What you’ll learn in this article…
- In 2023, U.S. nursing schools turned away 65,766 qualified applicants due to clinical placement and faculty shortages.
- McLeod Health's $75,000 contribution to Francis Marion University funds faculty development and clinical training.
- Communication gaps, not funding, remain the most cited barrier to clinical partnership success.
The U.S. will need to fill 194,500 registered nurse positions annually through 2032, but in 2023 nursing schools turned away 65,766 qualified applicants because there were not enough clinical placements or faculty to train them. This bottleneck, largely fueled by the nurse educator shortagenurse educator shortage, has transformed academic-practice partnerships from a nice-to-have into the central strategy for expanding educational capacity and building an adequate nursing workforce.
McLeod Health's recent $75,000 commitment to Francis Marion University's nursing programs, including its Nurse Educator track1, is one concrete example of investment in that infrastructure. Such direct funding sustains both student clinical rotations and the pipeline of future nursing instructors. For nursing programs, cultivating these alliances is no longer optional; it is a structural requirement for survival.
What Are Clinical Partnerships in Nursing Education?
Today's nursing education landscape is defined by a deliberate shift away from siloed training toward deeply integrated academic-practice partnerships. At their core, these partnerships are formal, mutually beneficial alliances between nursing schools and healthcare delivery organizations. They go far beyond simple clinical placement arrangements; they represent a shared commitment to preparing graduates who can step into practice with competence and confidence.
Bridging the Classroom-to-Practice Gap
Academic-practice partnerships create a structured bridge where classroom theory meets real patient care. Students gain supervised, hands-on experience in authentic clinical environments, applying concepts like pathophysiology, pharmacology, and health assessment under the guidance of experienced preceptors, building clinical judgment. This direct application accelerates the transition from learner to practitioner, reducing the reality shock that can occur when new graduates face the complexities of contemporary healthcare delivery.
Strengthening Student Readiness and Workforce Supply
When partnerships function effectively, they enhance student readiness by aligning educational curricula with the current needs of practice. Healthcare organizations help shape learning objectives and expose students to the technologies, documentation systems, and interprofessional workflows they will encounter on the job. Equally important, by expanding clinical training capacity, these alliances directly address the national nursing shortage. With more clinical placements available, programs can increase enrollment and graduate more practice-ready nurses, ultimately strengthening the workforce pipeline.
Interprofessional Education: A Growing Component
A growing dimension of clinical partnerships is interprofessional education (IPE). Instead of training in isolation, nursing students increasingly collaborate alongside medical, pharmacy, respiratory therapy, and other health professions students during clinical rotations and simulation exercises. This team-based approach builds the communication and collaboration skills essential for safe, high-quality patient care. Well-designed partnerships intentionally create IPE opportunities, reflecting the reality that effective healthcare delivery depends on seamless teamwork across disciplines.
In 2023, U.S. nursing programs turned away 65,766 qualified applicants, according to the American Association of Colleges of Nursing. The primary reasons: a shortage of nursing faculty and an inability to secure enough clinical placement slots for students. This stark number highlights why building clinical partnerships is essential.
Key Types of Clinical Partnership Models
Dedicated education units and student-employee programs represent two ends of the clinical partnership spectrum, each with distinct structures, oversight needs, and outcomes. While one emphasizes a teaching-focused hospital unit staffed entirely by students and clinical faculty, the other integrates student learning directly into paid patient care roles. Understanding the core models helps nursing programs and clinical agencies pick the approach that aligns with their resources, regulatory landscape, and workforce goals.
Dedicated Education Units (DEUs)
In a dedicated education unit, a hospital unit or a portion of a unit is set aside solely for nursing student clinical experiences. Staff nurses serve as clinical instructors in close collaboration with academic faculty, creating an immersive teaching environment. This model often improves student confidence, clinical reasoning, and transition-to-practice readiness because learners work under consistent preceptors who have received targeted training in education methods. The National League for Nursing and the American Nurses Association have highlighted DEUs in published case studies, noting higher student satisfaction and stronger faculty-practice relationships. Successful DEUs require clear communication channels, shared governance of the unit’s educational mission, and a structured clinical placement evaluationclinical placement evaluation to monitor student competency and patient outcomes.
