What you’ll learn in this article…
- The U.S. needs over 3.3 million RNs by 2028 but can train roughly 3 million.
- Whitworth's BSN invested $3 million and 10 faculty lines as launch benchmarks.
- State board approval must precede enrollment; national accreditation follows separately.
The United States will need more than 3.3 million registered nurses by 2028, but current education capacity is projected to produce only about 3 million, leaving a shortage of roughly 300,000 nurses. This gap is not an abstraction: it represents unfilled hospital beds, delayed surgeries, and communities without adequate primary care. For nurse educators and administrators, the most sustainable solution is to build new programs that expand enrollment capacity where demand is highest.
Developing a new nursing program requires navigating six interdependent stages: conducting a community needs assessment, securing state board approval, designing a curriculum framework, recruiting faculty and clinical partners, pursuing national accreditation, and launching with evaluation protocols in place. Each stage carries regulatory requirements, resource benchmarks, and decision points that determine whether your program will earn approval and produce graduates who pass the NCLEX-RN on the first attempt.
Whitworth University's new BSN program, launching in fall 2027 with 40 students and a $3 million simulation facility, illustrates how institutions can move from concept to first cohort while meeting state and accreditor expectations.1 The program's timeline, faculty hiring plan, and clinical-hour allocation offer concrete benchmarks that other institutions can adapt to their own regional shortages and institutional missions. Building nursing student pipelines that feed into programs like this one is equally important for sustaining long-term workforce growth.
Why New Nursing Programs Are Urgently Needed
The nursing shortage is not a distant concern or policy abstraction: it is a measurable gap between the number of registered nurses the healthcare system needs and the number available to fill those roles. Understanding the scale of this shortfall helps explain why launching new nursing programs is one of the most direct actions nurse educators can take to address the crisis.
National Workforce Projections Paint a Clear Picture
According to the Bureau of Labor Statistics Occupational Outlook Handbook, registered nursing is projected to grow at 5 percent between 2024 and 2034, with roughly 189,100 openings anticipated each year during that period.1 These openings arise from a combination of retirements, nurses leaving the profession, and new positions created by population growth and aging demographics. Earlier projections suggested the U.S. would need more than 3.3 million registered nurses by 2028 but would only have capacity for approximately 3 million, leaving a substantial gap. While updated federal data refines these estimates over time, the fundamental imbalance persists: demand consistently outpaces the pipeline of new graduates.
Healthcare occupations overall are expected to generate approximately 1.9 million annual openings through 2034, reflecting the sector's outsized role in employment growth.2 Nursing sits at the center of this demand, and the profession's median annual wage of $93,600 as of May 2024 underscores its critical value in the labor market.1
Regional Shortages Vary, and Local Training Matters
National averages mask significant regional variation. Washington state, for example, is projected to face the fifth largest RN shortage in the country through 2038. This is not simply a numbers problem: nurses tend to practice where they train. Data from Spokane-area programs illustrate this retention pattern. WSU Spokane reports that 74 percent of its nursing graduates remain in the region, while Gonzaga University retains 78 percent within Washington state. Eastern Washington University keeps 75 percent of graduates local, and Spokane Community College sees 99 percent of its graduates stay in the Spokane area.3
These retention rates make a compelling case for building nursing education capacity in underserved regions. When you train nurses locally, you grow the local workforce.
New Programs Are a Supply-Side Lever Educators Can Pull
Policy discussions often focus on incentives, loan forgiveness, and workplace improvements to retain existing nurses. These matter, but they do not address the fundamental supply bottleneck: not enough students are entering and completing nursing programs. New program launches, like nurse educator demand driving Whitworth University's BSN program opening in fall 2027, represent a tangible mechanism to increase the pipeline.
Whitworth's plan to enroll up to 40 students per year initially, with potential growth to 80 after 2031, demonstrates how a single institution can meaningfully expand regional capacity. Multiply this across dozens of institutions nationwide, and the cumulative effect begins to address the shortage in real terms.
Faculty Shortages Compound the Challenge
One complicating factor deserves early mention: qualified nursing faculty are themselves in short supply. Programs cannot simply open seats without instructors to fill them. Whitworth's plan to hire 10 full-time faculty members, plus adjuncts, reflects the staffing investment required to launch and sustain a program. The nursing faculty shortage will be explored in greater depth later in this guide, but it is worth noting here that new program development must account for both student capacity and instructor availability from the outset.
