What you’ll learn in this article…
- Covista and Advocate launched a formal nursing pipeline partnership in June 2026.
- Per-student pipeline costs range from roughly $200 to over $10,000 annually.
- Structured pipelines measurably improve diversity, retention, and time to licensure.
Reactive recruitment, posting clinical openings after attrition has already thinned your cohort, versus proactive pipeline building, cultivating future nurses years before they ever apply. The difference increasingly determines which nursing programs fill their seats and which operate below capacity. The U.S. is projected to need more than 200,000 new registered nurses each year through 2030, and schools turned away over 90,000 qualified applicants in 2023 alone, largely due to faculty and clinical site constraints.
Nurse educators sit at the exact intersection where the solution takes shape. Building nursing student pipelines is a long-term, structural strategy that spans high school outreach, community college articulation, apprenticeship models, employer partnerships in nursing education, and wraparound student support. Recent moves, such as the Covista and Advocate partnership announced in June 2026, confirm that health systems are actively seeking academic collaborators who can co-design these pathways.1 Programs that wait for applicants to find them are already behind.
What Are Nursing Student Pipeline Programs and Why Do They Matter?
A nursing student pipeline program is a coordinated, multi-year continuum that guides prospective nurses from early exposure in middle or high school, through academic preparation and clinical training, and ultimately to licensure and employment in a healthcare setting. Unlike a single recruitment event or open house, a pipeline sustains engagement across years, building relationships with students long before they submit a college application.
The Urgency Behind Pipeline Development
Passive recruitment strategies are no longer enough to meet healthcare demands. The Bureau of Labor Statistics projects the U.S. will need more than 200,000 new registered nurses each year through 2031 to fill vacancies and replace retirees. Meanwhile, the National Council of State Boards of Nursing reports that nearly one in five RNs intend to leave the profession within the next five years, with retirement rates accelerating among nurses over age 55. These overlapping pressures create a gap that traditional admissions cycles cannot close on their own.
Waiting for students to discover nursing on their own, apply, and hope they persist through graduation leaves too much to chance. Healthcare systems and nursing programs that invest in structured pipelines report stronger enrollment yields, higher retention rates, and shorter time-to-hire for graduates.
How Pipelines Differ From Traditional Recruitment
A traditional admissions funnel begins when a prospective student raises their hand, submits an inquiry, or attends an information session. The institution responds, and if all goes well, the student enrolls. The relationship starts at the student's initiative.
Pipeline programs flip this model. They reach into middle schools, high schools, and community organizations to introduce nursing as a viable career before students have formed fixed ideas about their futures. They offer summer camps, job shadows, mentorship pairings, and dual-enrollment courses that keep students connected over time. By the point of application, participants already have institutional relationships, academic preparation, and sometimes even clinical exposure.
The Nurse Educator's Role in Pipeline Design
Nurse educators occupy a unique position in pipeline work. On one side, you serve as an academic gatekeeper, shaping curriculum standards, admissions criteria, and progression policies. On the other, you function as a community liaison, representing your institution at career fairs, advising high school counselors, and mentoring prospective students who may be years away from enrollment.
This dual role makes educators essential to pipeline success. You can identify the academic competencies students need before they arrive, design bridge programs that address gaps, and advocate for institutional resources that sustain long-term partnerships with schools and healthcare employers. Building effective clinical partnerships in nursing education is one concrete way educators translate that advocacy into durable infrastructure. Without educator involvement, pipelines risk becoming disconnected marketing campaigns rather than integrated pathways to the profession.
Types of Nursing Pipeline Programs: From High School Clubs to Apprenticeships
Nursing pipeline programs have never been more varied, and that variety is exactly the point. No single model fits every community, institution, or student population, so understanding the full landscape helps you choose the right entry points for your program.