Student-Employee Partnership Models
Student-employee models allow nursing students to hold paid patient care positions, such as nurse externs or patient care technicians, while enrolled in a nursing program. The clinical hours logged in these roles may count toward program requirements, but only if the arrangement meets state board of nursing regulations. Many state boards outline specific rules for supervision, licensure levels of supervising nurses, and the maximum ratio of student-employees to preceptors. Some boards also govern whether credit-for-work can replace or supplement traditional clinical rotations. Before adopting this model, nursing programs typically review their state’s nurse practice act and position statements on student employment, ensuring the partnership does not blur the line between education and service delivery in ways that could jeopardize licensure eligibility.
Nurse Residency-Linked Academic Partnerships
A third model links academic nursing programs directly to hospital-based nurse residency programs. In this structure, students complete their final clinical immersion on a unit where they will likely transition into a residency after graduation. The hospital invests early in the student’s development, and the academic partner aligns its curriculum with the precepted experience and evidence-based practice projects threaded through the residency year. These partnerships often report stronger new-graduate retention and shorter time-to-competency, though formal comparative outcome data remains emerging. BLS.gov workforce projections and individual school outcomes pages sometimes cite improved retention rates for residency-linked models, giving nursing education leaders a starting point for data-informed conversations with hospital administrators.
Choosing the Right Model
No single model fits every context. A rural community college may gravitate toward a student-employee arrangement to expand placement capacity, while an academic medical center may have the infrastructure to sustain a DEU. Nursing programs often explore multiple models simultaneously, tailoring each partnership to the clinical agency’s patient population, staffing patterns, and preceptor availability. The decision should be grounded in a review of applicable board of nursing rules, faculty and preceptor workload capacity, the ongoing nursing faculty shortagenursing faculty shortage, and a clear-eyed assessment of the resources needed to maintain quality and safety in each type of clinical education structure.
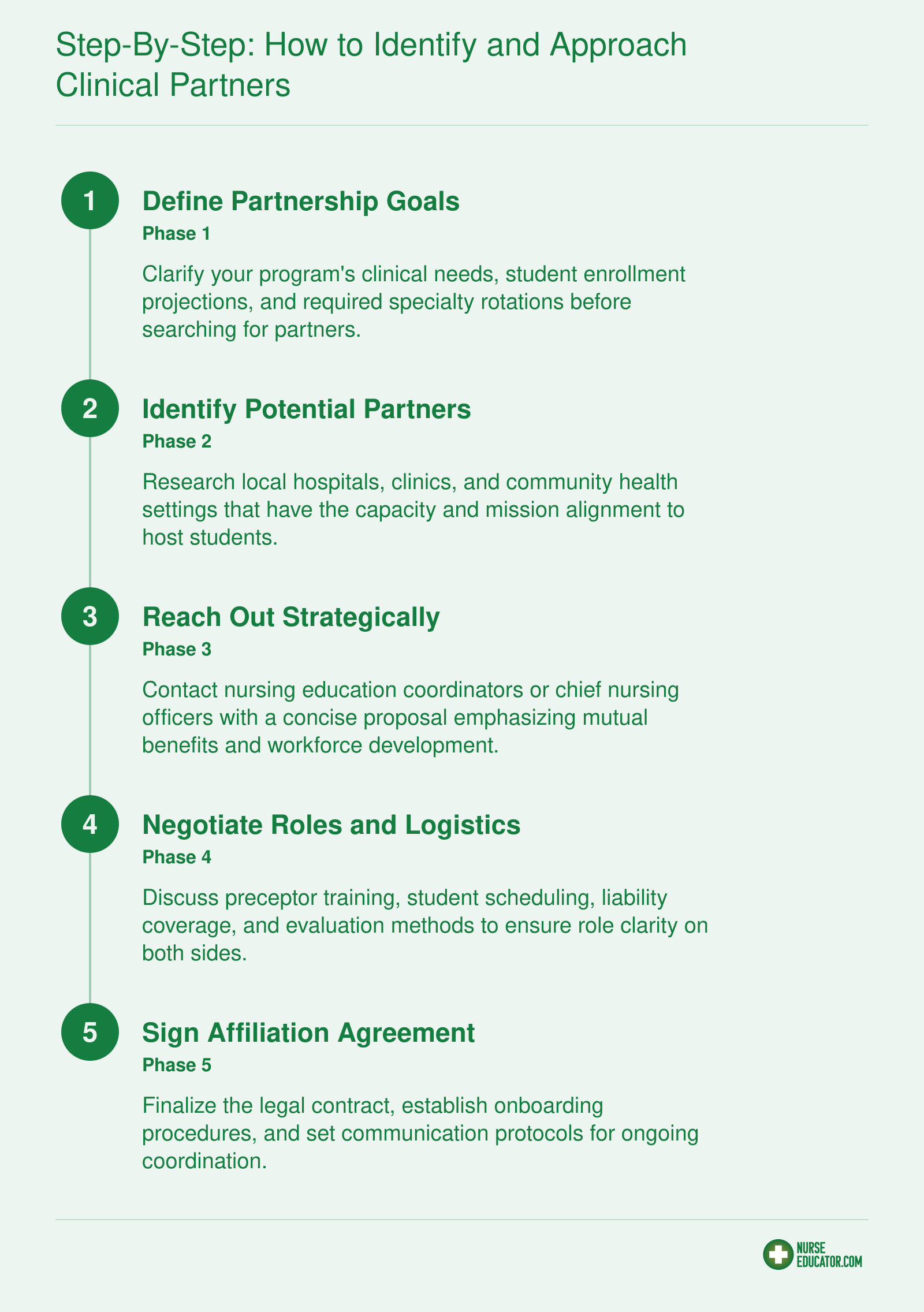
Step-By-Step: How to Identify and Approach Clinical Partners
Strong clinical partnerships don't happen by chance, they are built through intentional, well-sequenced outreach. Follow this pathway to move from identifying a potential site to signing a mutually beneficial affiliation agreement.