The urgency is clear. The pathway forward requires nurse educators willing to build new programs, and the following sections outline how to do exactly that.
From Concept to First Cohort: A Nursing Program Development Timeline
Launching a new nursing program is a multi-year undertaking that demands careful sequencing. The timeline below maps the major milestones most institutions navigate, from the earliest feasibility research through the day your first students arrive on campus. Whitworth University's BSN program offers a useful benchmark: announced in mid-2025, with facility renovations beginning September 2026 and a first cohort enrolling fall 2027.
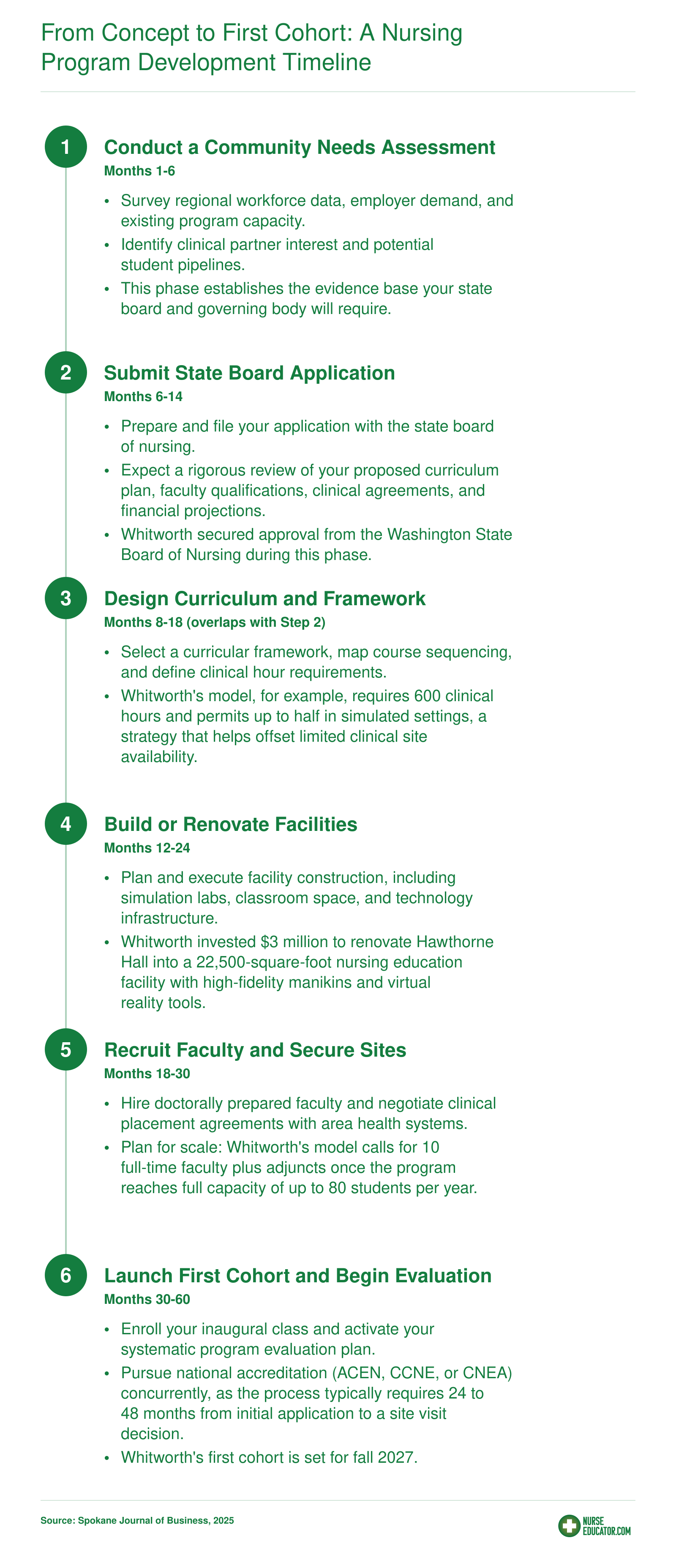
Step 1: Conduct a Community Needs Assessment
A formal needs assessment is the single most consequential document you will produce during program development, because every regulatory body and accreditor will ask for it before anything else moves forward. State boards of nursing require evidence that a new program addresses a genuine workforce gap, and national accrediting organizations expect the same data to appear in your self-study. Treat this document not as a bureaucratic hoop but as the evidentiary foundation for every approval application, budget request, and clinical-site negotiation that follows.