High School Exposure and Pre-Nursing Clubs
These programs introduce students to nursing before they ever set foot in a college classroom. Typically organized around CTE health science tracks or summer intensives, they target high school students from disadvantaged communities and aim to spark early interest rather than deliver clinical training.1 Educator involvement tends to be light on formal instruction but high on mentorship and campus visits. Costs vary widely depending on whether the program is grant-funded or institutionally supported, but many operate on modest budgets because they rely on volunteer faculty time and donated simulation hours.
- Target audience: High school students, especially those in CTE health science pathways
- Duration: A single semester or a summer program, sometimes recurring annually
- Best fit: Urban programs with proximity to high schools; also effective in rural districts through regional partnerships
Community College Bridge and Stackable Pathways
Bridge programs let students move from a CNA or LPN credential into an RN program without starting over. Initiatives like California's Strengthening the Nursing Pipeline effort have shown that stackable pathways are especially effective for students in urban, rural, and underserved communities who need flexible, affordable entry points.2 Educator involvement is significant here because curriculum alignment between institutions requires ongoing faculty coordination.
- Target audience: Working adults, community college enrollees, and students from underserved populations
- Duration: One to two years depending on the entry credential
- Best fit: Community colleges and regional consortia, both rural and urban
Accelerated BSN Tracks
Designed for career changers who already hold a bachelor's degree, second-degree BSN programs compress traditional four-year curricula into 12 to 18 months of intensive coursework.3 Faculty workload is high, and clinical placement coordination demands close relationships with hospital partners. These programs tend to carry higher tuition than traditional tracks, which can limit access for some students without scholarship support.
- Target audience: Career changers with a prior bachelor's degree
- Duration: Typically 12 to 18 months
- Best fit: Larger nursing programs in metro areas with robust clinical site networks
Apprenticeship Models
Registered nursing apprenticeships, recognized under the U.S. Department of Labor framework, are the fastest-growing pipeline category right now. Policy is evolving quickly at both the federal and state levels, and health systems are increasingly willing to fund earn-while-you-learn models that keep apprentices employed during training. Educator involvement shifts toward competency-based assessment and workplace mentorship rather than traditional classroom delivery. Costs per apprentice are often offset by employer contributions, making this model financially attractive for institutions willing to build the infrastructure.
- Target audience: Entry-level healthcare workers seeking a pathway to RN licensure
- Duration: Two to three years, depending on state standards
- Best fit: Health-system-aligned programs; increasingly viable in rural settings where employers need local workforce solutions
Academic-Clinical and Regional Partnerships
Programs like READI 2 Work and Area Health Education Center (AHEC) networks sit at the intersection of education and practice. They connect nursing schools with healthcare employers to create shared pipelines, co-funded clinical training, and coordinated recruitment. Academic-practice partnerships in nursing distribute the cost and administrative burden across multiple stakeholders, which makes them scalable for both small programs that lack resources and large systems managing high student volume.
- Target audience: Broad, often spanning high school through graduate entry
- Duration: Ongoing, relationship-based rather than time-limited
- Best fit: Programs in regions with active AHEC networks or employer coalitions willing to co-invest
Taken together, these six models give nurse educators a genuine toolkit. The right combination depends on your institution's size, geographic setting, existing employer relationships, and the student populations you are trying to reach.