Negotiating Affiliation Agreements: Key Contract Elements
Negotiating an affiliation agreement often feels like a tug-of-war between protecting your institution's legal and financial interests and building the genuine trust that makes a clinical partnership actually work. The agreement isn't just paperwork: it's the structural backbone that defines how the school and the healthcare facility share responsibility for students, preceptors, and patient care.
Essential Contract Components
A strong agreement addresses four areas explicitly. First, governance: spell out who has decision-making authority for student placements, scheduling changes, and performance issues. Without a clear escalation path, small disagreements can stall an entire cohort.
Second, resource sharing details: storage for student belongings, documentation access, EMR logins, simulation lab time, meeting space, even parking. Vague language leaves preceptors scrambling to find space on the first day. Third, liability and insurance: specify who provides malpractice coverage for students, what happens when a student error triggers a claim, and whether the facility extends its own coverage during clinical hours. Many schools rely on their own policies, but not all facilities will accept that without explicit indemnification language.
Fourth, operational roles: define what the clinical instructor, staff preceptor, and unit manager are each accountable for. Ambiguity here is the most frequent source of friction, especially around evaluation and remediation responsibilities.
Common Pitfalls and How to Dodge Them
- Overnegotiating minor details: Spending weeks on custodial versus instructional responsibilities delays student access. Treat the contract as a living document that can be amended.
- Missing data sharing protocols: If you don't address HIPAA and FERPA alignment upfront, partners may restrict observation opportunities later.
- Assuming preceptor availability: A contract that requires staff preceptors without confirming their capacity or providing training support sets the partnership up for burnout.
Building Mutual Accountability
Move beyond a transactional lease-on-a-unit mindset. Tie agreement terms to a joint advisory committee with scheduled quarterly reviews. Write in clear communication channels: who notifies whom when a student is absent, when a preceptor is reassigned, or when a safety incident occurs. Use language that frames the partnership as a shared investment in the region's future nursing workforce, not a one-way transaction. When both signatories see the agreement as a tool for equitable risk-sharing and quality improvement, the contract becomes the foundation for a sustainable, evolving relationship.