What the Document Must Contain
A complete needs assessment typically covers four domains:
- Regional employer demand: Letters of support from hospital systems, long-term care facilities, and community health agencies, paired with current vacancy rates and projected hiring volumes.
- Existing program capacity: An inventory of every nursing program in your service area, including current enrollment caps, graduation rates, and waitlist sizes. State boards of nursing maintain these inventories and often publish them annually.
- Population health indicators: Community demographics, chronic disease prevalence, aging population trends, and uninsured rates that substantiate the need for more nurses at the bedside.
- Projected workforce gaps: Quantified shortfall estimates over five, ten, and twenty years, drawn from credible forecasting models.
Where to Find the Data
You do not need to commission original research. Most of the evidence you need already exists in public sources:
- Bureau of Labor Statistics (BLS) occupational projections for registered nurses at both the national and state level.
- Your state workforce commission or employment security department, which publishes occupation-specific supply-and-demand reports.
- Hospital system workforce development offices, which can provide internal hiring plans and turnover data.
- Your state board of nursing program inventory, which lists every approved program, its enrollment cap, and its NCLEX pass rate.
Cross-referencing these sources lets you build a layered argument: national projections set the macro context, state data narrows the scope, and local employer testimony makes the case personal and immediate. Programs in regions already grappling with a nursing faculty shortage may find that documenting faculty pipeline constraints alongside student demand strengthens the case further.
Learning from Whitworth's Approach
Whitworth University's new Bachelor of Science in Nursing program, approved for a fall 2027 launch, offers a useful example.1 Their needs assessment anchored on a stark projection: the nation will need over 3.3 million registered nurses by 2028 but will have capacity for roughly 3 million, and Washington state faces the fifth-largest RN shortage through 2038. Whitworth supplemented those macro figures with granular local retention data showing that graduates of Spokane-area nursing programs overwhelmingly stay in the region. Washington State University Spokane retains about 74 percent of its graduates locally, Gonzaga University keeps 78 percent in Washington, and Spokane Community College retains 99 percent in the Spokane area. That combination of statewide shortage projections and documented local retention made a compelling case that adding 40 seats (growing to 80 after 2031) would directly reduce the regional gap rather than simply redistribute graduates from existing programs.
If you are building your own needs assessment, model this layered strategy: lead with national context, anchor in state-level projections, and close with employer-level evidence that ties your proposed program to a specific community need. The stronger this document, the smoother every subsequent step becomes.
Step 2: Navigate State Board Approval and Regulatory Requirements
State Approval vs. National Accreditation: What's the Difference?
A frequent point of confusion is the distinction between state board approval and national accreditation. State board approval is mandatory: without it, your program cannot enroll students, graduates cannot sit for the NCLEX, and the program has no legal standing to operate. National accreditation from bodies like ACEN, CCNE, or CNEA is voluntary (though highly recommended) and typically pursued after or alongside the launch. While both involve rigorous review, state approval is the non-negotiable gatekeeper that grants initial licensure eligibility. strategies to increase NCLEX pass rates depend heavily on clearing this gate first, since board approval governs whether graduates can sit for the exam at all.
The General State Board Approval Process
Though each state has unique requirements, a common pathway emerges across boards of nursing. The process usually begins with a letter of intent or pre-application notice, followed by a formal feasibility study that demonstrates workforce need, institutional capacity, and curricular soundness. Next comes a detailed application package containing curriculum plans, faculty credentials, clinical agreements, and resource inventories. After an initial review, the board conducts an on-site evaluation to verify facilities, simulation labs, and administrative readiness. If successful, the program receives provisional or initial approval, allowing enrollment of the first cohort. Full approval is typically withheld until after the first class graduates and NCLEX pass rates are analyzed. Timelines vary: many states take 12 to 24 months from initial inquiry to provisional approval, though California can stretch to 18 to 36 months. Ongoing monitoring is standard, with board authority to revoke approval if outcomes fall below standards.
State-by-State Variations
Regulatory landscapes differ significantly. Below are examples from four states with large nursing education footprints.
- California (Board of Registered Nursing): Requires a feasibility study, formal application, and an on-site evaluation by the Nursing Education Consultant (NEC).1 Uniquely, the BRN must approve each clinical facility and, for non-accredited programs, individual faculty members.2 The timeline often ranges from 18 to 36 months.1 The board may grant extensions for feasibility studies3 and regularly updates regulations,4 so continuous monitoring of BRN communications is essential.
