What you’ll learn in this article…
- Academic nurse educators typically work 40 to 55 hours per week during active semesters, while clinical educators average closer to 40.
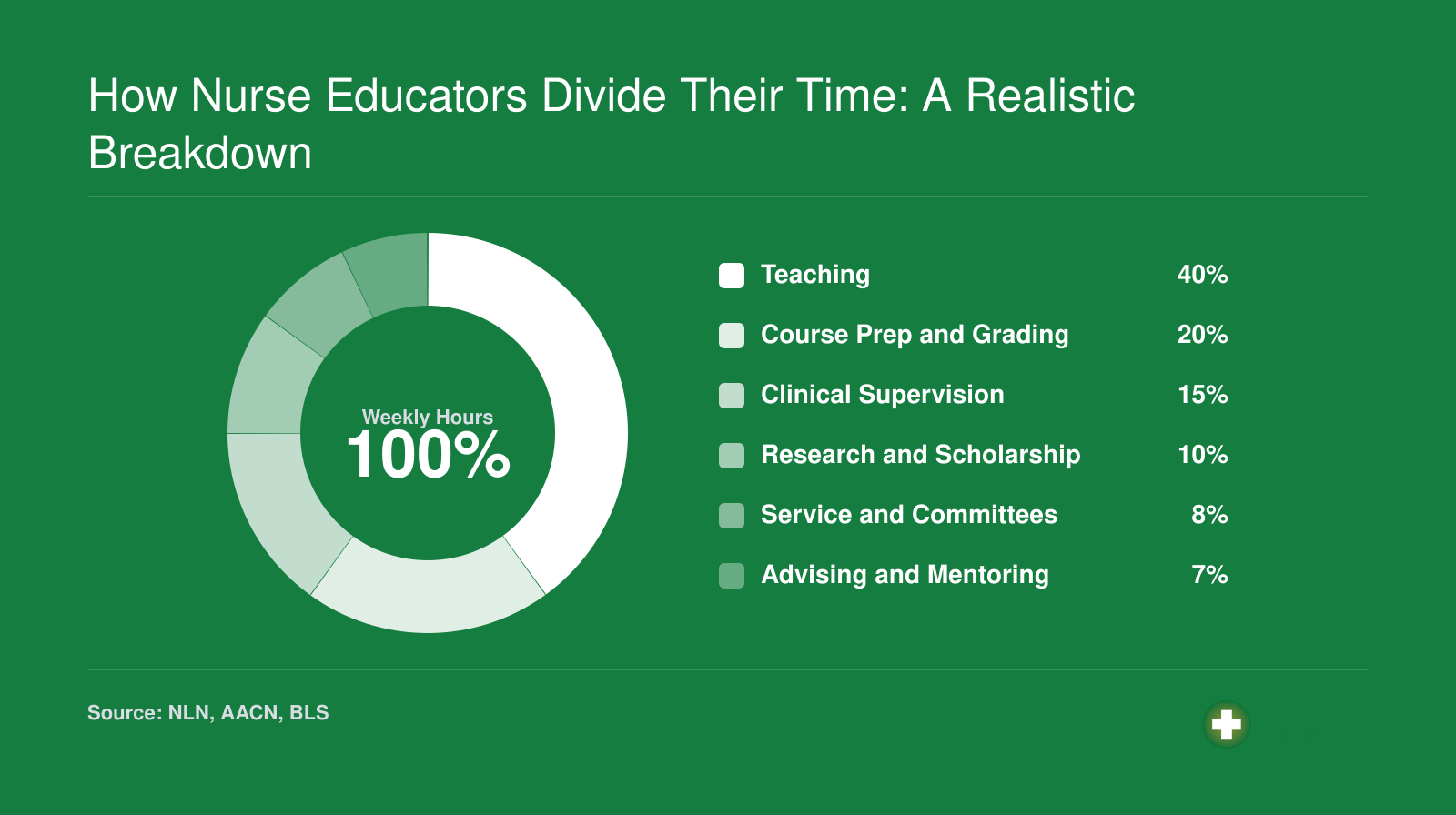
- Teaching accounts for roughly 40 to 50 percent of a university nurse educator's time, with scholarship and service filling the rest.
