What you’ll learn in this article…
- High exam scores can mask a student silently in personal crisis.
- One missed clinical day can invalidate an entire rotation placement.
- FERPA protects crisis disclosures the moment faculty document them.
Two weeks from graduation, a nursing student posted to r/StudentNurse in 2026 describing a breakup that landed mid-exam season. The student had just scored 95% on an ATI predictor exam. Their partner, a medical student, disclosed weeks of emotional withdrawal at the worst possible moment. Peers online advised compartmentalization and channeling the pain into fuel. The student pressed forward.
That post captures something nursing educators encounter regularly but rarely discuss in formal faculty training: students absorbing significant personal crises quietly, performing well on the surface, and getting no structured support because nothing visible broke down. Generic institutional crisis protocols were not built for nursing education's specific constraints, including mandatory clinical hours, cohort-based progression, patient safety obligations, and licensure timelines that leave almost no room for disruption.
What follows covers how to recognize suppressed distress, respond with a nursing-specific protocol, extend appropriate academic accommodations, protect clinical safety, comply with FERPA and mandatory reporting rules, and build the peer support networks that catch students before a quiet crisis becomes a program-ending one.
Why Personal Crises Hit Nursing Students Differently
A single missed clinical day can invalidate an entire rotation placement. That is not a policy quirk unique to one program. It is a structural reality baked into how nursing education works, and it means that when a student's personal life falls apart, the academic consequences arrive faster and cut deeper than they would in almost any other degree program.
The Architecture of Nursing Education Leaves Little Room
Four structural features make nursing programs especially unforgiving during a personal crisis:
- Rigid clinical scheduling: Clinical placements are arranged months in advance with hospital partners. There is no "make it up next week." Miss a required clinical day and you may forfeit the placement entirely, with no guarantee of a replacement slot.
- Lock-step cohort progression: Nursing programs are not designed for detours. Fall behind, and the next available on-ramp is typically a full semester away. A student managing a family emergency in November may not be able to resume until the following fall.
- Pass/fail clinical evaluations: Written exams allow partial credit and recovery across a semester. clinical placement evaluations for nursing students often do not. A student who arrives emotionally overwhelmed on evaluation day carries no safety net of accumulated points.
- Emotional labor during patient care: Nursing students are expected to regulate their own distress and show up therapeutically present for patients, sometimes within hours of receiving devastating personal news. That demand is real and professional, but it is also an extraordinary ask of someone mid-crisis.
What Online Peer Communities Reveal
When nursing students face a personal crisis, many do not walk into a faculty office. They turn to each other, often anonymously. Posts in communities like r/StudentNurse show students two weeks from graduation, mid-breakup, asking peers how to get through back-to-back exams. The advice they receive focuses on compartmentalization: put the feelings in a box, use whatever emotional energy is available as fuel, survive until the finish line.
That kind of peer support is genuine and sometimes effective. But it also signals something faculty need to sit with. Students are developing their own crisis protocols in spaces educators cannot see, which means the distress is real, the coping is active, and the faculty are largely absent from the conversation. Nursing student mental health support resources only help when students feel safe enough to use them.
The Cohort Model: Pressure and Potential
The same cohort structure that makes crises so costly also creates something valuable. Nursing students move through a program together, often for two years or more. They know each other's schedules, stress levels, and clinical placements in ways that a history professor advising 200 students simply cannot replicate.
A history major who misses a lecture can catch up on notes. A nursing student who misses a clinical shift may lose a semester. But that same nursing student also has a cohort of peers who noticed they were quieter than usual last week. Faculty who deliberately cultivate that peer awareness, rather than leaving it to chance, are adding a meaningful layer to the safety net they cannot personally provide around the clock.
Recognizing a Student in Crisis: Signs Educators Often MISs
High academic performance can mask deep personal crisis, creating a dangerous blind spot for nursing educators. A student who continues to excel on exams may be silently unraveling, and relying on grades alone to gauge well-being misses the nuanced behavioral shifts that signal a need for intervention.