- Texas (Board of Nursing): Generally requests a letter of intent, a feasibility report, and a new program application detailing curriculum, clinical placements, and faculty qualifications. A site visit is conducted, and the board may require program directors to present. Approval timelines are typically 12 to 18 months if all documentation is in order.
- Florida (Board of Nursing): Requires submission of a new program application along with evidence of compliance with the Florida Administrative Code. Documentation includes curriculum plans, clinical affiliation agreements, and faculty vitae. The board reviews quarterly, and approval can be granted within one year if no deficiencies arise.
- New York (State Education Department): Nursing programs fall under the Office of the Professions. The process demands a comprehensive proposal that includes institutional accreditation, detailed curricula, faculty credentials, and signed clinical agreements. The SED also evaluates library and learning resource adequacy. The timeline can extend beyond two years due to the thorough multi-stage review.
Whitworth's Washington State Approval
A current example underscores the sequential nature of this step. Whitworth University secured approval from the Washington State Board of Nursing before announcing its BSN launch for fall 2027. This approval was a prerequisite for moving forward with facilities renovation, faculty recruitment, and curriculum finalization. For nurse educators developing a program, Whitworth's experience illustrates that state board approval is not a box to check near the end: it is an early, non-negotiable milestone that unlocks enrollment authority.
Questions to Ask Yourself
Step 3: Design Your Curriculum and Choose a Framework
Your curriculum framework is the single most consequential design decision you will make, because it dictates course sequencing, clinical structure, faculty workload, and how you will demonstrate outcomes to accreditors. Choose it before you write a single course syllabus.
Concept-Based vs. Competency-Based Models
Two frameworks dominate contemporary BSN curriculum design, and each fits a different institutional strategy.
- Concept-based curriculum: Organizes learning around big physiological and professional concepts (oxygenation, perfusion, infection, safety, ethics) rather than around medical-surgical, pediatric, and obstetric silos. It works well when you want students to transfer knowledge across populations and settings, and when you have faculty comfortable teaching integratively. It shortens content redundancy but demands strong faculty development.
- Competency-based curriculum: Organizes learning around measurable, observable skills tied to defined performance levels. It fits programs that want tight alignment with the 2021 AACN Essentials, which restructured baccalaureate education around ten domains and sub-competencies. If your institution values clear rubrics, portfolio assessment, and employer-facing outcomes data, competency-based is the natural fit.
Many new programs blend the two: concept-based sequencing with competency-based assessment layered on top.
Aligning with AACN Essentials and Accreditor Expectations
Whichever framework you pick, the 2021 AACN Essentials are effectively non-negotiable for BSN programs pursuing CCNE accreditation, and ACEN standards similarly expect explicit mapping of course objectives to end-of-program outcomes. Build a curriculum map early that traces each Essentials sub-competency to specific courses, active learning strategies in nursing clinical experiences, and learning activities. Accreditors will ask for this document, and reviewers dislike retrofitted maps.
Course sequencing should follow a scaffolded logic: foundational sciences and health assessment, then adult medical-surgical concepts, then specialty populations, then a capstone integration and preceptorship. Clinical experiences must be tied to didactic content in the same term, not deferred.
Clinical Hours and Simulation Strategy
Most BSN programs require between 500 and 750 direct clinical hours. Whitworth's 600-hour target sits in the middle of that range and is a reasonable benchmark. Delaware, by contrast, requires 400 hours for RN programs2 and 200 for LPN programs, while Virginia mandates 500 for RN prelicensure.3
Simulation substitution is where state policy will constrain your design. The NCSBN's landmark 2014 study endorsed up to 50% simulation substitution,4 and states have moved unevenly since:
- 50% cap per course: Arkansas (formalized in 2022 after pandemic-era relaxation), Delaware (2023), Montana, and Virginia allow up to half of a course's clinical hours in simulation, though Virginia caps program-wide substitution at 25%.23
- 25% program-wide cap: Illinois held this line pre-2026, and its new HB1807 (effective 2026) tightens requirements around minimum direct clinical hours and evidence-based simulation practices.5
- No explicit cap: New York provides statutory authorization for simulation without a numeric ceiling (2023).2
- No guidance at all: As of 2024, 19 states still lack explicit simulation policy,6 leaving programs to justify their approach directly to the board.