- DNP and PhD holders spend more daily hours on research or practice projects compared to MSN-prepared educators.
- Hospital-based clinical nurse educators follow shifting daily priorities driven by patient needs rather than a fixed class schedule.
A nurse educator's day varies sharply by setting, degree level, and whether the semester is in full swing or on break. An assistant professor at a university might spend Monday morning in a simulation lab coaching 18 students through a code scenario, then shift to grading case studies and drafting an IRB proposal in the afternoon. A clinical nurse educator at a 400-bed hospital typically starts the day rounding with new hires, troubleshoots a medication error during lunch, and wraps up by updating competency checklists and prepping a skills session on central-line maintenance.
Both roles center on teaching, but the academic track adds layers of scholarship, curriculum design, and committee service that hospital-based educators rarely face. Clinical educators work within operational hospital schedules, policy cycles, and regulatory audits, while academic faculty navigate semester calendars, accreditation reviews, and institutional research expectations. If you are still sorting out which path fits, understanding the difference between a nurse and a nurse educator is a useful starting point.
The sharpest dividing lines appear in time allocation and schedule flexibility. Academic educators log 40 to 55 hours per week during active terms, with summers often reserved for grant writing or course redesign. Clinical educators typically work closer to 40 hours but carry on-call duties, weekend rotations, and rapid-response obligations that blur personal and professional time.
Sample Day: Academic Nurse Educator (university Setting)
A lecture day and a clinical lab day pull an academic nurse educator in opposite directions. The core of the role blends classroom teaching, curriculum design, student mentorship, and scholarly work, but no two days look the same.1 For an MSN-prepared faculty member during a regular semester, the typical weekday stretches from early morning until evening, with a campus presence roughly 7:00 a.m. to 4:30 p.m. followed by hours of after-hours work.
The Rhythm of a Lecture Day
A didactic teaching day centers on a three-hour class block, often scheduled between 9:00 a.m. and noon. The schedule below reflects a common Tuesday or Thursday at a university school of nursing.
- 7:00 a.m. Arrive on campus, settle into the office, and review the day's lecture slides. Check the learning management system for overnight student messages or assignment submissions.
- 7:30 a.m. Finalize any last-minute clinical coordination emails or respond to a preceptor's question about a student's placement.
- 8:00 a.m. Quick walk through the simulation lab to confirm equipment set-up for an upcoming clinical lab session later in the week.
- 9:00 a.m. to 12:00 p.m. Three-hour didactic class for an undergraduate nursing course, such as Adult Health II or Pathopharmacology. The block often moves between brief lecture segments, case study discussions, and small-group problem-solving, keeping 40-plus students engaged requires more than straight PowerPoint.
- 12:00 to 1:00 p.m. Open office hours in the faculty suite. Students drop in with questions about the morning's content, upcoming exams, or clinical paperwork.
- 1:00 p.m. Lunch at the desk while scanning department announcements and accreditation updates.
- 2:00 to 3:30 p.m. Weekly curriculum committee meeting. Today's agenda: revising the pediatric simulation scenarios to align with new AACN Essentials.
- 3:30 to 4:30 p.m. Grading care plans or discussion board posts. Update the LMS with next week's readings and a recorded mini-lecture on EKG interpretation. Leave campus by 4:30 p.m.
Full-time faculty typically manage three courses per semester.1 A single course might combine a didactic section of 40 students with multiple clinical groups of eight to ten students rotating through hospital units. If you are still weighing the differences between these two teaching tracks, a closer look at the academic vs clinical nurse educator comparison can help clarify each path.
A Day in the Clinical Setting
Clinical teaching days follow a completely different clock.2 Instead of a lecture hall, the morning starts at a hospital nurses' station or simulation lab. The educator arrives by 6:30 a.m. for a 7:00 a.m. clinical start, meets eight to ten students, and reviews patient assignments. For the next four to six hours, the instructor rotates among students, verifying assessments, coaching medication administration, and leading bedside mini-teachings. A post-conference huddle at 1:00 p.m. ties the clinical experiences back to course concepts. These days leave little room for committee work or office hours; grading and prep shift entirely to evening blocks.
