What you’ll learn in this article…
- WVU Medicine opened a 15,000-square-foot education center in Wheeling in June 2026.
- Simulation labs expand training capacity without relying on hospital preceptors.
- West Virginia invested over $90 million since 2022 to expand nursing workforce.
How is WVU Medicine addressing the nursing shortage in the Ohio Valley? In June 2026, the health system opened a 15,000-square-foot nursing education center in Wheeling, directly confronting a regional crisis that has left hospitals understaffed.1 The facility houses simulation labs and bedside training capacity, creating a direct pipeline from classroom to clinic within the hospital network.
For nurse educators, this represents more than a building. A major hospital system is not waiting for academic partners to scale up; it is building its own workforce solution. The center arrives amid West Virginia's record nursing vacancies and a nursing faculty shortage that limits traditional program growth. The model in Wheeling tests whether employer-operated education can break the training bottleneck that has long constrained the nation's nursing pipeline.
Why the Ohio Valley Faces a Critical Nursing Shortage
West Virginia's nursing shortage runs deeper than the national crisis, and quick fixes like recruitment bonuses or travel nurse contracts cannot patch a pipeline that lacks enough training slots to begin with. As of 2026, the state faces an estimated deficit of 3,860 registered nurses, with supply meeting only 81 percent of demand.1 The RN-to-population ratio sits at 9.46 per 1,000, well below what an aging and rural state requires.2 While national RN vacancy rates hover around 15 percent in some benchmarking reports, West Virginia posted a 19.3 percent vacancy rate in hospitals as recently as 2024, a figure that has likely held steady or worsened into 2026.3
Why the Ohio Valley Feels the Shortage More Acutely
The Ohio Valley region compounds these statewide challenges with geographic isolation and a limited number of clinical placement sites. Many nursing education programs rely on hospitals and clinics to give students hands-on experience, but in rural corners of the Northern Panhandle, those sites are both fewer and smaller. Compounding the problem, the existing nursing workforce in the Ohio Valley skews older, with retirements accelerating the exodus. Without accessible training pipelines that keep graduates local, newly licensed nurses often leave for higher-paying markets in Pennsylvania or Ohio, perpetuating a cycle of understaffing.
The Faculty Bottleneck: Turning Away Qualified Students
A less visible but equally damaging barrier sits inside nursing schools: West Virginia programs cannot expand enrollment because they lack enough nursing faculty. Nationally, nursing schools turned away over 65,000 qualified applicants during the 2023 cycle, and a nursing faculty shortage persists across the country, with a 7.8 percent full-time faculty vacancy rate.4 In Appalachia, the numbers feel even tighter: doctoral-prepared instructors are rare, and experienced nurses can earn significantly more in clinical roles than in teaching positions. As a result, West Virginia nursing programs are unable to fill seats, not because students are not applying, but because there is no one to teach them. The faculty shortage acts as a choke point directly upstream of the bedside shortage.
Why Quick Fixes Are Not Enough
Hospitals across West Virginia have tried recruitment bonuses, international hiring, and contract travel nurses to fill gaps, but these are stopgaps: expensive and temporary. They do nothing to increase the total number of nurses entering the profession. A lasting solution requires building new training capacity, including simulation labs and additional clinical education spaces like the WVU Medicine center in Wheeling. By doubling down on education infrastructure, the state can address the root cause rather than just the symptom.