Nationally, only about 17% of prelicensure programs currently substitute simulation for 26% to 50% of clinical hours,6 so a Whitworth-style 50% strategy is aggressive by current norms. Before you commit facility dollars to high-fidelity labs, confirm exactly what your state board will approve, and design the simulation curriculum to INACSL Standards of Best Practice so it will withstand accreditor scrutiny.
Related Articles
Step 4: Secure Faculty, Clinical Sites, and Facility Resources
Securing the right people, places, and spaces turns your curriculum from paper to practice. This step demands both strategic hiring and tangible investments, because even the most innovative program fails without qualified educators, real-world training sites, and modern learning environments.
Recruiting Qualified Nursing Faculty
The nursing faculty vacancy rate is the single biggest bottleneck in nursing education today. In the 2025-2026 academic year, nursing schools nationwide reported 1,588 full-time faculty vacancies, a 7.2% vacancy rate, according to the American Association of Colleges of Nursing.1 In the Western region, that rate climbs to 9.8%.2 This shortage directly blocks expansion: more than 80,000 qualified nursing applicants were turned away in 2024, with insufficient faculty cited as the primary reason.3
Credential expectations drive hiring dynamics. About 81% of full-time faculty positions require or strongly prefer a doctoral degree (PhD or DNP), while roughly 18% accept a master's as the terminal credential, most often for clinical instructors.3 Most state boards mandate an MSN minimum for clinical faculty, with doctoral preparation expected for didactic, research, and leadership roles.
Staffing Benchmarks to Guide Your Budget
When planning your faculty roster, look to peer programs for scale. Whitworth University's new BSN, launching in fall 2027, plans for 10 full-time faculty plus adjuncts to support an initial cohort of 40 students, with the potential to expand to 80 students after 2031. Clinical instructor-to-student ratios typically max out at 1:8 or 1:10, depending on state regulations, so larger enrollments demand proportionally larger clinical faculty pools. Additionally, faculty time must be allocated for course development, accreditation preparation, and student mentoring, not just face-to-face teaching.
Securing Clinical Placements and Affiliation Agreements
Building clinical partnerships in nursing education is often make-or-break for program launch. Most state boards require formal affiliation agreements with hospitals, health systems, or community clinics before students begin rotations. These contracts generally cover liability insurance, student health and background check compliance, supervision responsibilities, and termination clauses. Negotiating these agreements early prevents delays in launching your first clinical courses. In competitive markets, build relationships with multiple partners and consider nontraditional sites such as public health departments, long-term care facilities, and telehealth providers.
Investing in Simulation and Physical Space
Physical infrastructure anchors the student experience. Whitworth's $3 million renovation of Hawthorne Hall created a 22,500-square-foot nursing education facility featuring high-fidelity manikins, simulation labs, and virtual reality tools. The program is designed so that up to half of required clinical hours can be completed in this simulated environment, a model that eases pressure on limited clinical placements while still meeting board requirements. As you budget, note that facility construction or renovation, simulation equipment, and technology licensing will be among your largest capital outlays, often requiring institutional investment, grants, or donor support.
Whitworth University's new BSN program offers concrete planning benchmarks: a $3 million renovation created 22,500 square feet of nursing education space, including simulation labs and high-fidelity manikins. The program budgeted for 10 full-time faculty positions and sized its initial cohort at 40 students, with capacity to scale to 80 once fully operational. Use these figures as a reference point when building your own business case and capital budget.
Step 5: Pursue National Accreditation, ACEN Vs. CCNE Vs. CNEA
Which accrediting body, ACEN, CCNE, or CNEA, should your new nursing program pursue? The answer depends on your program type, institutional philosophy, and long-term goals. While accreditation is technically voluntary, it is functionally essential: without it, students cannot access federal financial aid, employers may not recognize the credential, and the program loses credibility in a competitive academic landscape.
Understanding the Three National Nursing Accreditors
The Accreditation Commission for Education in Nursing (ACEN) accredits nursing programs at every level, from practical nursing through clinical doctorates and post-graduate residencies.1 Its process is prescriptive and policy-driven, with a strong emphasis on documented clinical competency and outcomes assessment.2 ACEN's standards reflect a meticulous approach that many long-established programs appreciate for its structure and clarity.