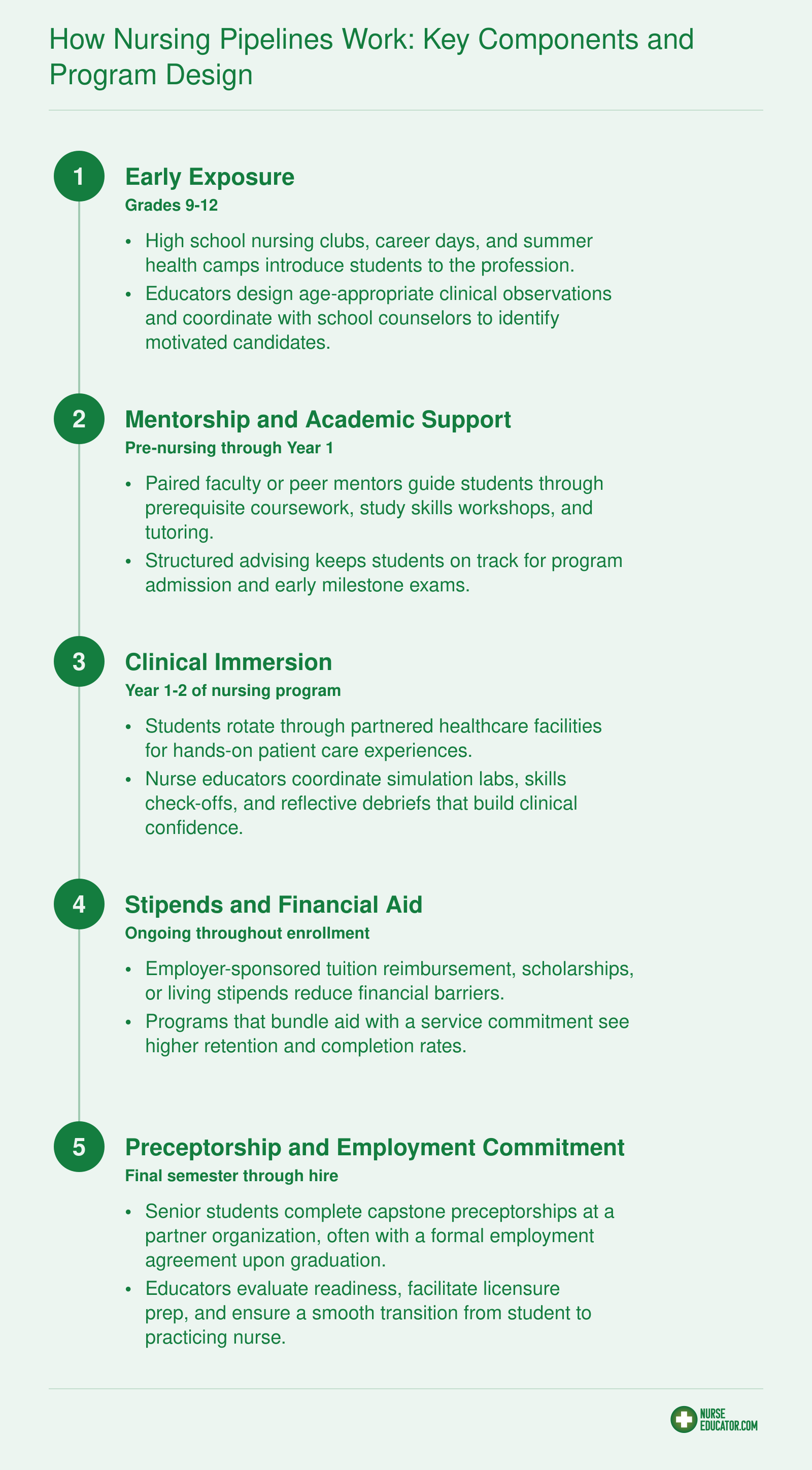
How Nursing Pipelines Work: Key Components and Program Design
The strongest nursing student pipeline programs connect at least four or five of these stages into a single, coordinated pathway. Each stage carries specific educator responsibilities and clear student milestones, so gaps are caught early and momentum stays high.
Questions to Ask Yourself
Building a Pipeline Step by Step: A Framework for Nurse Educators
Twelve to eighteen months is the typical timeline from initial concept to first cohort enrollment for most nursing pipeline programs, according to implementation patterns observed across academic health partnerships. That window may feel long, but rushing the process often leads to underenrolled cohorts, misaligned curricula, or partnerships that dissolve after one cycle. A structured framework helps nurse educators build pipelines that actually function and persist.