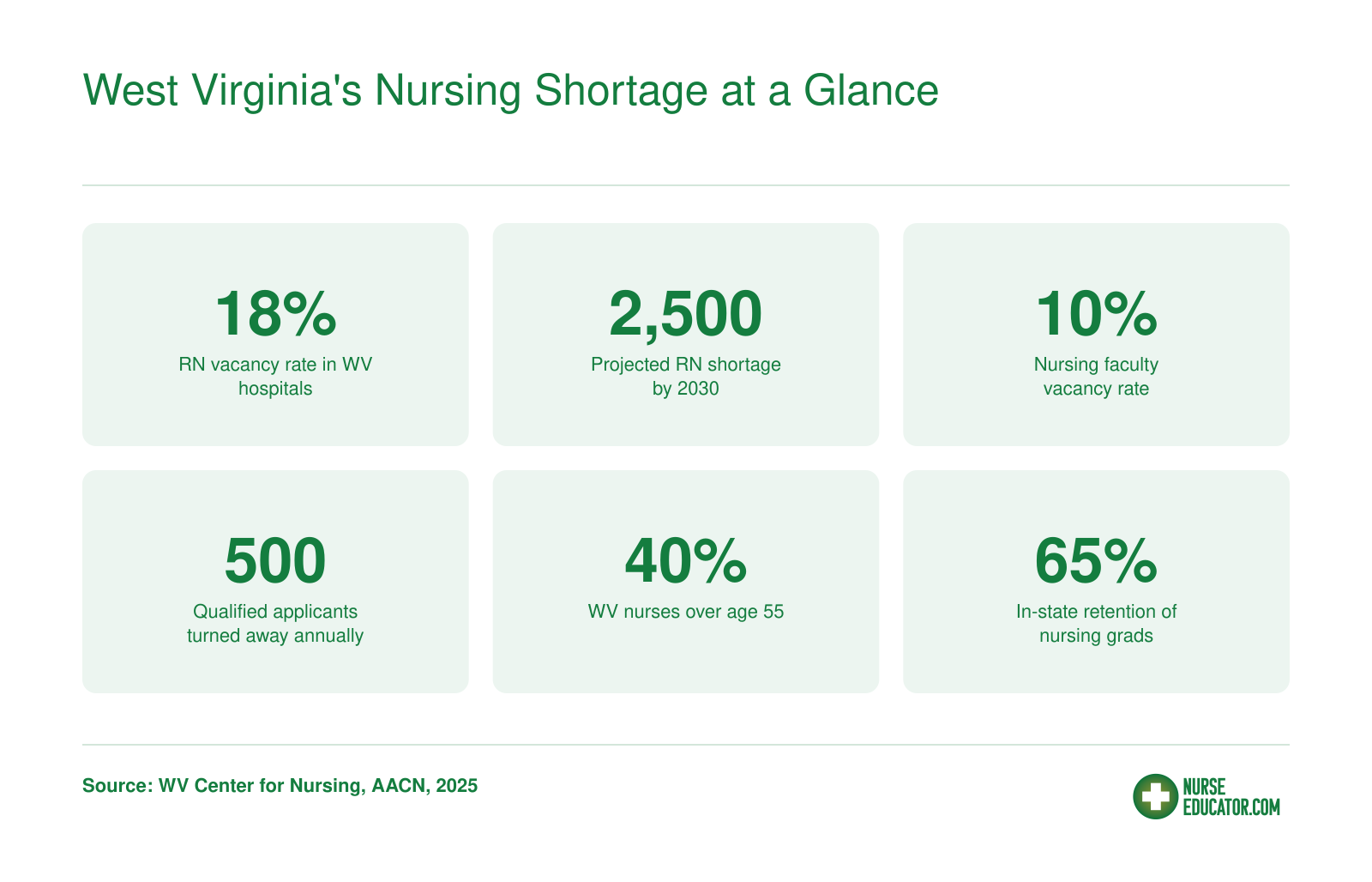
West Virginia's Nursing Shortage at a Glance
The new WVU Medicine education center in Wheeling arrives as West Virginia faces one of the nation's most acute nursing shortages. The numbers below paint a stark picture of the gap between workforce supply and patient demand.
What WVU Medicine's Wheeling Education Center Offers
WVU Medicine opened its Wheeling nursing education center in June 2026, housed within the WVU Medicine Operations Support Center on the Wheeling University campus.1 The 15,000-square-foot facility directly targets nursing shortages in the Ohio Valley by training bedside-ready nurses inside a clinical health system rather than through a traditional academic college.2
A Hospital-Embedded RN Diploma Program
Unlike a conventional nursing school, the center operates a diploma program: a 21-month track slated to launch its first cohort in August 2027, with applications due October 6, 2026.3 The program accepts just 26 students, focusing exclusively on bedside nursing competency. WVU Medicine eliminates financial barriers by covering full tuition, books, and supplies , a zero-cost education in exchange for a three-year bedside employment commitment after graduation.1 This model serves individuals unable to pursue a traditional four-year BSN, widening the pipeline while guaranteeing a dedicated workforce for the health system.
Simulation and Skills Labs
The center's physical footprint includes a simulation center, a virtual reality lab, and clinical skills labs that mirror acute-care settings.4 Students practice high-stakes scenarios, including cardiac emergencies, difficult conversations, and rapid response protocols, before they ever touch a live patient. Repeated deliberate practice in these environments builds the clinical judgment and muscle memory essential for new graduates entering fast-paced medical-surgical or intensive care units.
Part of a Regional Workforce Strategy
WVU Medicine now runs nursing education centers in Morgantown, Martinsburg, and Wheeling, signaling a larger investment in Ohio Valley infrastructure and academic-practice partnerships in nursing.1 By controlling the entire training pipeline, from recruitment and education through preceptorship and eventual hire, the system can tailor curricula to its patient population and staffing needs. For nurse educators, this represents a growing model where clinical employers partner with academic institutions and influence both curriculum design and simulation pedagogy, producing graduates who are truly practice-ready on day one.