The Commission on Collegiate Nursing Education (CCNE) focuses exclusively on baccalaureate, master's, and Doctor of Nursing Practice programs, as well as post-graduate APRN certificates and nurse residencies.3 Aligned with the American Association of Colleges of Nursing (AACN) Essentials, CCNE emphasizes competency-based education and self-regulation. Institutions that already uphold the AACN framework often find CCNE's expectations a natural fit.
The National League for Nursing Commission for Nursing Education Accreditation (NLN CNEA) is the newest option, designed to be streamlined and innovation-friendly.4 It accredits pre-licensure programs at multiple levels, including LPN, ADN, BSN, and entry-level MSN, and some post-licensure tracks. CNEA's philosophy centers on the NLN's teaching-learning scholarship, making it appealing for programs that prioritize educational research and creative curricular design.
Comparing Costs and Timelines
- ACEN: The journey from application to initial accreditation typically spans 1.5 to 3 years. New programs first achieve candidacy, then undergo a site visit within two years.2 Fees include a candidacy application fee, site visit expenses, and annual dues, though exact amounts vary by institution.1
- CCNE: Expect a similar 1.5- to 3-year timeline. Programs start as new applicants and, if successful, receive a 5-year initial accreditation term (with the possibility of a 10-year term for established programs).2 Costs involve a new applicant review fee, on-site evaluation charges, and yearly continuation fees.3
- NLN CNEA: Pre-accreditation status can be attained within three years, after which programs must demonstrate full compliance with CNEA's 2026 standards (with a deadline of July 1, 2027, for those currently in progress).4 Expenses include application, pre-accreditation, site-visit, and annual fees.
While precise dollar figures are not published uniformly, all three bodies require a significant financial commitment. Budget for these costs early, and factor in ongoing compliance expenses such as annual reports and dedicated staff time.
Why Accreditation Is Non-Negotiable
Though you could theoretically operate an unaccredited nursing program, the practical consequences are severe. Students would be barred from federal Pell Grants and Direct Loans, making enrollment unfeasible for most. Many healthcare employers require graduation from an accredited program as a hiring condition, and tuition reimbursement plans often deny benefits to those without accredited credentials. Furthermore, state boards of nursing typically mandate national accreditation as a prerequisite for program approval or continued operation. If you are still weighing your leadership qualifications alongside this process, understanding what a nursing program director does can sharpen how you frame your program's administrative structure for reviewers. Selecting the right accreditor is not just a quality marker: it is a foundational step that determines your program's viability and your graduates' career prospects.
Step 6: Launch, Evaluate, and Continuously Improve
The tension between ambition and prudence defines your first years of operation. You want to graduate as many new nurses as the workforce demands, but enrolling too many students before your faculty, clinical sites, and support systems are battle-tested is the fastest way to produce poor outcomes and attract regulatory scrutiny. Start small, measure relentlessly, and scale only when the data tells you it is safe to do so.
Start Small and Scale Deliberately
Whitworth University's new BSN program offers a textbook example: an initial cohort of up to 40 students beginning in fall 2027, with plans to double enrollment to 80 only after 2031, once the program is fully operational and outcomes are established. This phased approach is the industry standard for good reason. A smaller inaugural class lets you identify curriculum gaps, calibrate simulation-to-clinical ratios, refine faculty workloads, and build preceptor relationships before the stakes multiply. Resist institutional pressure to fill every seat in year one. Your program's reputation will be written by the performance of that first graduating class.
Track the Metric That Matters Most: NCLEX Pass Rates
No single number carries more weight than your graduates' first-time NCLEX-RN pass rate. Most state boards of nursing set a minimum threshold, often 80 percent, and programs that fall below it face formal review, mandatory improvement plans, or probationary status that can restrict enrollment. Understanding NCLEX pass rate improvement strategies is essential before the first student sits for the exam. Build your assessment infrastructure early:
- Benchmark testing: Administer standardized readiness exams at multiple points in the curriculum so you can identify at-risk students early.
- Remediation protocols: Establish clear, documented pathways for students who do not meet progression benchmarks.
- Data dashboards: Report pass-rate trends to faculty and administration each semester, not just annually.
Treating NCLEX outcomes as a lagging indicator you check once a year is a recipe for surprises you cannot afford.
Adopt a Systematic Evaluation Plan
Both ACEN and CCNE expect programs to maintain formal, ongoing evaluation processes, not a binder you dust off before a site visit. Build a systematic evaluation plan from day one that tracks:
- Retention and graduation rates: Identify where students leave and why. Proactive nursing student retention strategies can reduce attrition before it damages your outcomes data.