Questions to Ask Yourself
Role Clarity and Support for Clinical Preceptors
Clinical preceptors are the practicing nurses who directly supervise and mentor students during clinical rotations, turning classroom knowledge into bedside competence. A clear, well-supported preceptor role is the foundation of every effective academic-practice partnership.
Selecting the Right Preceptors
Establishing clear selection criteria sets expectations from the start. Most partnerships look for registered nurses with at least a BSN (many prefer or require an MSN) and a minimum of two to three years of bedside experience in the relevant clinical area. Beyond credentials, effective preceptors demonstrate strong communication skills, a genuine interest in teaching, and solid time-management abilities. Using a brief application or interview with the academic partner helps confirm that the nurse is not only clinically competent but also motivated to mentor.
Preceptor Training and Continuing Education
Even experienced nurses benefit from structured preparation. While no single national standard exists, current practice guides recommend 8 to 16 hours of initial training that covers clinical teaching strategies, student evaluation, and common preceptor challenges. An annual refresher of 4 to 8 hours keeps skills current and addresses emerging practice issues. The NLN Commission for Nursing Education Accreditation requires that programs allocate adequate resources for clinical learning, and that includes preceptor development.1 Many partnerships award CE or CNE credits to reinforce the value of training. For example, the AACN Clinical Nurse Educator Academy delivers 9.75 to 15 contact hours, showing how academic organizations are investing in preceptor education.1
Managing Workload to Prevent Burnout
Combining a full patient load with student supervision quickly leads to nurse educator burnout. The gold standard student-to-preceptor ratio is 1:1, though 1:2 is acceptable in exceptionally stable settings. To protect teaching time, many health systems reduce the preceptor's patient assignment by one to two patients. A tiered support model (unit-based preceptor, a dedicated clinical nurse educator, and an accessible academic faculty liaison) distributes the load and ensures preceptors have backup when questions or safety concerns arise. The faculty liaison should be consistently available to clarify learning objectives and step in if a student or preceptor needs additional support.
Compensation and Recognition Models
Precepting is a significant professional contribution that deserves both financial and institutional recognition. Common compensation approaches include: - Per-student stipend: A flat fee for each student over a semester. - Hourly adjunct pay: Compensation for direct teaching and mentoring time. - Retention bonuses: Bonuses awarded after completing a set number of rotations.
Nonmonetary recognition is equally important. Strategies that work well include: - CE/CNE credits: Pair training and assessment activities with accredited contact hours. - Academic titles: Designate preceptors as adjunct clinical faculty. - Conference access: Offer priority registration and travel support. - Annual awards: Celebrate outstanding preceptors during Nurses Week or partnership events.
Formalizing these benefits in the partnership memorandum of understanding (MOU) clarifies role expectations and signals that the organization truly values preceptor development.
Evaluating Partnership Effectiveness: Metrics and Tools
Measuring the success of a clinical partnership is not a once-a-year checkbox exercise. It is an ongoing process of collecting meaningful data, interpreting trends, and using those insights to strengthen the collaboration. Without a structured evaluation approach, even well-intentioned partnerships can drift, misalign, or fail to deliver on their promise.
Key Metrics That Matter
Effective evaluation begins with identifying the right combination of outcomes. Most nursing education partnerships track a mix of student, workforce, and partnership health indicators:
- NCLEX pass rates: These remain a fundamental benchmark, reflecting how well clinical preparation translates into licensure readiness.
- Job placement and retention: Tracking whether graduates are hired by the partner organization and remain in those roles over time signals the partnership's workforce impact.
- Preceptor and student satisfaction surveys: Structured feedback from both sides reveals how well the clinical environment supports learning, communication, and role clarity.
- Clinical quality indicators: When partner hospitals share unit-level data on safety, infection rates, or patient outcomes, nursing programs can evaluate whether their students contribute to a culture of quality.
Many institutions now compile these metrics into outcome dashboards that are reviewed jointly by academic and practice leaders at quarterly or biannual meetings. The dashboard becomes a shared mirror, making it easier to spot trends, celebrate wins, and address gaps before they escalate.