How Simulation Labs and Hospital Partnerships Expand Training Capacity
Simulation labs and hospital-operated education models directly tackle the clinical placement bottleneck that has long capped nursing school enrollments. By decoupling training hours from the limited availability of hospital floor preceptors, these innovations make it possible to educate more nurses without overwhelming clinical sites.
The Clinical Placement Bottleneck and How Simulation Relieves It
Traditional nursing programs compete fiercely for a finite number of hospital-based clinical slots. Each student requires direct supervision from a staff nurse or clinical instructor, and patient safety concerns cap the student-to-preceptor ratio. This physical constraint means that even well-funded schools often must turn away qualified applicants. High-fidelity simulation labs break that logjam by providing a controlled, risk-free environment where students can practice assessments, interventions, and crisis management without occupying a bed or dividing a preceptor's attention. Many state boards of nursing, including West Virginia's, now allow high-fidelity simulation to substitute for a significant portion of traditional clinical hours. The Wheeling education center's dedicated simulation suites thus directly expand the region's clinical placement evaluation for nursing students, ensuring learners meet competency benchmarks before stepping onto a live unit. With scenarios that replicate real bedside challenges, from routine medication administration to rapid-response emergencies, simulation builds competence and confidence before students ever step onto a live unit.
The Hospital-Operated Education Model: A New Kind of Partnership
WVU Medicine isn't just a clinical site for a partner school; it is the school. This hospital-operated education model flips the traditional academic-practice partnership model for nursing education on its head. Instead of negotiating preceptor placements across multiple institutions, WVU Medicine embeds faculty and preceptors directly within its own facilities, with curricula designed to match its patient populations and care protocols. Students train inside the health system they may one day join, absorbing its culture, standards, and workflows from day one. This seamless integration means no handoff friction between classroom and bedside. Preceptorships are built into the employment pipeline; students often rotate through units where they'll receive job offers. The Wheeling center's design centralizes this model, co-locating classrooms, simulation labs, and clinical floors under one organizational roof.
Faster Onboarding, Lower Turnover, and a Workforce That Stays Local
The payoff is measurable: graduates of hospital-embedded programs require shorter orientation periods because they're already socialized to the system's electronic health records, equipment, and team structures. Turnover drops when nurses feel a strong cultural fit from the start, and local recruitment means these professionals are more likely to put down roots in the Ohio Valley. WVU Medicine's investment in simulation not only speeds the scaling of its education pipeline but also ensures that every new nurse has rehearsed high-stakes scenarios before they're ever counted in a staffing ratio. The result is a self-reinforcing cycle: expanded training capacity leads to more graduates, who fill local vacancies and reduce reliance on expensive travel nurses, which in turn stabilizes the workforce and allows the health system to invest further in education infrastructure.
Related Articles
What This Means for Nurse Educators and Faculty Recruitment in WV
The opening of WVU Medicine's nursing education center in Wheeling signals more than expanded training capacity for students. It introduces a new model of nursing education that directly opens doors for nurse educators. For professionals in West Virginia considering or already in teaching roles, this center creates tangible career opportunities that blend clinical expertise with educational delivery outside the traditional academic structure.
New Faculty Roles Emerging from the Simulation Lab
Facilities like the Wheeling center generate positions seldom seen in conventional nursing programs. Simulation lab directors manage high-tech learning environments, develop scenario-based curricula, and ensure equipment fidelity. Clinical coordinators bridge the gap between classroom learning and bedside practice, often working directly with hospital units to design preceptor experiences. Curriculum designers who specialize in simulation pedagogy are needed to build immersive, evidence-based modules. These roles reward hands-on clinical judgment and teaching ability, and they often do not require a tenure-track appointment. For educators who want to remain close to patient care while mentoring students, such roles offer a compelling alternative.