Why Academic Success Isn't a Reliable Indicator
The recent Reddit post by a nursing student who scored 95% on the ATI predictor exam while processing a devastating breakup illustrates this paradox. The student was emotionally shattered yet maintained near-perfect test performance. This compartmentalization is common in high-achieving programs: students often prioritize academic outcomes over self-care, believing they cannot afford to show vulnerability. As a result, an otherwise strong student may suddenly turn in a failing assignment or miss a deadline, but a single data point can be dismissed as an anomaly. More telling are sustained pattern changes, such as a drop in overall course engagement, frequent late submissions, or a sharp decline in the quality of written work. Teaching emotional intelligence to nursing students can help build the self-awareness that makes these warning signs more visible to faculty and peers alike.
Clinical-Specific Red Flags
The clinical environment often reveals what classroom performance conceals. Faculty and preceptors should note:
- Emotional flatness during patient interactions, where a typically warm student becomes detached or robotic.
- Difficulty focusing during medication administration, with repeated double-checks or near-misses that deviate from the student's baseline.
- Tearfulness in post-conference or after feedback, particularly if the student has historically been resilient.
- Preceptor reports of changed demeanor, such as irritability, withdrawal from team discussions, or unusual reluctance to take on new tasks.
These signs are not diagnostic but serve as early warnings. Importantly, students may continue to attend clinicals faithfully while skipping non-clinical sessions like simulation lab or lecture, a masking behavior that preserves clinical hours but hides the extent of their distress. A structured clinical placement evaluation for nursing students can give preceptors a consistent framework to flag these behavioral deviations early.
Creating Low-Barrier Check-Ins
Waiting for students to self-disclose is unreliable; many fear judgment or academic repercussions. Instead, embed brief, private check-ins into existing routines:
- Schedule a 5-minute one-on-one after clinical debrief to ask, "How are you managing everything outside of clinical?"
- Use an anonymous self-assessment form at midterm with a question like, "Is anything outside of school affecting your ability to learn?"
- Normalize the conversation by sharing that many students face personal crises and that seeking support is a sign of professionalism, not weakness.
These low-stakes opportunities can make the difference between early intervention and crisis escalation.
Questions to Ask Yourself
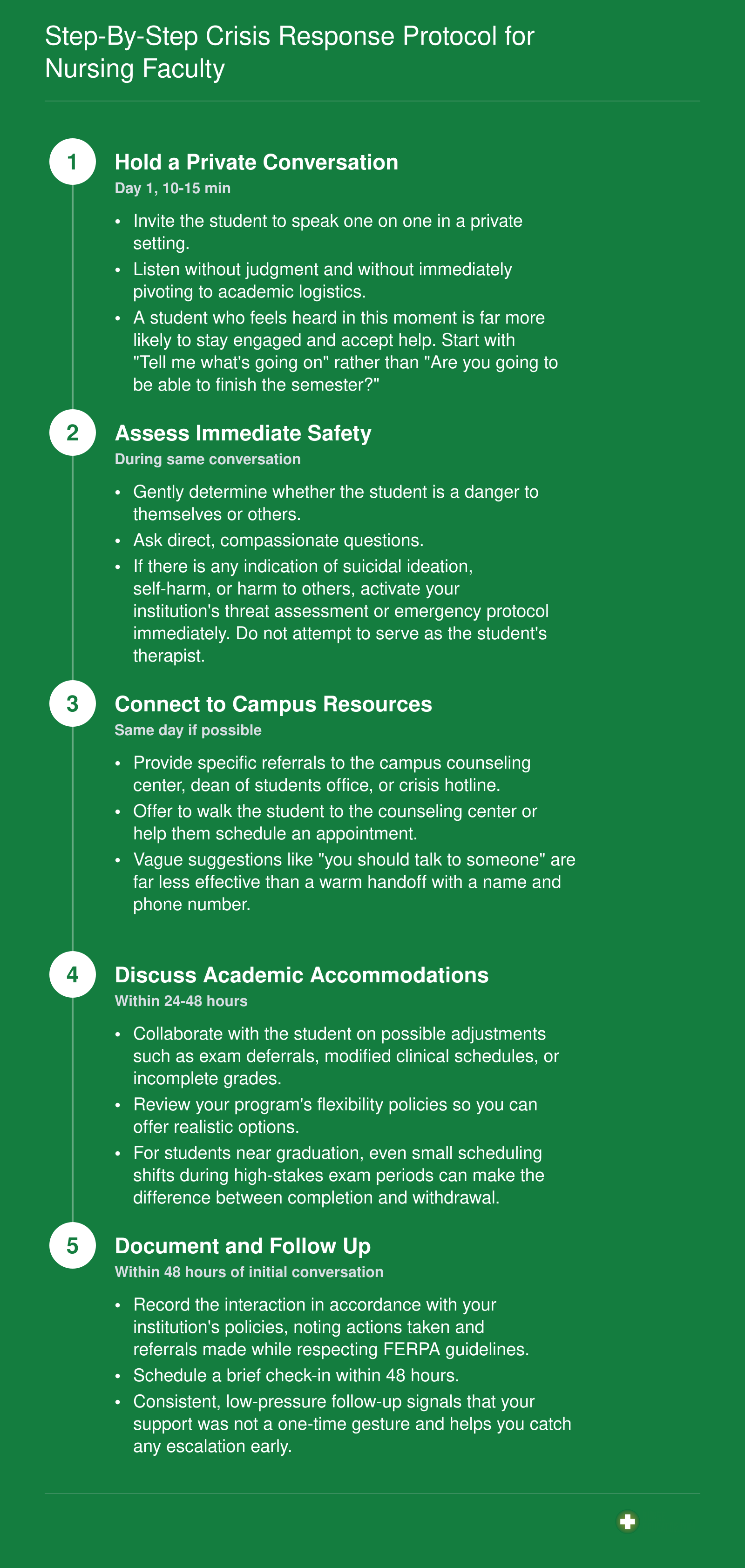
Step-By-Step Crisis Response Protocol for Nursing Faculty
Most nursing programs lack a structured, nursing-specific protocol for responding when a student discloses a personal crisis. Generic advice to "check on them" is not enough when clinical safety, patient outcomes, and licensure timelines are on the line. The sequence below gives you a repeatable framework you can adapt to your program. Remember: the first conversation sets the tone. Resist the urge to jump straight to "what about your clinicals?" before you have genuinely acknowledged the student's pain.