Step 1: Conduct a Community Needs Assessment
Before approaching partners or drafting curricula, analyze your local landscape. Gather demographic data on high school graduation rates, community college enrollment trends, and the age distribution of working nurses in nearby health systems. Identify which feeder schools already send students into healthcare tracks and which neighborhoods remain underrepresented in your applicant pool. Talk to local employers about their hiring projections and vacancy rates. This step prevents a common failure mode: building a pipeline that nobody uses because it targets the wrong population or geographic area.
Step 2: Identify and Formalize Partnerships
Pipelines require partners. Reach out to K-12 districts, community colleges, and health systems with a clear value proposition. For school districts, emphasize career exposure and college readiness. For community colleges, highlight articulation agreements and transfer pathways. For health systems, stress workforce development and potential recruitment advantages. Put agreements in writing. Memoranda of understanding should specify each party's responsibilities, data-sharing protocols, and timelines for review.
Step 3: Align Curriculum With Program Prerequisites and Accreditation
Pipeline coursework must feed directly into your nursing program's admission requirements. Map prerequisite courses, clinical observation hours, and any certification components (such as CNA training) against your institution's standards and state board requirements. Accreditation bodies expect transparency in how pre-nursing experiences connect to degree outcomes. Document these alignments early to avoid compliance headaches later. Understanding the nursing education curriculum your program expects students to enter with is essential to building that map correctly.
Step 4: Secure Staffing and Protect Faculty Time
Pipeline coordination demands dedicated attention. Estimate five to ten hours per month for tasks such as partner communication, student tracking, event planning, and data collection. Decide whether an existing faculty member will absorb this role, whether you will hire a part-time coordinator, or whether an administrative staff member can manage logistics. Faculty workload is already stretched in most nursing programs, so building in protected time or compensation prevents burnout and turnover in the coordinator role.
Step 5: Pilot With a Single Cohort and Defined Timeline
Resist the urge to launch multiple tracks at once. Start with one cohort at one partner site. Define a clear timeline: application period, orientation, intervention activities, and transition points into your nursing program. A smaller pilot allows you to troubleshoot logistics, identify curriculum gaps, and gather meaningful data without overextending resources.
Step 6: Iterate Based on First-Year Data
After your pilot cohort completes its cycle, review outcomes systematically. Track how many students applied, enrolled, completed prerequisites, and ultimately entered your nursing program. Survey participants about their experience. Meet with partner organizations to discuss what worked and what needs adjustment. Use this data to refine recruitment messaging, adjust curriculum sequencing, or reallocate staffing before scaling to additional cohorts or partner sites. Paying attention to early warning signs of struggle is equally important; nursing student retention strategies can inform how you structure support checkpoints throughout the pipeline.
Following this six-step framework gives nurse educators a replicable structure. The temptation to skip the needs assessment or rush into multiple partnerships often leads to fragmented efforts. A methodical approach, even when it takes over a year, produces pipelines that deliver students who are ready to succeed.
Funding Models and Cost per Student: What the Numbers Look Like
Pipeline programs are affordable to start and expensive to scale, and the per-student cost varies more with program depth than with geography. A high school exposure club running after school is a fundamentally different budget line than a paid apprenticeship that carries a student through licensure, and educators who conflate the two will underprice the wrong end of the pipeline every time.
Per-Student Cost Ranges by Program Type
Use these as planning brackets, not fixed prices. Actual costs shift with faculty salaries, clinical site fees, and whether stipends are involved.
- High school exposure and clubs: Typically the cheapest tier. Costs concentrate in curriculum materials, guest speaker honoraria, and coordinator time. Many programs run on a few hundred dollars per student per year when hosted inside an existing CTE structure.
- Community college partnerships and dual enrollment: Mid-range. The California Community Colleges Chancellor's Office reports a BSN pathway tuition and fee load around $10,560,1 which is a useful anchor for what a student pays, though the institutional cost to deliver is higher once faculty and clinical placements are counted.
