectations.
How NP Days Differ
Nurse practitioners spend the bulk of their hours in direct patient care. A primary-care NP might see 18 to 25 patients per day: taking histories, performing physical exams, ordering and interpreting labs, diagnosing acute and chronic conditions, prescribing medications, and coordinating referrals. The work is autonomous in most states, decisions are made in real time, and documentation happens between visits. There is no curriculum to write at 9 p.m., but there is a full inbox of patient messages.
Where the CNS Sits in Between
Clinical nurse specialists occupy a hybrid space. Their day often blends bedside consultation on complex cases, leading evidence-based practice projects, training staff nurses on new protocols, and driving systems-level quality improvement. A CNS may teach, but the audience is working nurses rather than students, and the goal is unit performance rather than degree completion. If you are curious about how nurses teach other nurses in these settings, the dynamics differ significantly from academic instruction.
Clinical Currency for Educators
Nurse educators rarely carry direct patient assignments, but most maintain clinical competency through per-diem or adjunct practice, summer hospital work, or by precepting alongside students. Many programs and certification bodies expect this ongoing practice so faculty stay credible at the bedside they are preparing students to enter. If you are weighing whether you still want nurse educator patient care responsibilities, know that most educators do find ways to stay connected to clinical work.
Questions to Ask Yourself
Academic Vs. Hospital-Based Nurse Educator Roles
Not all nurse educator positions look the same. The two main tracks, university or college faculty and hospital-based clinical educator, differ in daily responsibilities, credential expectations, earning potential, and long-term career trajectory. Understanding where each path leads will help you choose the setting that fits your professional goals.
University and College Faculty
Academic nurse educators teach in pre-licensure or graduate nursing programs. Their work typically includes designing curricula, delivering lectures, supervising clinical rotations, mentoring students through research projects, and publishing scholarly work. Faculty roles usually fall into two categories:
- Tenure-track positions: These require a doctoral degree (PhD or DNP) at most universities and carry expectations for research, publication, and service to the institution.
- Clinical-track positions: Often open to master's-prepared nurses, clinical-track faculty focus primarily on teaching and clinical supervision rather than research output.
According to the American Association of Colleges of Nursing, the national median salary for master's-prepared nursing faculty is approximately $93,958.1 Compensation varies considerably by rank, institution type, and geographic region. The American Association of University Professors reports that full-time faculty across all ranks saw a salary increase of about 2.3% for the 2025-26 academic year, suggesting modest but steady growth.2 For a deeper look at compensation across states, see our breakdown of highest paid nurse educators.
Hospital-Based Clinical Educators
Hospital-based nurse educators work within health systems to handle staff development, new-hire onboarding, competency training, and continuing education. Their scope centers on institutional protocols, evidence-based practice updates, and quality improvement metrics rather than academic publishing.
A master's degree in nursing education or a related field is typically required, but a doctoral degree is often not expected. Certification such as the CNE (Certified Nurse Educator) can strengthen your candidacy, though some hospitals accept equivalent clinical credentials.
Direct salary comparisons between hospital and academic educators are limited in publicly available data. However, hospital-based educator roles in high cost-of-living metro areas frequently advertise salaries that exceed academic faculty pay at comparable experience levels. Health system educators may also receive shift differentials, clinical bonuses, and employer-matched retirement contributions that are less common in academic contracts.
Autonomy and Scope
The two settings offer distinctly different kinds of professional independence:
- Academic educators enjoy broad latitude over course design, teaching methods, and research agendas. They shape the profession's future workforce and contribute to nursing science through scholarship.
- Hospital educators operate within the framework of organizational goals, regulatory requirements, and patient safety standards. Their impact is immediate and measurable, often tied to staff competency rates, reduced errors, or improved patient outcomes.
Neither path is inherently better. If you thrive on curriculum innovation and long-term mentorship, the academic route is worth the doctoral investment. The ongoing nursing faculty shortage also means strong demand for qualified candidates in higher education. If you prefer staying close to clinical practice and seeing direct results from your teaching, a hospital-based role lets you do exactly that, often without the years of additional education a tenure-track appointment demands.