Academic Accommodations and Flexible Policies During Crises
Academic accommodations are formal adjustments to course requirements, timelines, or clinical schedules that allow students experiencing personal crises to continue their nursing education without sacrificing program integrity. These accommodations range from simple exam deferrals to extended leaves of absence, and understanding the full spectrum helps you guide students toward solutions that fit their specific situations.
Main Accommodation Categories
Nursing programs typically offer several accommodation pathways for students in crisis:
- Exam deferrals: Students can postpone high-stakes exams to a later date, usually within the same academic term. Approval typically requires a written request submitted through the disability services office and course director, along with supporting documentation when appropriate.1
- Incomplete grades: A temporary grade placeholder allows students to complete coursework after the semester ends, buying time without academic penalty.
- Clinical schedule adjustments: Students may shift to a later rotation group, change clinical sites, or work with different preceptors to accommodate personal circumstances.
- Formal leave of absence: Most programs allow one semester to one year away from studies with guaranteed cohort re-entry, though returning students typically must complete a skills competency check before resuming clinical work.2
What Accreditation Bodies Require
Neither AACN, NLN, nor CCNE prescribes uniform accommodation procedures, which gives individual programs significant flexibility in how they structure crisis support.3 However, all three organizations require that programs have clear student policies and provide reasonable accommodations. The Americans with Disabilities Act and Section 504 of the Rehabilitation Act also mandate reasonable accommodations, though any adjustment must preserve the essential functions of the nursing curriculum.4
Here is the critical tension you need to understand: accreditation bodies do not set minimum clinical hour thresholds, but state boards of nursing do.3 This means the total number of clinical hours is generally non-negotiable. What is adjustable includes the timing of those hours, the clinical site, and the assigned preceptor. Most programs also maintain 90 to 95 percent clinical attendance requirements that cannot be waived without board approval.5
Helping Students Navigate the Process
When a student is managing a breakup, family emergency, or mental health crisis, the last thing they need is to decode bureaucratic pathways alone. Rather than waiting for students to figure out accommodation options, you can proactively offer information during one-on-one check-ins or class announcements about available supports. Students dealing with accommodations for nursing students with mental health conditions often face overlapping challenges that a single referral cannot resolve.