- Employment outcomes: Survey graduates at six and twelve months post-graduation to capture job placement rates and employer satisfaction.
- Clinical partner feedback: Schedule annual meetings with preceptors and clinical site coordinators to surface concerns before they become deal-breakers.
- Student evaluations: Go beyond end-of-course surveys. Use focus groups and exit interviews to capture qualitative data that numbers miss.
Assign a faculty member or committee to own this process. Evaluation without accountability is just paperwork.
Plan for Curriculum Revision Cycles
Your curriculum is not a finished product on launch day. The NCLEX test plan is updated periodically by the National Council of State Boards of Nursing, and each revision can shift content emphasis in ways that ripple through your courses. Beyond NCLEX changes, you should expect to revise based on clinical site feedback (are students arriving prepared for the realities of the unit?), emerging evidence in nursing practice, and your own outcome data.
A practical cadence is to conduct minor course-level reviews annually and a comprehensive curriculum evaluation every three to five years. Document every change and the rationale behind it. Accreditors want to see that revisions are data-driven, not reactive.
Launching a nursing program is not a finish line. It is the start of a continuous improvement cycle that, done well, keeps your graduates competitive and your program in good standing for years to come.
Case Study: Whitworth University's New BSN Program
In fall 2027, Whitworth University will enroll up to 40 students in a new Bachelor of Science in Nursing, with plans to double capacity to 80 students annually after 2031.1 The program has already cleared two of the most consequential regulatory gates: approval from the Northwest Commission on Colleges and Universities and the Washington State Board of Nursing. It is a useful case study because Whitworth's path maps neatly onto the six-step framework, and because the choices the institution made are ones any nurse educator building a new program will face.
Aligning the Launch to the Framework
The needs assessment writes itself: Washington is projected to have the fifth largest RN shortage in the country through 2038, and national demand is expected to exceed supply by roughly 300,000 nurses by 2028.1 Whitworth's curriculum design meets standard BSN expectations with 600 clinical hours, and graduates will be eligible to sit for the NCLEX-RN. The prenursing track is being sunset: students enrolled in prenursing in 2027 will roll directly into the BSN, which preserves the existing pipeline rather than starting from zero.
Leadership and Facility Investment
Chris Sloan, DNP, RN, is serving as nursing administrator and program director. She previously led undergraduate nursing programming at Gonzaga. Hiring a director with regional program-building experience is a decision worth underlining: she brings existing relationships with Spokane-area clinical partners, familiarity with the state board, and credibility with prospective faculty. On the facility side, a $3 million renovation of Hawthorne Hall begins in September 2026, producing a 22,500-square-foot nursing education facility with simulation labs, high-fidelity manikins, and virtual reality tools.1
Simulation as a Clinical Placement Strategy
Up to half of the required clinical hours can be completed in simulation. This is the linchpin of the model. Spokane already hosts nursing programs at WSU Spokane, Gonzaga, EWU, and Spokane Community College, and those programs post strong local retention rates (74 to 99 percent staying in the region).1 Adding another program intensifies competition for hospital placements and preceptors, which is why building clinical partnerships in nursing education deserves attention well before the first cohort arrives. Whitworth's answer is to reduce dependency on scarce clinical seats by building the simulation capacity to substitute for them at scale. For educators planning their own launches, the takeaway is direct: if you cannot guarantee clinical placements, you must engineer around the bottleneck before you enroll students, not after.
Common Questions About Starting a Nursing Program
Whether you are drafting a feasibility report or presenting a proposal to your institution's leadership, these frequently asked questions cover the essentials of nursing program development. Each answer draws on the regulatory, curricular, and resource planning details discussed throughout this guide.
The needs assessment is where nursing programs are won or lost. Every subsequent step, state board approval, curriculum design, faculty hiring, accreditation review, traces back to whether that first document makes an airtight case for the program's existence.
Start with your state board's new program application requirements and work backward from them. Let those requirements drive your data collection, your workforce projections, and your institutional readiness review. The benchmarks are real: programs like Whitworth's invested three million dollars in facilities and planned for ten full-time faculty before enrolling a single student. Your case needs that same rigor. Proactive nursing student retention strategies should be built into your plan from the start, because regulators and accreditors will scrutinize not just how many students you enroll but how many you graduate. Every year a region waits for a new program is another graduating class it never produces, and another year the shortage deepens.