Career Outlook and Job Growth for Nurse Educators
Postsecondary nursing instructors and teachers are projected to see job growth of 7% or higher from 2024 to 2034, a rate the Bureau of Labor Statistics classifies as "much faster than average" compared to the 3.1% growth expected across all occupations.12 That headline number tells only part of the story, though. Understanding how nurse educator demand stacks up against other advanced nursing and clinical roles gives you a clearer picture of where opportunity really lives.
How Nurse Educator Growth Compares to NPs and RNs
Nurse practitioners have consistently been among the fastest-growing occupations in healthcare, with BLS projections for 2024 to 2034 expected to outpace most other roles in the sector.3 Registered nurses, by contrast, tend to track closer to the broader healthcare practitioner category, which is projected at 7.2% growth over the same period.2 In pure percentage terms, NP growth is likely to be steeper than nurse educator growth. But percentages alone can be misleading because the total employment base for each role differs dramatically: there are roughly three million RNs nationally, a much smaller pool of NPs, and a comparatively modest number of postsecondary nursing faculty. Even moderate percentage growth in the educator category translates into meaningful demand when set against a workforce that is already stretched thin.
The Faculty Shortage Factor
The real engine behind nurse educator demand is not just population-level healthcare needs. It is the persistent shortage of qualified nursing faculty. The American Association of Colleges of Nursing (AACN) has reported for years that tens of thousands of qualified applicants are turned away from baccalaureate and graduate nursing programs annually, largely because schools cannot hire enough instructors to expand capacity. Faculty retirements compound the issue: a significant share of current nursing professors are approaching or past traditional retirement age, and the pipeline of doctoral-prepared replacements has not kept pace.
This shortage creates a self-reinforcing cycle. Fewer faculty members mean fewer new nurses graduate, which tightens the clinical workforce, which in turn increases the urgency to train more nurses, which circles back to the need for more educators.
What This Means for Your Career Planning
If you are weighing a move into nursing education, the takeaway is encouraging but nuanced:
- Growth is strong. A "much faster than average" BLS outlook puts nurse educators in favorable territory alongside other high-demand healthcare roles.1
- Demand is retirement-driven. Unlike NP roles, where growth is fueled primarily by expanding scope of practice and patient access needs, educator openings are heavily shaped by retirements and the faculty pipeline gap.
- Absolute numbers are smaller. You will not see the sheer volume of job postings that exist for bedside RNs or NPs. Academic and clinical teaching positions are more targeted, so networking, geographic flexibility, and the right credentials matter more.
- Institutional variety is expanding. Hospitals, simulation centers, and online programs are all hiring nurse educators, not just traditional universities. This broadens the market beyond what BLS postsecondary numbers capture.
The bottom line: nurse educator job growth may not grab headlines the way NP projections do, but the combination of favorable BLS forecasts, an aging faculty workforce, and an unresolved pipeline gap makes this one of the more secure long-term career paths in advanced nursing. If you hold or are pursuing a doctoral degree (consider affordable nurse educator Ph.D. programs) and the Certified Nurse Educator credential, you are positioning yourself for a market that genuinely needs you.
Common Career Transitions Into Nurse Education
The pathway into nurse education is rarely a single leap. Most educators arrive through one of several well-worn tracks that allow them to test the teaching waters before committing full-time. Understanding these common transitions can help you chart a realistic timeline and choose the credentials that match your starting point.
From Bedside RN to MSN-Prepared Educator
The most direct route begins with clinical experience as a staff nurse, typically followed by enrollment in an MSN program with a nursing education or teaching concentration. Most programs require at least one to two years of RN experience before admission, and many nurses continue working part-time while completing the degree. Graduates often start as clinical instructors, supervising students in hospital settings, before moving into full-time faculty positions. This path builds pedagogical skills from the ground up and is the standard entry point for those who know early in their career that they want to teach. If you are weighing the move, our guide on becoming a nurse educator walks through the readiness signals worth considering.
Can a Nurse Practitioner Become a Nurse Educator?