AACN's Faculty Tool Kit on accommodating students with disabilities recommends that educators familiarize themselves with their institution's accommodation processes so they can serve as informed guides.5 NLN's guidelines on inclusion similarly emphasize faculty responsibility in connecting students to appropriate resources. When you know the process, you can walk a struggling student through each step: who to contact, what documentation helps, and realistic timelines for decisions.
Encourage students to submit written requests even when the situation feels informal. Documentation protects both the student and the program, creating a clear record of agreed-upon modifications. Most approvals flow through disability services and the course director together, so advising students to initiate contact with both parties simultaneously speeds resolution. For students at risk of leaving the program entirely, supporting nursing students at risk of dropping out offers additional retention strategies that complement accommodation planning.
Related Articles
Clinical Safety: When a Student's Crisis Affects Patient Care
Patient safety and student wellbeing sometimes pull in opposite directions, and faculty must navigate this tension without sacrificing either priority. A student experiencing a personal crisis may still be capable of safe clinical practice, or they may need a brief pause to protect themselves and their patients. The challenge lies in making that distinction fairly and consistently.
Fitness-for-Duty Assessment Framework
Not every sign of distress warrants removal from clinical settings. Students experiencing personal crises often demonstrate remarkable compartmentalization, continuing to perform safely even under emotional strain. Your assessment should focus on observable behaviors that directly affect patient care rather than assumptions about internal states. This focus on emotional intelligence for nurses can help faculty distinguish genuine impairment from temporary distress.
Behaviors that typically warrant a clinical pause include:
- Medication errors: Calculation mistakes, missed doses, or incorrect administration that occur in a pattern rather than as isolated incidents
- Assessment gaps: Inability to perform focused patient assessments, missing critical vital sign changes, or failing to recognize deterioration
- Emotional dysregulation: Visible distress during patient encounters, crying at the bedside, or inappropriate emotional responses that affect therapeutic communication
- Psychomotor impairment: Trembling hands during procedures, slowed response times, or difficulty with basic skills previously mastered
Behaviors that suggest a student can continue with monitoring include occasional tearfulness in private spaces, requesting brief breaks, quieter than usual demeanor, or needing additional clarification on tasks. These warrant check-ins and support rather than removal.
Communicating with Clinical Site Partners
When a student needs schedule modifications, preceptors need enough information to plan effectively without receiving details that violate the student's privacy. Frame conversations around logistics rather than circumstances.
Share only what the preceptor needs to know: the student will be absent for a specific timeframe, and you are coordinating makeup hours. Do not share diagnoses, personal circumstances, or details about the crisis. A simple statement works well: "This student needs to step back from clinical for a few days due to a personal matter. We will coordinate with you on rescheduling."
If preceptors press for details, redirect firmly: "I appreciate your concern, but I can only share what the student has authorized. What I can tell you is the timeline for their return."
Temporary Removal Protocol
The decision to remove a student from clinical belongs to the clinical coordinator or designated faculty member, not the bedside preceptor alone. This ensures consistency and protects both students and preceptors from ad hoc decisions made in high-pressure moments. Understanding the clinical nurse educator role clarifies why this decision authority matters and how faculty can exercise it constructively.
When implementing a clinical pause:
- Decision authority: The clinical coordinator evaluates the situation, consulting with the course lead if needed, before any removal occurs
- Student notification: Meet privately with the student, using supportive language that emphasizes this as a protective measure. Say "clinical pause" rather than "suspension" or "removal"
- Documentation: Record the decision, the observable behaviors that prompted it, and the plan for return. Avoid diagnostic language or speculation about causes
- Return pathway: Establish clear criteria for resuming clinical work, whether that involves a check-in meeting, documentation from a counselor, or simply the passage of a defined time period
- Makeup plan: Outline how missed hours will be recovered, ensuring the student knows this is logistically manageable and will not derail their progression
The language you use shapes how the student experiences this process. A clinical pause is a temporary protective measure, not a judgment on their capability or character.
