What you’ll learn in this article…
- Formal complaints require five documented steps from intake through appeal.
- Anti-retaliation policies must be enforced, not just published in handbooks.
- Anonymous feedback channels reduce complaints by catching issues early.
Most nursing programs do not publish a clear, step-by-step workflow for handling student complaints about clinical instructors, which leaves both students and faculty navigating an ambiguous, high-stakes process during emotionally charged moments. A January 2026 post in the r/StudentNurse subreddit captured this tension: a paramedic-turned-nursing-student, weeks from graduation in a $130,000 program, described an instructor who followed male students on Spotify during introductions, refused to take students to the ER because it wasn't "her thing," and dismissed some clinical days by 2:30 p.m. instead of the scheduled 12-hour shift.1 The student asked whether reporting was worth the risk of retaliation.
That question is the starting point for every nurse educator who fields a complaint: what happens next, who decides, and how do you protect both the student's right to speak and the instructor's right to due process? Complaint management sits at the intersection of accreditation standards, employment law, nursing student rights, and professional ethics, and the absence of a visible process often does more damage than the original complaint.
Why Students Complain About Clinical Instructors
Every complaint sits at a tension between two legitimate needs: the student's need for a fair, safe learning environment and the instructor's authority to evaluate performance in a high-stakes clinical setting. When those needs collide, the clinical floor amplifies the friction in ways the didactic classroom rarely does.
The Recurring Complaint Themes
A review of nursing education literature, including work published in Nurse Education Today and summarized through PubMed Central, points to a consistent cluster of grievances.3 Most complaints fall into one of five buckets:
- Perceived unfairness in evaluation: subjective grading, moving goalposts, or inconsistent expectations across the cohort.
- Unprofessional conduct: dismissive comments, public shaming, or gossip about other units and specialties.
- Inadequate clinical exposure: shortened shifts, restricted unit access, or refusal to rotate students through certain areas.
- Favoritism: preferential assignments, social media connections with select students, or uneven attention.
- Boundary violations: inappropriate personal disclosures, following students on personal accounts, or blurring social and evaluative roles.
How Common Is This, Really?
The scale is larger than most program directors want to admit. A national survey of 152 nursing students reported that 88% had experienced some form of incivility in their training,1 and 47% described the challenge as moderate or greater.2 Roughly 34% flagged instructor-to-student ratios as unsuitable for meaningful learning, and 66% reported restricted access to units they needed for a well-rounded rotation.2 "Inconsistent expectations" surfaced as the single most common theme, and students exposed to these conditions consistently reported lower satisfaction with their program overall.3
Clinical complaints tend to outpace didactic ones because the setting is uniquely high-stakes: instructors control patient assignments, sign off on competencies, and hold the pen on pass or fail decisions, all while students are visible to nursing staff, physicians, and patients.
Why Students Stay Silent
Underreporting is the norm, not the exception. Students weigh three fears before speaking up: grade retaliation from an instructor who controls their evaluation, cohort visibility in small clinical groups where anonymity is impossible, and a learned belief that "nothing will change" because prior complaints went nowhere. Understanding clinical incivility in nursing education is the first step toward addressing these systemic barriers. Compounding this, many clinical instructors are novice educators or adjuncts hired for their bedside expertise, not their pedagogy, and complaints cluster disproportionately around faculty who have never received formal training in teaching or feedback.
A Real-World Example: What One Student's Reddit Post Reveals
A nursing student with six years of experience as a paramedic, enrolled in an advanced medical-surgical clinical rotation and set to graduate in November, paid $130,000 for a 2.5-year program at a private university with NCLEX pass rates in the 90s. That student turned to Reddit instead of their school administration when their clinical instructor's behavior raised serious concerns.
The post by user Immediate-Quote-9407 in r/StudentNurse1 describes a cardiac ICU nurse in her final quarter of nurse practitioner school who made several decisions that, from an educator's perspective, represent failures in professional judgment, curriculum fidelity, and boundary management. The student's hesitation to report these issues, despite their gravity, underscores the power dynamics and retaliation fears that pervade clinical education.
When Instructor Preference Overrides Curriculum Objectives
The instructor told her group of eight students she would not take them to the emergency department because the ER "isn't her thing." For an advanced med-surg rotation in a critical care nursing course, this decision substitutes personal preference for learning outcomes. Students at this level need exposure to rapid assessment, triage decision-making, and high-acuity interventions that the ER uniquely provides. When faculty refuse entire clinical environments based on comfort rather than competency development, they limit the scope of practice students will enter upon licensure.