Standardized Toolkits for Consistent Measurement
Relying solely on homegrown metrics can make it difficult to compare performance across partnerships or align with national standards. Several nationally recognized frameworks exist to bring structure and credibility to the evaluation process.
The American Association of Colleges of Nursing (AACN) offers the Academic-Practice Partnerships Implementation Tool Kit, which helps partners jointly define goals and select measurable outcomes across education, workforce, quality, and partnership process domains. Schools use it to embed evaluation into clinical experiences and conduct data-driven reviews.
A complementary resource is the Academic Practice Partnership Playbook from AACN and the American Organization for Nursing Leadership (AONL). It guides teams through identifying shared goals and tracking outcomes across education, workforce, and quality, while also offering strategies for refining clinical placement models. Many nursing programs pair these tools with the Partnership Expectation and Outcome Matrix and the Partnership Metrics Worksheet to create a customized, living evaluation plan.6
For direct clinical evaluation, tools that embody the AACN BSN Essentials and QSEN competencies use a 0-to-4 scale for safety, evidence-based practice, informatics, and quality improvement. Aggregated scores from these clinical evaluation forms offer a data-rich view of the learning environment's strengths and weaknesses.5
Longitudinal Tracking and Continuous Improvement
Snapshot evaluations are useful, but the real value lies in watching trends over time. Strong partnerships track the same core metrics year after year, allowing them to identify whether improvements are sustained or if new challenges are emerging. Longitudinal data might reveal, for example, that preceptor satisfaction drops as a cohort size increases, or that job placement rates improve after a revised onboarding process.
Continuous improvement cycles follow naturally from longitudinal tracking. Partners review dashboard data, pinpoint one or two priority areas, pilot an adjustment, and then reassess. This iterative rhythm transforms the relationship from a transactional placement arrangement into a true academic-practice partnership. It also creates a culture where both sides are accountable for outcomes and invested in each other's success.
Snapshot: What Successful Partnerships Achieve
Clinical partnerships directly improve nursing education outcomes. A review of partnership-based NCLEX prep programs shows striking pass rate gains.

Case Studies: Successful Clinical Partnerships in Action
What do successful clinical-academic partnerships look like in practice? The strongest collaborations share a common thread: they go beyond transactional placement agreements to create truly integrated learning ecosystems. Below, we examine three partnerships that demonstrate how shared investment, role clarity, and long-term vision can produce measurable gains in nursing education.
McLeod Health and Francis Marion University: Investing in the Educator Pipeline
In June 2026, McLeod Health made a $75,000 contribution to Francis Marion University (FMU) to help maintain and strengthen its nursing programs. Tony Derrick, Chief Nursing Officer for McLeod Regional Medical Center, framed the gift as a direct response to the national nursing shortage and the growing demand for healthcare services driven by an aging population. What sets this ongoing partnership between McLeod Health and Francis Marion University apart is its dual focus: the funding supports not only general nursing students but specifically FMU's Nurse Educator program, a pipeline that will produce future nursing faculty.
Dr. Fred Carter, president of Francis Marion University, noted that McLeod's ongoing commitment has translated into scholarship support and expanded clinical training opportunities for FMU students. By explicitly earmarking resources for the Nurse Educator track, the partnership addresses the bottleneck in nursing education: without enough qualified instructors, programs cannot grow to meet workforce demand. For nurse educators and academic leaders reading this, the takeaway is clear. Sustainable clinical pipelines depend on investing in the faculty who will oversee those placements.
UMKC and Clinical Partners: A 100% NCLEX Pass Rate
At the University of Missouri-Kansas City (UMKC), a collaborative model with multiple clinical partners has yielded a standout outcome: a 100% first-time NCLEX pass rate for its graduating cohort in 20241 as documented by the Missouri Board of Nursing. While UMKC's curriculum and simulation resources are strong on their own, university leaders attribute much of the exam success to the depth and quality of clinical placements secured through long-standing agreements with regional health systems.
These partnerships are built on a shared clinical faculty model, where seasoned practice professionals are jointly appointed by the university and the healthcare organization. This arrangement ensures that preceptors are not only clinically expert but also well-versed in the program's learning objectives, creating a seamless bridge between coursework and bedside experience. The partnership actively tracks competency milestones across placements, using shared dashboards that give academic and clinical educators real-time visibility into student progress. For programs looking to replicate this success, the UMKC example underscores the value of shared governance and data transparency.