The Salary Gap and Incentives That Could Make a Difference
West Virginia's hospital nursing roles reflect a competitive market: in 2024, the state's hospital nursing vacancies stood at 19.3% with turnover at 26.3%.1 Clinical salaries have risen to attract and retain bedside nurses, while academic faculty pay frequently lags. This disconnect is a central reason nursing schools nationwide reported 1,588 full-time faculty vacancies in 2025 and turned away over 80,000 qualified applicants.2 Hospital-based education centers can narrow this gap by offering clinical pay scales to teaching staff, a model that aligns compensation more closely with the market. Federal programs already exist to make academic roles more viable: the nurse faculty vacancy rate nationwide reached 7.2% in 2025, and programs like the Nurse Faculty Loan Program, which cancels up to 85% of loans for educators who serve four years, and the Faculty Loan Repayment Program, which provides up to $40,000, offer meaningful relief.3 West Virginia could build on such foundations with state-level loan forgiveness or service scholarships, similar to the West Virginia Nursing Scholarship Program, which saw 88.7% of its completers maintain active licenses.1
Hospital-Based Teaching: Flexibility and Proximity
For nurses who love teaching but dread the rigidity of academia, hospital-based educator roles at centers like Wheeling offer flexible scheduling and immediate access to real patient care environments. These positions can be structured as full- or part-time, often with shift options that accommodate family life or continued clinical practice. They allow educators to demonstrate skills at the bedside and in simulation simultaneously, reinforcing theory with practice. This hybrid model may attract mid-career nurses becoming educators who might otherwise avoid teaching due to perceived red tape or reduced income.
Simulation Roles Widen the Faculty Pipeline
Perhaps the most strategic benefit is that simulation-focused teaching positions can lower the credential barrier. While many traditional faculty roles demand a doctoral degree, simulation education often prioritizes clinical experience, certification in simulation instruction, and demonstrated teaching ability. This allows nurses with an MSN or a BSN plus specialty certification to transition into education without the time and expense of a PhD or DNP. By creating a more accessible on-ramp, West Virginia can enlarge its pool of qualified educators, helping to address the 7.2% national faculty vacancy rate2 in a region that urgently needs more graduates.
How WV's Statewide Strategy and Replicability Shape the Future
West Virginia has committed over $90 million to nursing workforce expansion since 2022, and the newly opened WVU Medicine Nursing Education Center in Wheeling is one visible result of that sustained investment.
Statewide Strategic Initiatives Already Underway
The Governor's Nursing Workforce Expansion Program channels funds through the West Virginia Higher Education Policy Commission and Community and Technical College System.1 Its core components, including nursing career pathways, Junior/Senior Nursing Academies, a fully funded scholarship program, and direct grants to nursing schools, are all active as of 2025-2026. The state reports a 25% increase in filled nursing program seats since the initiative launched,2 alongside a 15% rise in associate-degree RN graduates between 2022 and 2023.3 Overall, West Virginia graduated 15% more nurses in 2023 than a decade earlier.3 Twenty-three expansion grants were awarded in the 2024-2025 cycle alone,2 with multiple community colleges and universities receiving substantial sums to grow their programs.
Connecting the Wheeling Center to the Broader Strategy
The Wheeling center extends this momentum into clinical education. By building simulation labs and training space within a major health system, it addresses a frequent bottleneck: adequate clinical placement capacity. The center's emphasis on bedside care aligns with state goals to produce practice-ready nurses who stay in West Virginia. When WVU Medicine places this center in the Ohio Valley, it leverages a region where access to nursing programs has been limited, making every new graduate a direct pipeline for local hiring.
What Makes This Model Replicable
- Health system footprint: WVU Medicine operates across West Virginia, giving it the patient volume and preceptor pool to sustain a teaching center. Other regional systems may follow suit.
- Supportive regulatory environment: West Virginia's approach to counting simulation hours toward clinical requirements lowers the barrier for non-traditional education sites, so hospital-operated centers can meet state standards without an entire college infrastructure.
- Underserved community need: The Ohio Valley lacked sufficient nursing education infrastructure, making it prime for a hospital-operated training hub. Similar regions across Appalachia and rural America share that profile.
Barriers and a Look Ahead
- Accreditation timelines: New nursing programs, even those embedded in hospitals, must meet state board and national accreditation standards, a process that can take years.
- Faculty recruitment remains the universal bottleneck: Finding experienced nurses willing to become nurse educators is tough everywhere, but especially in rural areas. WVU Medicine may need to invest heavily in adjunct and clinical instructor pipelines.
As nursing shortages persist nationally, hospital-operated education centers may shift from a rarity to a recognized workforce strategy. West Virginia's multi-year investment and early outcomes offer a template, but scaling it hinges on solving the nursing faculty shortage and ensuring graduates stay in-state. For now, the Wheeling center demonstrates that when a health system, state funding, and higher education institutions align, new capacity can come online faster than rebuilding traditional programs alone.
Key Takeaways for Nurse Educators Watching This Space
The opening of WVU Medicine's new clinical education center in Wheeling raises important questions for nurse educators about training capacity, faculty roles, accreditation, and scalability. Here are grounded answers to the most pressing questions.