A temporary pause from clinical rotations is an act of care, not a consequence. When you frame it as protection for both the student and the patient, students feel supported rather than punished. Students who fear disciplinary action will hide their crises, and that silence is what truly puts patient safety at risk.
Confidentiality, FERPA, and Mandatory Reporting: What Nursing Faculty Must Know
Every crisis disclosure a nursing student makes to you becomes part of their protected education record the moment you document it. Understanding exactly when you can share that information, when you must share it, and when sharing would violate federal law is not optional knowledge for nursing faculty. Getting this wrong exposes your institution to legal liability and, more importantly, can damage the trust students need to seek help in the first place.
The FERPA Baseline: What Stays Confidential
The Family Educational Rights and Privacy Act governs student education records at any postsecondary institution receiving U.S. Department of Education funds, which includes virtually all nursing programs.1 Under FERPA, when a student tells you about a divorce, a death in the family, financial hardship, or mental health struggles, you cannot share those details with clinical preceptors, fellow students, or even the student's parents without written consent.
This confidentiality applies broadly. The fact that a clinical coordinator needs to know why a student missed rotation does not override FERPA. The fact that a student is 22 years old and their mother calls demanding information does not override FERPA. One narrow exception allows disclosure to parents if the student qualifies as a dependent under IRS rules, but you should verify this through your registrar rather than making assumptions.2
Within your institution, FERPA permits sharing with school officials who have a legitimate educational interest.3 This means you can consult with your program director, academic advisor, or student services coordinator when making decisions about a student's academic standing. However, this does not extend to casual conversation or sharing more information than necessary for the specific educational decision at hand.
The Health and Safety Emergency Exception
FERPA includes a critical exception that nursing faculty must understand clearly: you may disclose protected information without consent when you can articulate a significant threat to the health or safety of the student or others.4 This exception exists precisely for the crisis situations you are most likely to encounter.
If a student discloses an imminent plan for self-harm, you may notify campus security, counseling services, emergency medical services, or law enforcement. You may also contact parents in this circumstance. The key word is "articulable." You must be able to explain specifically why you believed the threat was significant and why disclosure was necessary.
When invoking this exception, federal guidance requires documenting the nature of the threat, why you determined disclosure was necessary, to whom you disclosed information, and what specific information you shared.4 This documentation protects both you and your institution while demonstrating that you acted reasonably under the circumstances.
In nursing clinical settings, this exception becomes particularly relevant. If a student's crisis creates an immediate safety concern for patients, you have legal grounds to inform clinical site personnel of the specific safety issue without disclosing the underlying personal details. You might tell a preceptor that a student needs to be removed from patient care today without explaining that the student disclosed suicidal thoughts that morning.
Mandatory Reporting: When State Law Overrides FERPA
FERPA explicitly permits disclosure when required by state law, and nursing faculty face several mandatory reporting obligations that vary by jurisdiction.2 These typically include:
- Child abuse: If a student discloses witnessing or experiencing child abuse, you must report to child protective services or law enforcement per your state's requirements.3
- Vulnerable adult abuse: Similar obligations apply when students disclose abuse of elderly or disabled adults.
- Impaired practice: When a student's substance use or mental health condition creates an immediate risk in clinical settings, state nursing practice acts may require reporting to boards of nursing or designated monitoring programs.
When a student discloses substance use that is currently impairing their clinical performance, you should remove them from patient care immediately for safety reasons. You may notify program leadership and clinical site coordinators using the health and safety emergency exception. Depending on your state, you may also have obligations to report to impaired-practitioner programs.
FERPA vs. HIPAA: A Common Source of Confusion
Nursing faculty frequently confuse FERPA and HIPAA because they work in both educational and healthcare environments. The distinction is straightforward but essential: HIPAA governs the protected health information of patients at your clinical sites, while FERPA governs your students' education records.5 accommodations for nursing students with mental health conditions often surface this confusion, because faculty who handle both domains assume the frameworks overlap more than they do.