The same student had completed a pediatric clinical rotation at a daycare center rather than a hospital. These patterns suggest a program willing to accept convenience over rigor, even as it charges six figures in tuition. Building stronger clinical partnerships in nursing education can reduce the likelihood that instructors make placement decisions based on personal preference rather than curriculum requirements.
Clinical Hours as a Purchased Commodity
The instructor informed students they would leave some days by 2:30 p.m. instead of completing the scheduled 12-hour shifts (0700 to 1900). From the educator's lens, early dismissals represent lost clinical hours the student paid for and the state board of nursing counted toward licensure eligibility. At $130,000 for 2.5 years, each clinical hour carries a tangible cost. Shortening shifts without educational justification is not flexibility; it is a breach of the implicit contract between institution and student.
Professional Boundary Violations in Plain Sight
During introductions, the instructor followed a male student on Spotify. This act crosses professional boundaries in a teaching relationship. Clinical instructors hold evaluative power over student progression, and any behavior that suggests favoritism, personal interest, or social connection outside the educational context undermines the integrity of assessment and creates an environment where other students may perceive bias. These are exactly the situations that qualities of a good nurse educator frameworks are designed to prevent, by establishing clear expectations for professional conduct before faculty enter the clinical setting.
The instructor also remarked that obstetric nurses are "too happy" and their demeanor is off-putting. Such comments model disrespect for nursing specialties and reinforce stereotypes rather than fostering collegiality across the profession.
The Retaliation Calculus
The student ended their post with a question: should they report the instructor? The fear of retaliation is explicit. This hesitation is not unique. It is the norm in clinical education, where students depend on favorable evaluations to progress, secure recommendations, and graduate on time. The fact that a student with significant prehospital experience, paying top-tier tuition at a high-performing school, feels safer posting anonymously online than filing a complaint with their program director reveals a structural failure in how nursing education handles accountability.
This case is not an outlier. It is a window into what happens when institutions prioritize faculty convenience and pass rates over student advocacy and educational integrity. The remainder of this article will walk you through the complaint management workflow that should exist, the student rights that should be protected, and the cultural shifts required to move from retaliation fears to responsive, fair processes.
Questions to Ask Yourself
Feedback Vs. Formal Complaint: Knowing the Difference
Not every student concern rises to the level of a formal complaint, and understanding that distinction is one of the most practical skills a nurse educator can develop. When a student expresses dissatisfaction with a clinical experience, your first job is to assess what kind of response the situation actually calls for.
Routine feedback covers everyday frustrations that are real but resolvable through conversation. A student who feels a rotation moved too quickly, or who wished they had more hands-on time with a particular skill, is offering constructive input. That input belongs in a debrief, a one-on-one check-in, or a course evaluation. It does not require a paper trail or administrative escalation.
A formal complaint is different in both nature and stakes. It involves conduct that is repeated, targeted, or potentially harmful to the student's learning or well-being. Consider the scenario that surfaced in a widely discussed nursing student thread: a clinical instructor who refused to take students to the ER because it "isn't her thing," dismissed entire specialties based on personal opinion, and allowed clinical days to end hours before the scheduled 12-hour shift. Students in that group were paying $130,000 for a 2.5-year program and receiving pediatric rotations at a daycare center rather than a hospital setting. That is not a feedback situation. That is a pattern of conduct that directly undermines educational outcomes and warrants formal review.
As an educator, you also need to distinguish between complaints that reflect a student's personal discomfort and those that signal genuine misconduct. A student who dislikes being corrected publicly may be uncomfortable, but a student who describes consistent differential treatment across a clinical group is describing something more serious. clinical placement evaluation for nursing students gives programs a structured way to surface these patterns before they reach the complaint stage.
When a student comes to you unsure whether to report, help them ask three questions: Was the behavior isolated or repeated? Did it affect their learning or sense of safety? Would a reasonable peer in the same situation share their concern? If the answers point toward yes, guide them toward your institution's formal process without discouraging them or minimizing what they experienced.
Step-By-Step Complaint Management Workflow for Nurse Educators
A consistent, well-documented complaint process protects students, instructors, and your program's accreditation standing. The workflow below aligns with ACEN and CCNE accreditation expectations for due process, which require notice, an opportunity to respond, impartial review, access to evidence, and a written explanation of the outcome. Adapt timelines to your institution's policies, but treat these benchmarks as the floor, not the ceiling.