NewYork-Presbyterian and Columbia University School of Nursing: The LINK Program
NewYork-Presbyterian and Columbia University School of Nursing have partnered on the LINK program2, a clinical education model designed to immerse students in practice environments for extended, uninterrupted rotations. Unlike traditional models where students rotate through multiple short placements, LINK participants remain on a single unit for a full semester, working alongside the same preceptor team and caring for a consistent patient population.
This continuity has paid dividends in student satisfaction and clinical judgment development. Program evaluations indicate that students in the LINK model report significantly higher confidence in decision-making and stronger interprofessional communication skills than peers in conventional rotations. Employers within the NewYork-Presbyterian system note that LINK graduates transition into practice with less orientation time and greater readiness for complex patient care. While formal job placement rates for the program are not publicly reported, the partnership's longevity and the system's ongoing investment speak to its perceived value on both sides.
Key Lessons for Your Own Partnership Development
Across these three case studies, several actionable lessons emerge:
- Invest in educators, not just placements. The McLeod-FMU contribution highlights that solving the clinical placement crisis begins upstream, with a steady supply of qualified nursing faculty.
- Share governance and data. UMKC's joint faculty model and transparent progress tracking show that true collaboration means both academic and practice partners hold a stake in student outcomes.
- Design for continuity. The LINK program's semester-long immersion demonstrates that deeper, sustained clinical relationships can produce stronger clinical thinkers than rapid rotation models.
- Measure what matters. Each partnership ties its model to concrete outcomes: NCLEX pass rates, readiness-to-practice indicators, and scholarship-supported enrollment growth. Define success metrics early and revisit them together.
These examples prove that when health systems and nursing schools move beyond transactional agreements toward genuine academic-practice integration, the entire nursing workforce benefits.
Funding Models and Financial Sustainability
The greatest tension in clinical partnerships often isn't philosophical alignment; it's the delicate balance between the immediate costs of training placements and the long-term investment required to build a sustainable nursing workforce. Schools face constrained budgets, while hospitals weigh the ROI of dedicating staff time and resources to student education. The partnerships that thrive are those that treat funding as a shared, strategic commitment rather than a series of one-off transactions.
Shared Cost Models Between Schools and Health Systems
A common starting point is joint funding for dedicated educator positions. The clinical instructor partner model illustrates this well: a health system may fund approximately a 0.7 FTE clinical instructor role, while the academic institution covers the remaining 0.3 FTE and provides curricular oversight. This structure gives students consistent, clinically immersed faculty while relieving the school of the full salary burden.2 The AACN Guiding Principles for Academic-Practice Partnerships emphasize that sustainable models rely on a blend of direct financial contributions and in-kind resources from both sides.
- Personnel sharing: Protected staff time for precepting, shared coordinator roles across institutions.
- Facilities and access: Hospital-provided simulation lab space, electronic health record training environments, and meeting rooms.
- Leadership participation: Health system leaders serving on advisory boards, curriculum committees, or as guest lecturers, costing little in dollars but yielding high educational value.
Direct Financial Contributions and Scholarship Support
Some partners make targeted contributions that directly support program viability. For example, in June 2026, McLeod Health committed $75,000 to Francis Marion University’s nursing programs.1 This ongoing partnership specifically helps sustain the university’s Nurse Educator track, a direct investment in the faculty pipeline that eases the nursing faculty shortage. These kinds of contributions can be structured as annual gifts, scholarship endowments, or multi-year grants that reduce financial pressure on the school while signaling a health system’s long-term commitment.
Grants, In-Kind Support, and Preceptor Incentives
External funding sources can de-risk the early stages of a partnership. HRSA grants, state nursing workforce initiatives, and foundation awards frequently cover start-up costs, curriculum design, pilot programs, and rigorous evaluation.4 Hospitals supplement this with in-kind support, everything from protected preceptor time and free parking for students to leadership hours spent on partnership governance. The AONL Nurse Leadership Workforce Compendium identifies salaried positions, hourly pay, and incentive pay as core budget items.3 Preceptor stipends, even modest ones, can improve retention of those teaching at the bedside and are often a small line item with outsized impact.