- Accelerated BSN tracks: One private accelerated BSN program shared by a nurse educator community carries a total program cost near $53,000 per student.2 Public and hospital-subsidized versions can land lower, but this is the ballpark to plan against.
- Apprenticeships: The most expensive per-seat, because they combine wages, preceptor time, tuition support, and coordination overhead across two organizations.
Where the Money Comes From
Most sustainable pipelines braid several sources rather than relying on one. The primary categories:
- HRSA Nursing Workforce Development grants (Titles VII and VIII) for faculty support, student stipends, and program infrastructure.
- Title V and Perkins CTE funds for secondary and postsecondary career pathway work.
- State workforce dollars. Texas appropriated $46.8 million to the Professional Nursing Shortage Reduction Program in 2024, an increase of $27.9 million.3 Kansas layered roughly $6.5 million in student aid with $10 million in institutional funding for 2025-2026, and its Medical Loan Program awards $4,000 for LPN and $5,000 for RN scholarships.4
- Hospital system co-investment, increasingly common as systems recognize that labor represents about 56% of hospital expenses nationally.5 nursing faculty shortage solutions compound this pressure: when programs cannot hire educators, they cannot expand cohorts, making hospital dollars even more critical.
- Philanthropic grants from regional foundations and health conversion foundations.
A Practical Budget Framework
Split your budget cleanly. Direct costs include student stipends, uniforms and supplies, clinical site fees, licensure exam prep, and background checks. Indirect costs include faculty release time, program coordinator salary, evaluation and data infrastructure, and marketing.
Start with grant funding for the pilot phase. Grants tolerate the ambiguity of a new model. Once you have two or three cohorts of nursing student retention and NCLEX data, use those outcomes to negotiate an institutional budget line or a formal hospital co-investment agreement. That transition, from soft money to hard money, is where most pipelines either mature or quietly fold.
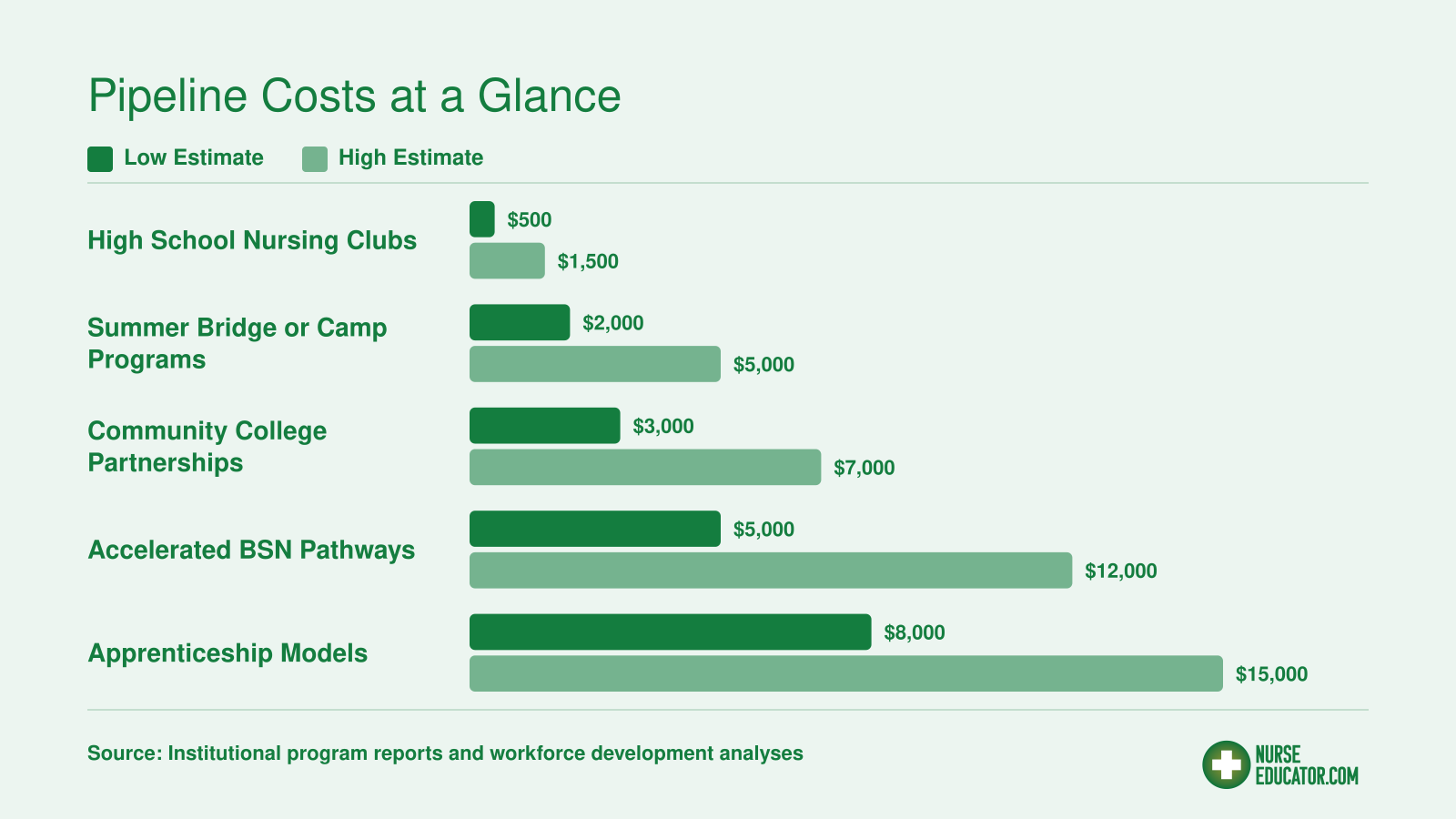
Pipeline Costs at a Glance
Pipeline program costs vary widely depending on the model, intensity of student support, and length of engagement. The ranges below reflect published estimates and institutional reports across common pipeline types. Keep in mind that grants and employer partnerships typically cover 40% to 60% of total program costs, significantly reducing the out-of-pocket burden on academic institutions.