After Hours: Grading and Graduate Study
Evenings are rarely truly off. Most academic nurse educators log another two to three hours at home responding to student emails, entering clinical evaluations, or updating online modules. Many MSN-prepared faculty are also completing a DNP or PhD, carving out dedicated study time (often from 7:30 to 10:30 p.m.) to read research articles, draft dissertation chapters, or attend online seminars. For those exploring doctoral options, affordable nurse educator DNP programs can ease the financial burden. The workload easily exceeds forty hours a week, but the structure flexes: a heavy lecture day might mean fewer evening tasks, while a clinical day often spills grading into Saturday morning.
Sample Day: Clinical Nurse Educator (hospital Setting)
A hospital-based clinical nurse educator spends most of the day on the move, responding to the real-time demands of a live clinical environment rather than following a fixed classroom schedule.1
The Morning: Setting the Stage
7:00 AM - The day starts at the nursing station, not a desk. Most clinical educators begin with a quick check-in with charge nurses on each unit to identify education needs that have surfaced overnight. Did a new piece of equipment arrive? Is there a cluster of near-miss incidents that need addressing? That first conversation often shapes the rest of the day.
7:30 AM - New-hire orientation cohort session. If a group of nurses started the week, the clinical educator may lead a 30- to 60-minute skills lab or policy walkthrough before those nurses begin supervised floor time.
8:30 AM - Unit rounding begins. The clinical nurse educator role comes to life here as the educator moves from bed to floor, observing practices, validating competencies using standardized checklists, and fielding questions from staff. This is the core of the position: direct, bedside mentoring that an academic educator rarely provides.
Midday: In-Services and Documentation
10:00 AM - A 15- to 30-minute in-service session on an updated evidence-based protocol, perhaps a revised sepsis bundle or a new IV therapy guideline.1 Staff rotate through during breaks, so the educator may run the same short session two or three times across different units.
11:30 AM - Documentation catch-up. Competency completions, attendance records, and training logs get entered into the learning management system. Regulatory surveys and Joint Commission reviews depend on this data being current and accurate.
12:00 PM - Lunch, often interrupted. Staffing emergencies, a critical event on one of the floors, or a manager requesting an urgent debrief can pull the educator away mid-meal. This kind of interruption is routine, not the exception.
Afternoon: Project Work and Coordination
1:00 PM - Project-based work: updating a competency module, coordinating an upcoming certification prep course (BLS, ACLS, specialty certs), or reviewing staff compliance dashboards.
2:00 PM - Post-incident debrief or follow-up coaching with a nurse who struggled during a skills validation earlier in the day. These conversations are low-key but high-impact.
3:00 PM - Final check-in with nurse managers, flagging staff who need follow-up education and confirming tomorrow's scheduled in-services.
3:30 PM - End of shift, though clinical educators on project deadlines or during regulatory prep periods often stay later.
How This Differs from the Academic Side
Unlike academic educators, clinical educators rarely grade papers or sit on curriculum committees. The trade-off is a schedule far more subject to the rhythm of patient census, staffing gaps, and system-wide rollouts. Covering two or three specialty units in a single day is common, and no two days look exactly alike. If you are weighing whether bedside teaching or classroom instruction fits you better, understanding careers in nurse education can help clarify the decision. The work is immediate and visible: a nurse validates a skill correctly, a protocol gets adopted, a new hire gains confidence. The feedback loop is short and satisfying in ways that semester-long course outcomes simply are not.
How Nurse Educators Divide Their Time: A Realistic Breakdown
No two weeks look identical, but published surveys and faculty workload policies reveal consistent patterns in how nurse educators allocate their professional hours. The percentages below reflect a composite picture drawn from national nursing education workforce data. For the most current breakdowns, review reports from the National League for Nursing (NLN Faculty Census), the American Association of Colleges of Nursing (AACN Faculty Vacancy Survey and Annual Report on Nursing Faculty Salaries), and the Bureau of Labor Statistics occupation profile for postsecondary nursing instructors. You can also search for specific university nursing faculty workload policies online, which often spell out expected splits across teaching, scholarship, and service.