When a student tells you about their own depression diagnosis, that information falls under FERPA as part of their education record. When that same student accesses a patient's medical record at clinical, HIPAA governs that patient's information. Confusing these frameworks leads to either over-disclosure (sharing student information inappropriately because "we're all healthcare people") or under-disclosure (failing to report genuine safety threats because of misplaced HIPAA concerns).
Know which law applies to the specific situation you are facing, and when uncertain, consult your institution's legal counsel or student affairs office before making disclosure decisions.
Culturally Responsive Crisis Support for Diverse Nursing Cohorts
Understanding Cultural Differences in Crisis Perception
Nursing students bring diverse cultural frameworks that shape how they perceive, disclose, and cope with personal crises. For some, counseling carries a strong stigma and seeking professional mental health support may be seen as a sign of weakness or family failure. Other students prioritize immediate family or faith community guidance over institutional resources. Recognizing these differences is the first step toward providing truly inclusive support.
First-generation and immigrant students often shoulder additional burdens that peers may not face, such as financial pressures tied to family obligations, immigration-related stressors, or language barriers that complicate disclosure. A student struggling with a breakup, for example, may also be navigating acculturation stress or serving as a primary translator for their family, layering crisis upon crisis. Helping nursing students cope with financial stress is one concrete place to start for educators who want to address these compounding pressures.
Actionable Strategies for Inclusive Support
To meet students where they are, nurse educators can expand their crisis response toolkit beyond a one-size-fits-all counseling referral. Consider these actionable strategies:
- Offer multiple resource pathways: Provide options that include peer support networks, community-based faith leaders, and culturally specific organizations, in addition to campus counseling. Let students choose what feels safe.
- Ask, don't assume: When a student discloses a crisis, ask "What does support look like for you right now?" rather than immediately prescribing a solution. This respects cultural autonomy and opens a collaborative dialogue.
- Facilitate culturally concordant connections: Where possible, help students connect with mentors, advisors, or faculty who share similar cultural or linguistic backgrounds. Representation reduces isolation and builds trust.
- Address hidden crisis layers: Proactively check in with first-generation and immigrant students about financial, housing, or immigration stressors. Offer flexibility with deadlines or clinical hours when these compound personal crises.
Addressing Language and Communication Barriers
Language barriers can prevent students from fully describing their crisis or understanding available resources. Teaching ESL nursing students effectively requires many of the same sensitivity skills that crisis support demands, and educators experienced in one area will find those skills transfer directly. Key program documents, including crisis protocols, counseling brochures, and academic accommodation forms, should be available in the primary languages spoken within your cohort. When a crisis conversation involves complex emotional or academic details, offer professional interpreters or bilingual staff to ensure clarity and preserve dignity. Even when students are proficient in English, distress can limit vocabulary, so patience and visual aids (like flowcharts of options) can bridge the gap.
Building Peer Support Networks Within Nursing Cohorts
One of the most telling details in the Reddit post from r/StudentNurse was not the student's 95% ATI predictor score, but the speed with which fellow students rallied around them with practical coping advice. Commenters offered targeted strategies: compartmentalize relationship stress until after exams, channel frustration into focused study, and lean on the momentum you have already built. That kind of responsive, peer-to-peer support can be the difference between a student who persists and one who quietly withdraws.
As an educator, you may not always be the first person a struggling student turns to. Peers often are. This means intentionally building cohort-level support structures is not optional; it is a core part of your retention strategy. Cohorts that communicate regularly, study together, and check in on one another create an informal safety net that catches students before they reach a formal crisis point.
Here are practical steps for fostering that network:
- Create structured small-group study teams early in the program and keep them consistent throughout, so students develop genuine familiarity and trust before high-stakes periods arrive.
- Build brief, low-stakes check-ins into clinical post-conference or classroom time. A simple "how is everyone managing this week" normalizes the idea that stress is shared and discussable.
- Introduce students to peer mentoring resources or upper-cohort volunteers who can speak honestly about surviving the final stretch of the program.
- Use group communication platforms your students already prefer, and encourage faculty-approved channels where students can share study resources and encouragement without faculty surveillance dampening candor.
- Acknowledge publicly, when appropriate, that personal life does not pause for nursing school, and that reaching out to a classmate is a sign of self-awareness, not weakness.