Advancing Diversity: Pipeline Strategies for Underrepresented Students
How can nursing programs move beyond diversity statements and actually increase representation in the workforce?
The numbers tell a clear story: nationally, about 76.6% of registered nurses are white, while Black nurses represent just 8.6%, Hispanic nurses 7.2%, and Asian nurses 7.9%.1 Pipeline programs designed with structural supports, not just good intentions, offer the most promising path toward meaningful change.
Evidence From High School CTE Immersion Models
High school Career and Technical Education nursing immersion pipelines have demonstrated strong outcomes in communities with high concentrations of underrepresented students. One documented program serving schools where 65% to 79% of students were Hispanic and 70% to 93% were economically disadvantaged achieved a 90% completion rate among a 31-student cohort.2 These results suggest that early exposure combined with clear pathways can overcome barriers that typically filter out first-generation and minority students before they ever reach a nursing program application.
California community college nursing pipelines reported that 62% of their students in the 2024-25 academic year came from economically disadvantaged backgrounds, though Black student enrollment in RN programs remained at just 5%.3 The state has expanded capacity by 15% and seen enrollment increases of 12% to 18%, but demographic representation has not shifted proportionally, highlighting the difference between growing a pipeline and diversifying it.
Models Designed for Diversity Outcomes
Programs like Plant the Seed and HBCU-affiliated nursing pipelines intentionally center underrepresented students rather than treating diversity as an afterthought. The federal Nursing Workforce Diversity Program reports that 60% of its participants come from underrepresented minority backgrounds,4 demonstrating what targeted funding and program design can accomplish.
Culturally responsive mentorship has emerged as a critical retention factor. Pairing students with mentors who share their backgrounds and understand their communities creates accountability and belonging that generic advising cannot replicate. Some programs integrate community health workers into their pipeline design, connecting students to health careers through trusted community figures who can navigate cultural and logistical barriers alongside academic ones. Nurse educators interested in the broader equity dimensions of this work will find it connects directly to how nurse educators can promote health equity in their communities.