How the Workday Changes Across the Academic Calendar
Academic nurse educators experience roughly 30 to 35 weeks of intensive teaching each year, with the remaining time split between summer sessions, intersession breaks, and designated research or development periods. This rhythm shapes daily responsibilities in ways that clinical settings rarely replicate.
Fall and Spring Semesters: Teaching at Full Intensity
During active semesters, classroom and clinical instruction dominate the schedule. A typical week might include 9 to 12 hours of direct teaching, plus student advising, exam creation, grading, and committee meetings. Office hours expand, clinical site coordination intensifies, and simulation lab time increases as students progress through skills checkoffs. Many faculty describe these months as a sprint, with evenings and weekends often absorbed by grading or student concerns.
Summer Sessions: Development, Not Vacation
Myths about nurse educators abound, and the idea that academic educators enjoy summers off is one of the most persistent. Most faculty use these months for curriculum revision, course redesign, and accreditation documentation. Grant writing peaks during summer when uninterrupted focus is possible. Conference attendance clusters here as well, with national meetings from organizations like the National League for Nursing or Sigma often scheduled in June or July. Some faculty teach condensed summer courses or pick up adjunct clinical shifts to maintain patient care competencies. Others complete continuing education requirements or pursue certification renewal, including the CNE vs CNEcl decision, which requires ongoing professional development.
Clinical Nurse Educators: A Steadier Rhythm
Hospital-based clinical nurse educators experience less dramatic seasonal swings, but predictable peaks still occur. New graduate nurse orientation programs typically launch in summer and early fall, creating intensive onboarding cycles. Annual competency assessments, skills fairs, and mandatory training renewals cluster at fiscal year boundaries, often January or July. During these periods, daily schedules shift toward group instruction, skills validation, and documentation review. Outside these peaks, the workday remains more consistent, focused on unit-level education, policy rollouts, and precepting support.
Breaks and Continuing Education
Winter and spring breaks offer academic faculty opportunities to catch up on scholarly projects, complete clinical practice hours, or simply recover from the semester's pace. Many programs encourage or require faculty to maintain some level of clinical involvement, whether through per diem shifts or simulation work, to ensure teaching remains grounded in current practice standards. If you are weighing whether nurse educators work with patients during these periods, the answer often depends on the program's expectations and each educator's personal goals.
Questions to Ask Yourself
Online and Hybrid Teaching: What's Different for Nurse Educators?
Online and hybrid formats have moved from contingency measures to permanent fixtures in nursing education, reshaping what a typical workday looks and feels like at a structural level.
A Different Kind of Morning Routine
For online and hybrid educators, the day rarely starts in a classroom. It starts with the learning management system. Most nursing programs now run on Canvas, Blackboard, Moodle, or D2L/Brightspace, and checking in on those platforms is often the first task of the morning.1 Educators scan for new student messages, review overnight discussion board posts, and check which students have completed assigned virtual simulation modules in tools like vSim, Shadow Health, or i-Human. Virtual simulation adoption across nursing programs reached 87% by 2020, a 24-percentage-point jump from 2016.1
Those simulation platforms matter more than they might appear to. Students complete clinical reasoning scenarios independently, and the educator's job shifts from real-time supervision to reviewing performance data after the fact. That means analyzing decision pathways, identifying where students struggled, and writing individualized feedback, all asynchronous, all time-intensive.
Afternoons: Where Synchronous Work Lives
Synchronous activity tends to cluster in the afternoon: live class sessions via videoconference, virtual office hours, and simulation debriefings where educators walk through case outcomes with students in real time.1 These blocks feel closer to traditional teaching, but the prep work behind them is heavier. Lecture videos require recording, editing, and uploading before the week begins. Modules need updating whenever content changes. Educators who want to sharpen these skills can explore innovative teaching strategies in nursing education that translate well to virtual formats.