Educators who actively model nursing student stigma reduction strategies make it easier for students to admit they are struggling before the situation escalates. When a cohort has been taught that vulnerability is acceptable, peer support activates faster and more effectively.
The student in that Reddit thread succeeded in part because their community responded immediately with empathy and direction. Your role is to build the conditions where that kind of community already exists long before a student needs it most. A well-connected cohort does not just improve morale; it directly supports nursing student retention strategies and completion rates across the board.
Mental Health Resources and Crisis Hotlines for Nursing Students
Most nursing students in crisis do not reach out because they do not know where to turn. They may assume support is unavailable at 2 a.m. before an NCLEX predictor exam, or that asking for help signals weakness to faculty. The reality is that a robust network of resources exists specifically for students in health sciences, and a significant number of students will never encounter those resources unless an educator puts them directly in front of them.1 Distribute this list at orientation, post it in your learning management system, and revisit it at the midpoint of each semester, especially before high-stakes exam blocks.
Immediate Crisis Support
- 988 Suicide and Crisis Lifeline: Call, text, or chat 988, available around the clock.2 Best for students experiencing suicidal thoughts, self-harm urges, or acute emotional crisis. Free and confidential.
- Crisis Text Line: Text HOME to 741741, available 24/7.1 Best for students who are not in a position to speak aloud, such as those in shared dorms or clinical housing, and who prefer a text-based format.
- NAMI HelpLine: Available by phone, text, and webchat. This is not a crisis line but an information and referral service. Best for students who need non-emergency guidance or help locating local mental health providers.
Nursing-Specific and Peer Support
- Nurse2Nurse Peer Support: A peer support hotline accessible through your state nurses association or a local ANA chapter.1 Best for students and new nurses navigating burnout, moral distress, or second-victim experiences after difficult clinical events.
- ANA Healthy Nurse, Healthy Nation: A free wellness program open to both ANA members and non-members, including nursing students. Students can register through the ANA website. Best for preventive wellness, stress management, and building long-term resilience habits before a crisis develops.
Campus and Clinical Site Options
- Campus Counseling Centers: Most accredited nursing programs are affiliated with a college or university that offers short-term counseling at no direct cost to enrolled students. Encourage students to identify their campus counseling contact during the first week of the program, not after a problem arises.
- TELUS Health Student Support (My SSP): A mental health app available at participating institutions.1 Students log in with school credentials and can access counselors around the clock. Best for health sciences students whose schools have adopted the platform.
- Hospital and Health-System Employee Assistance Programs: Many clinical placement sites extend their employee assistance programs to nursing students on rotation. Students can typically find the EAP contact number on their clinical site's intranet or on the back of their facility badge. Best for students dealing with distressing clinical experiences and who need confidential support quickly.
A Note on Proactive Distribution
Research on student help-seeking behavior consistently shows that awareness is a primary barrier. When students are overwhelmed, they do not search for resources. Faculty who embed this list in syllabi, post it in clinical handbooks, and mention it verbally before exam season remove that barrier at the moment it matters most. Fostering nursing student stress management habits early, and pairing that effort with a laminated card on a faculty office door or a pinned post in a course discussion board, costs nothing and may be exactly what a struggling student needs to take the first step.
Common Questions About Supporting Nursing Students in Crisis
These are the questions nursing educators ask most often when a student shares a personal crisis. Each answer is grounded in current best practices for nursing education and aims to give you a clear, actionable starting point. When in doubt, always consult your institution's student affairs office or legal counsel for guidance specific to your program.
As a nursing educator, you face a choice: wait for a student to hit a breaking point and ask for help, or act as the first line of support before a crisis disrupts their entire trajectory. Nursing programs often rely on formal counseling referrals, but the reality is that faculty are the first adults to notice when a student is struggling. High-achieving students can silently compartmentalize devastating personal events, and a single missed clinical day can derail a semester. Your three most critical actions are recognizing subtle signs early, following a clear protocol, and connecting students to resources. Nursing student retention strategies depend on exactly this kind of proactive educator presence. This week, review your program's crisis policies and identify one gap to address.