- Student nurse apprentice programs: Combine hourly wages with partial tuition support, creating a funded pipeline that lets students earn while they learn.5
- Joint residency programs: A 30-position, 6-month nurse residency financed jointly by an academic and practice partner can reduce first-year turnover and pay for itself through lower recruitment costs.
Building the Business Case for Long-Term Investment
Securing sustained funding requires moving the conversation from “What does this cost?” to “What does it save, and what does it produce?” The business case should connect partnership investment to concrete outcomes: reduced vacancy rates among new graduates hired from partner schools, shorter orientation periods because students are trained in the system’s protocols, and avoided contract labor expenses. When a hospital sees that each dollar invested in a shared preceptor role translates into three to five new hires who stay beyond two years, the partnership becomes a workforce strategy, not a charitable donation. Frame the ask around shared risk and shared reward: both parties benefit from a well-prepared, locally grown nursing workforce, and both should have skin in the game.
Despite the common focus on funding, communication gaps remain the most frequently cited barrier to clinical partnership success in nursing education literature. Proactively address role clarity and mutual expectations with preceptors and clinical sites to prevent misunderstandings that can unravel even well-funded collaborations.
Overcoming Common Challenges in Clinical Partnerships
Bridging the Rural-Urban Placement Gap
Rural nursing programs consistently face tighter clinical placement options: fewer hospitals, limited specialty units, and a smaller pool of available preceptors. Urban sites, by contrast, often compete among multiple schools for the same teaching units. These disparities can delay student progression and reduce exposure to diverse patient populations.
Creative solutions are closing that gap. Tele-simulation, one of the most adaptable innovative teaching strategies in nursing education, allows students to connect to remote clinical instructors and simulated patient scenarios from their home campus, reducing the travel burden that makes rural placements impractical. When paired with periodic in-person immersion days, tele-simulation helps rural sites train more students without overloading on-site staff. Some partnerships also use shared simulation labs: one hospital invests in high-fidelity manikins, while neighboring schools rotate through the space, spreading costs across partners. Financial contributions, such as McLeod Health's $75,000 commitment to Francis Marion University's nursing program, further expand clinical training opportunities in regions where hospital capacity is limited, directly creating slots for students who would otherwise be waitlisted.1
Navigating Regulatory Compliance Across State Lines
Multi-state partnerships multiply the regulatory complexity. Each state board of nursing sets its own requirements for student clinical experiences, preceptor qualifications, and faculty supervision ratios. When a program places students across state lines, it must satisfy the rules of both the sending and the host state.
The Nurse Licensure Compact (NLC) eases the burden for participating states. Under the compact, nurses holding a multistate license can function as preceptors without obtaining a separate license, and students may cross borders for rotations more smoothly. As of 2026, many states remain non-compact, however, meaning programs must secure individual state board approvals and track varying continuing education mandates for preceptors. Successful partnerships build a centralized compliance checklist, assign a designated liaison to monitor rule changes, and use standardized affiliation agreements that include clauses for jurisdiction and liability. Early engagement with state nursing boards during the planning phase prevents costly delays and protects program accreditation.
Scaling from Pilot to System-Wide Partnership
Launching a single-unit pilot builds proof of concept without over-committing resources. The key is to design the pilot with scalability in mind. Define measurable outcomes upfront: student competency scores, preceptor turnover, placement fill rates, and any cost offsets. After one or two semesters, present the data to health system leadership alongside a clear expansion roadmap.
Scaling involves moving from a handshake arrangement to formal memoranda of understanding that cover multiple facilities. One effective model is a tiered partnership: a core academic-practice steering committee governs the relationship, while site-specific coordinators handle daily logistics. This structure allows the partnership to absorb new clinical units, add simulation resources, and even expand into joint faculty appointments or shared research projects, fostering nurse-led research in education. Programs that grow this way report more stable placement pipelines and deeper investment from both sides, transforming a single pilot into a durable, system-wide commitment.