Yes, and NP clinical expertise is highly valued in academic settings, especially in programs that emphasize advanced practice or specialty tracks. Many nurse practitioners transition into teaching by accepting part-time adjunct roles while maintaining a clinical practice, then gradually shift toward full-time faculty positions as they discover a passion for education. Universities often recruit NPs to teach pharmacology, pathophysiology, or clinical assessment courses, leveraging their diagnostic and prescriptive authority to bring current practice into the classroom. Some schools offer post-master's certificates in nursing education specifically for NPs or clinical nurse specialists who already hold an MSN but not in an education-focused track, allowing them to add teaching credentials without repeating foundational graduate coursework.
CNS to Staff Educator to Academic Faculty
Clinical nurse specialists frequently move into nurse education through hospital-based staff development roles, where they design orientation programs, lead continuing education, and mentor new hires. This experience translates well to academic teaching, and many CNSs eventually apply for faculty positions at community colleges or universities. The transition is often gradual: teaching one course per semester as an adjunct, then increasing the load over time. This incremental approach lets you build a teaching portfolio and determine whether academic life suits you before leaving clinical employment entirely.
Adjunct and Clinical Instructor Roles as Testing Grounds
Many nurse educators start part-time, balancing clinical shifts with a single course or clinical supervision assignment. Adjunct teaching offers a low-risk way to explore whether you enjoy curriculum planning, grading, and classroom management. If the fit is good, you can pursue additional credentials or apply for tenure-track positions. If not, you retain your clinical role and income. Curious about why nurses become nurse educators? The motivations range from burnout recovery to a genuine calling to shape the next generation. Either way, this flexibility makes the transition gradual rather than all-or-nothing, reducing financial and professional risk.
Is Being a Nurse Educator Worth It?
Nurse education offers a genuinely rewarding career path, but it comes with trade-offs that deserve honest examination before you make the leap from clinical practice.
What Makes It Worth It
The most consistent finding in nursing faculty research is that educators draw deep satisfaction from their work.1 Autonomy ranks high: you design curricula, mentor students over time, and watch your influence ripple outward through every nurse you prepare. That sense of legacy is difficult to replicate at the bedside. Intellectual stimulation is another real advantage. Unlike many clinical shifts, which can settle into familiar routines, teaching demands continuous learning as evidence, technology, and standards evolve.
For nurses leaving high-acuity environments, the shift away from rotating weekends, mandatory overtime, and physical demands is also significant. Academic schedules rarely mirror the relentlessness of a 36-hour-per-week bedside rotation.
The Burnout Picture Is More Complicated
Nurse educators are not immune to exhaustion. Research using the Maslach Burnout Inventory found that midcareer academic nurse educators scored a mean emotional exhaustion score of approximately 23.55, meaningfully higher than postsecondary teachers overall (a statistically significant difference at p=0.0086).1 Workload pressure, especially around research expectations, accreditation demands, and understaffed nursing faculties, drives much of that strain.
For context, bedside nursing fares worse on most burnout measures: national surveys consistently find that 60 to 70 percent of acute-care RNs endorse high burnout or emotional exhaustion.2 Compressed schedules (three 12-hour shifts) do offer extended recovery time, which some nurses prize.3 Nurse practitioners face their own version of burnout, shaped by productivity targets, documentation burden, and role ambiguity rather than direct patient-care intensity.1
Putting It All Together
No role is burnout-proof. The question is which sources of stress you find more manageable and which rewards matter most to you. If shaping the next generation of nurses, maintaining schedule control, and engaging intellectually outweigh a potential salary gap compared to NP or specialist roles, nurse education is very likely worth it. You can explore careers in nurse education to see the full range of paths available. If compensation growth and direct patient interaction are your primary motivators, a clinical trajectory will serve you better. The decision is personal, but the data gives you solid ground to stand on.
Frequently Asked Questions About Nurse Educator Careers
These are some of the most common questions nurses ask when weighing a move into education. Each answer draws on the salary data, credential requirements, and role comparisons covered earlier in this article.
What Is the Difference Between a Nurse Educator and a Nurse Practitioner?
This is one of the most common questions nurses ask when weighing an advanced degree. Both roles require graduate education and build on your RN foundation, but they diverge sharply in daily focus, earning potential, and career trajectory. The quick answers below break down each difference so you can decide which path fits your goals.