Structural Supports That Actually Work
Avoiding performative diversity language means investing in what actually helps students persist. Pipeline programs with strong diversity outcomes typically include:
- Stipends: Paid time for clinical hours or coursework reduces the impossible choice between earning and learning.
- Childcare assistance: Students with caregiving responsibilities often drop out when childcare falls through, not when coursework becomes too hard.
- Transportation aid: Bus passes, gas cards, or centralized clinical placements remove a barrier that disproportionately affects low-income students.
- Flexible scheduling: Evening and weekend course options accommodate students who cannot leave daytime jobs.
Without these supports, diversity recruitment becomes a revolving door. Programs attract underrepresented students with marketing materials and lose them to life circumstances that could have been addressed with modest structural investments. Supporting nursing students at risk of dropping out is an equally important counterpart to recruitment, and nurse educators designing pipelines should audit their program's actual support infrastructure against these categories before launching campaigns.
The strongest pipelines are built through active co-design with clinical partners from the outset, not after your curriculum is finalized. When hospitals, health systems, and community partners shape program structure, clinical placements, and student supports together with educators, the result is a seamless pathway that addresses real workforce needs and sustains student momentum from enrollment through employment.
Industry Spotlight: Covista–advocate Partnership Signals New Pipeline Trends
When a health system and an academic institution formally agree to build a nursing student pipeline together, they are creating a structured pathway that recruits, educates, and employs future nurses in a coordinated sequence. This is not simply about clinical placements; it is a deliberate, long-term investment in workforce supply. On June 29, 2026, Crain's Chicago Business reported that Covista and Advocate Health Care launched exactly this kind of partnership, explicitly to address a worsening nursing shortage.1 For nurse educators, this deal is not just a local headline. It signals that major health systems are actively seeking academic partners, and it previews the kind of arrangements that will shape nursing education in the years ahead.
A New Model Emerges
The Covista, Advocate collaboration stands out because it goes beyond traditional clinical contracts. While details are still unfolding, the core premise is a jointly designed pipeline that likely includes commitments around student enrollment targets, mentoring, and employment upon graduation. Such models often include shared resources for faculty, dedicated clinical slots, and early exposure to the employer's culture. For nursing programs, this translates into more predictable student demand and deeper integration with practice settings.
What This Means for Nursing Programs
Too often, nursing schools wait for health systems to approach them with affiliation agreements. The Covista, Advocate announcement flips that script: it shows that employers are moving first to lock in talent pipelines. For nurse educators, the message is clear. Waiting to be recruited is a missed opportunity. Instead, department chairs and deans should proactively identify regional health systems with urgent staffing needs and propose key elements of successful clinical partnerships built around shared goals.
Positioning Your Program as a Partner
To be an attractive partner, nursing programs need to bring concrete data to the conversation. Employers want to see graduation rates, NCLEX pass rates, and employment outcomes for different student populations. They also want flexibility: accelerated tracks, evening and weekend schedules, and pipelines that draw from underrepresented groups. Programs that can demonstrate year-over-year improvement in these areas will have a competitive advantage when negotiating pipeline terms. The Covista, Advocate deal is a reminder that pipeline building is no longer a fringe activity; it is becoming a central function of nursing faculty leadership.
Measuring Success: Outcome Metrics and Program Evaluation
Some programs launch with vivid mission statements but measure outcomes through isolated anecdotes. Others embed systematic evaluation from the first student contact and let real-time data drive every tweak to the model.
A Metrics Dashboard That Works
A well-constructed pipeline dashboard captures the full student journey, from initial outreach through long-term employment. Without a dashboard, programs default to gut feelings about what is working. The following eight metrics, tracked consistently, create a clear picture of pipeline health and surface problems early.