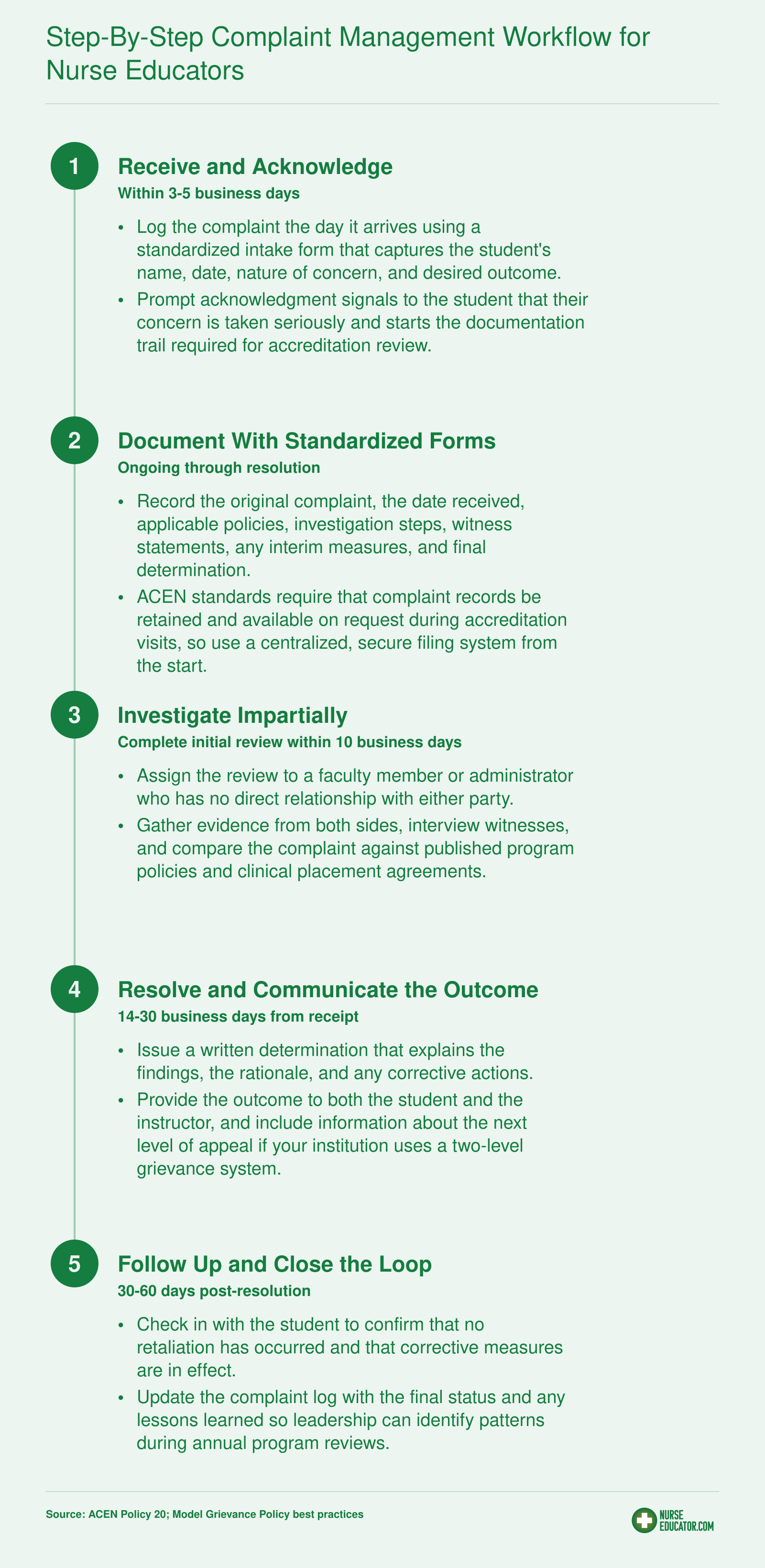
Inside the Workflow: What Each Step Looks Like in Practice
A workflow diagram is only as strong as the judgment behind each step. Here is how experienced nursing programs translate those five steps into daily practice.
Step 1: Routing the Complaint to the Right Person
Student complaints should not land on the desk of the accused instructor's direct supervisor if that can be avoided. When the supervisor also serves as the intake officer, students perceive (often correctly) that loyalty and reporting lines will color the review. Instead, route intake to a course coordinator, clinical placement director, or an assistant dean of student affairs who sits outside the accused faculty member's chain of command. That structural separation is what gives the process credibility, both to the student and to any external reviewer who later audits the file.