The Flexible-but-Longer Hours Reality
A common misread of online teaching is that flexibility equals reduced hours. Post-pandemic research on nursing faculty tells a different story: online workloads run equal to or higher than in-person loads, largely because the LMS is always accessible.2 Educators report checking messages and grading across evenings and weekends far more often than their in-person counterparts. The boundaries that a physical campus once enforced simply disappear. If you are weighing the schedule trade-offs, our guide to the benefits of online nurse educator program options offers a fuller picture.
Hybrid Models: Two Worlds in One Schedule
Hybrid programs create a split-format workday that is genuinely distinct. An educator might spend Tuesday morning supervising students in a hospital clinical rotation and Tuesday afternoon recording a pharmacology lecture module for asynchronous delivery. The in-person clinical supervision does not shrink; the online instructional load simply gets added alongside it. That combination rewards educators who are comfortable moving between high-presence clinical coaching and independent, self-directed content production, but it also means the workday rarely has a clean off-switch.
MSN Vs. Dnp/phd: How Education Level Shapes Daily Responsibilities
Your terminal degree does not just open different doors; it reshapes what you do once you walk through them. An MSN, a DNP, and a PhD each channel a nurse educator's daily energy toward distinct priorities, and understanding those differences helps you choose a path that fits the career you actually want.
MSN-Prepared Educators: Teaching at the Core
Most MSN-prepared nurse educators spend the bulk of their workday in direct teaching and clinical supervision.1 A typical morning might involve lecturing in a fundamentals or med-surg course, while the afternoon is spent on a clinical unit precepting students through patient assessments. Research expectations are modest, usually limited to curriculum development or small-scale scholarly projects.2 Many community colleges hire MSN-prepared faculty for full-time positions, though at four-year universities these roles are often non-tenure-track (clinical instructor, lecturer, or adjunct).2 If you love bedside teaching and want to stay close to hands-on patient care, the MSN route keeps your daily schedule anchored there.
DNP-Prepared Educators: Bridging Practice and Classroom
DNP-prepared educators add a translational layer to their workdays. Beyond lecturing and clinical oversight, they frequently lead evidence-based practice initiatives, quality-improvement projects, or practice-change pilots within affiliated health systems.1 Many hold dual clinical-academic appointments, splitting time between a university and a hospital or clinic. This practice credibility makes them especially effective mentors for advanced-practice students. Tenure eligibility varies by institution; some schools offer a dedicated practice track rather than a traditional tenure line.2 Daily tasks lean toward teaching, practice leadership, and translating research findings into clinical protocols.
PhD-Prepared Educators: Research Takes Center Stage
PhD-prepared faculty carry the heaviest scholarship expectations. On a given day, protected research time may consume several hours: writing grant proposals, analyzing study data, drafting manuscripts, or mentoring doctoral students through dissertations.2 Teaching loads are typically lighter than those of MSN colleagues precisely because publishing in peer-reviewed journals and securing external funding are core performance metrics. At research-intensive universities, a PhD is increasingly the baseline for a tenure-track appointment.2 Administrative and leadership roles, such as department chair or associate dean, also tend to favor doctoral-level faculty. If the PhD path appeals to you, exploring an affordable online nurse educator PhD can help you compare programs and costs.
Quick Comparison Across Key Dimensions
- Daily tasks: MSN educators center on teaching and clinical supervision; DNP educators blend teaching with practice-improvement work; PhD educators balance teaching with original research.
- Research expectations: Modest curriculum scholarship (MSN), practice translation and quality improvement (DNP), grant-funded original research and publication (PhD).
- Tenure eligibility: Often non-tenure-track (MSN), practice-track at select institutions (DNP), commonly tenure-track (PhD).
- Leadership roles: MSN faculty may lead course coordination; DNP faculty often direct clinical partnerships; PhD faculty frequently hold senior administrative positions.
- Clinical integration: MSN and DNP educators typically maintain active clinical roles, while PhD faculty may step away from direct patient care to prioritize scholarship.
The credential you pursue should align with how you want to spend your hours, not just the title on your badge. If direct teaching energizes you, an MSN can launch a fulfilling career. If you want to shape practice at a systems level while still teaching, a DNP fits. And if generating new nursing knowledge is the goal, a PhD positions you for a research-centered academic life. Understanding the full range of nurse educator job titles can also help you match your degree to the role that suits you best.