Key Metrics to Monitor
- Pipeline enrollment yield: What portion of students exposed to the pipeline actually enroll in a nursing program? Measure by comparing participants who submit applications or matriculate against total pipeline participants. Data source: program enrollment records. Frequency: each application cycle. Benchmark: Many successful pipelines see yields above 75%, though targets depend on program selectivity.
- Cohort completion rate: Among those who enroll, how many complete the program? Source: institutional student records. Frequency: annually, by cohort. Benchmark: One California community college pipeline reported a 90% completion rate (2023, 2025).1 Aim to track and disaggregate by student subgroups.
- NCLEX pass rate: First-time pass rate for pipeline graduates, compared to the program average. Source: nursing board licensing data. Frequency: quarterly or after each exam window. Benchmark: The same California system saw a 91% average pass rate, with 18 colleges achieving 100% in a recent period.1 Pipeline pass rates should at least match or exceed program averages.
- Post-licensure employment rate: What percentage of graduates secure nursing jobs within 6, 12 months of licensure? Source: graduate surveys, employer verification, or state workforce databases. Frequency: annually. Benchmark: Many programs target 90%+ employment within one year, though market conditions influence this.
- One-year retention rate: Among employed graduates, what share remain in nursing roles after one year? Source: employer follow-up surveys, alumni tracking. Frequency: annually. Benchmark: The same California pipeline reported 93% one-year retention, a strong indicator of preparation and support.1
- Diversity composition vs. community demographics: Does the pipeline's student body reflect the racial, ethnic, and socioeconomic makeup of the communities it serves? Source: enrollment data compared to U.S. Census data for the service area. Frequency: annually. Benchmark: Target proportional representation, or set incremental improvement goals.
- Cost per completer: Total program investment divided by number of students who successfully complete the program. Source: budget and completion records. Frequency: annually. Benchmark: Varies widely; calculate a baseline in year one and work to reduce while maintaining quality.
- Partner satisfaction: Healthcare partners' ratings of graduates' readiness and collaboration effectiveness. Source: structured surveys of clinical partners and employers. Frequency: biannual or annual. Benchmark: Target average scores above 4 on a 5-point scale, with qualitative feedback guiding curriculum adjustments.
Why Day-One Tracking Matters
The most common pipeline evaluation mistake is waiting until year two or three to design the measurement system. By then, data collection processes are fragmented, and critical early baselines are lost. Start capturing enrollment yield and demographic data the moment outreach begins. Build the dashboard as a living tool, not a retrospective report. This discipline enables mid-course corrections, justifies funding, and demonstrates impact to stakeholders who may need convincing.
Turning Data into Action
Numbers alone do not improve outcomes. Schedule quarterly data reviews with the pipeline team to identify trends. For example, if first-year retention dips for a particular cohort, investigate nursing student retention strategies and tutoring resources. If partner satisfaction slips, revisit clinical placement evaluation for nursing students and logistics. The dashboard becomes the engine for continuous improvement, not a static archive.
Common Questions About Nursing Pipeline Programs
Whether you are launching your first pipeline initiative or refining an existing one, these frequently asked questions cover the essentials. Each answer offers a concrete takeaway you can act on right away.
Related Articles
Three actions separate a pipeline idea from a pipeline that enrolls students: run a needs assessment this month to identify your community's workforce gaps and student demographics, reach out to one clinical partner for an exploratory conversation about co-designing a pathway, and draft a one-page pipeline proposal you can bring to your dean or advisory board. These steps mirror the framework outlined earlier in this guide, and they cost nothing but focused time.
For funding, start with HRSA's Nurse Education, Practice, Quality and Retention grant cycles and your state workforce development board, both of which prioritize pipeline-style initiatives. If financial barriers are part of what keeps prospective students from committing, nursing student financial stress is worth addressing in your program design from the start. Every semester without a structured pipeline is another cohort of potential nurses lost to careers that found them first. The nursing shortage is not waiting, and neither should you.