Related Articles
Work-Life Balance, Weekly Hours, and Common Stressors
Academic nurse educators typically log 40 to 55 hours per week during the active semester, while hospital-based clinical nurse educators tend to run closer to a standard 40-hour week, though many carry on-call duty, rotate through evening shifts, or flex their schedules to cover orientation cohorts and night-shift competency checks.
Is Nurse Educator a Stressful Job?
Yes, though the stressors look different from bedside nursing. The most commonly cited pressures in faculty workload discussions include:
- High student-to-faculty ratios: Clinical groups capped at 8 to 10 students still mean simultaneously supervising medication passes, charting, and patient assessments across an entire unit. The ongoing nursing faculty shortage only intensifies this pressure.
- Publish-or-perish pressure: Tenure-track faculty juggle teaching loads with manuscript deadlines, grant submissions, and committee service, often compressing scholarship into evenings and breaks.
- Emotional labor of clinical supervision: Coaching students through their first code, first patient death, or first medication error draws on the same reserves that contribute to bedside burnout. Building skills in teaching emotional intelligence to nursing students can help, but it takes real energy.
- Administrative burden: Accreditation self-studies, course mapping, learning management system maintenance, and competency documentation absorb hours that faculty often expected to spend teaching.
For context on the broader profession: national surveys of registered nurses in 2024 found burnout prevalence around 87%, with workload identified as the leading risk factor.1 RN job satisfaction slipped to 47% in 2026 from 55% the prior year, and 43% of bedside nurses reported intention to leave direct patient care.2 Whether educator-specific rates track that closely is not well established in the public data, so treat any direct comparison cautiously.
The Satisfaction Side of the Ledger
Despite the workload, nurse educators consistently report some of the highest career satisfaction in nursing. CareerExplorer's 2026 occupational rankings place nurse educators among the most satisfied healthcare roles, with respondents citing the impact of shaping the next generation of nurses, intellectual stimulation from curriculum design and scholarship, and meaningful schedule flexibility compared with 12-hour bedside shifts.
The Honest Caveat About Evenings and Weekends
The flexibility comes with a tradeoff worth naming directly. Grading clinical paperwork, responding to student emails, writing exam items, and reviewing care plans rarely fit cleanly into business hours. Most academic faculty describe a rhythm where Sunday evenings absorb the week's prep, and clinical educators often field texts from preceptors well outside their posted shift. The work is portable, which is both the benefit and the catch.
Nurse Educator Salary by Setting: Where You Work Shapes What You Earn
The table below compares national median salaries and percentile ranges for three occupations most relevant to nurse educators, drawn from the latest Bureau of Labor Statistics data. Keep in mind that hospital-based clinical nurse educators are typically classified under the Registered Nurses category in BLS reporting, not under postsecondary instructors. That means a clinical educator's pay often looks more like an RN salary than an academic faculty salary. Setting choice also affects compensation beyond base pay: hospital educators may receive shift differentials, overtime eligibility, and comprehensive benefits packages, while academic nurse educators may enjoy tuition waivers, sabbatical eligibility, and more flexible scheduling during summer and winter breaks.
| Occupation | National Employment | 25th Percentile | Median Salary | 75th Percentile | Mean Salary |
|---|---|---|---|---|---|
| Nursing Instructors and Teachers, Postsecondary | 74,250 | $62,210 | $79,940 | $102,020 | $87,090 |
| Registered Nurses | 3,282,010 | $78,610 | $93,600 | $107,960 | $98,430 |
| Nurse Practitioners | 307,390 | $109,940 | $129,210 | $149,570 | $132,000 |
The AACN notes that a national faculty shortage forces nursing schools to turn away thousands of qualified applicants annually. As a result, nurse educators often face heavier-than-ideal workloads, managing larger classes and additional committee responsibilities, which directly intensifies their daily schedules.
Frequently Asked Questions About Nurse Educator Work Days
These are the questions nurses ask most often when exploring educator roles. Each answer gives you the essentials; scroll up to the corresponding section of this article for a deeper look.