If your program is small and separation is impossible, name a designated alternate in writing before any complaint arises. Deciding who investigates after a complaint lands looks like scrambling, even when it isn't.
Step 2: What the Documentation Should Capture
A usable complaint record includes the date and location of each incident, the names of any witnesses, the specific behaviors observed (not conclusions like "unprofessional"), any prior attempts the student made to resolve the issue informally, and the student's desired outcome. Ask the student directly: do you want an apology, a change in clinical assignment, a formal reprimand, or simply a record on file? The answer shapes the entire investigation.
Keep the original student narrative intact. Summaries introduced later should be labeled as such.
Step 3: Investigating While Preserving Impartiality
Interview the student, the accused instructor, and any witnesses separately. Do not share the complainant's exact wording with the instructor in the first interview: describe the concerns in neutral terms and let the instructor respond. Review clinical schedules, attendance logs, and any written communications that corroborate or contradict either account. A nursing clinical placement quality assessment at the program level can surface patterns that individual complaints might not reveal on their own.
Step 4: Timelines That Signal the Process Is Real
ACEN does not prescribe a specific number of days for internal grievance handling1; instead, its Policy #20 requires that programs resolve student complaints in a timely manner and follow their own published procedures.2 Programs are also expected to keep a record of complaints available to ACEN on request.1 A defensible internal benchmark: acknowledge receipt within 48 hours, complete the investigation within 10 business days, and communicate the outcome within 5 business days of the decision. Publish those numbers in your student handbook so expectations are shared.
Step 5: Confidentiality on Both Sides
Protect the complainant's identity within the limits of due process, and protect the accused instructor from hallway speculation until findings are complete. Share information strictly on a need-to-know basis, and remind every participant in writing that discussing the case outside the process is itself a professionalism issue.
Protecting Students From Retaliation
Mount Carmel College of Nursing explicitly prohibits retaliation against any person who reports a crime, brings a disciplinary complaint, pursues legal action, or participates in an investigation.1 That bright-line policy reflects a national consensus: retaliation is one of the most corrosive forces in clinical education, and programs that fail to prevent it enable underreporting.
What Retaliation Looks Like
In clinical nursing education, retaliation is rarely as crude as a shouted threat. More often it appears as grade deflation after a complaint, sudden negative clinical evaluations that contradict earlier feedback, exclusion from valuable learning opportunities, hostile questioning designed to humiliate, or reassignment to undesirable shifts without educational rationale.2 These actions may fall into a gray area, but the effect is the same: students learn that speaking up carries a personal cost. When the fear of retaliation outweighs the perceived benefit of reporting, legitimate concerns go unaddressed.
Building Systemic Anti-Retaliation Safeguards
Effective programs put structural protections in place, not just promises.3 Concrete strategies include: - Anonymous reporting channels: Online portals that allow students to raise concerns without attaching their name, while still triggering a formal review. - Third-party evaluation during investigations: Assigning a neutral faculty member or clinical coordinator to assess the student's performance while a complaint is open, insulating the evaluation from bias. - Written no-retaliation pledges: Signed at the start of every clinical rotation by instructors and students alike, these pledges define prohibited behaviors and clarify that retaliation will result in disciplinary action. - Grade-freeze policies: Temporarily locking the student's evaluation status so that no grade changes can occur until the investigation concludes, removing the incentive to punish through grading. - Designated ombuds contact: A confidential, impartial resource who can guide students through the process, advocate for fair treatment, and monitor for signs of retaliation after a report.
The Legal Framework
On the federal level, Title IX prohibits retaliation against individuals who oppose discrimination, report gender-based harassment, or participate in an investigation.2 Title VI, Section 504, and the Age Discrimination Act create similar protections. FERPA does not itself create a standalone anti-retaliation right, but it requires that complaint-related records be kept confidential and shared only with those who have a legitimate educational interest, which can help limit exposure.2 State-level whistleblower statutes add another layer: Ohio Revised Code § 4723.33 protects nurses who report violations in good faith, Texas Health and Safety Code § 161.134 bars hospital retaliation against employees who report infractions, and Minnesota's expanded Patients' Bill of Rights safeguards residents from retaliation for advocacy.4
Why Fear Persists
Return to the Reddit case. The student's highest barrier was not proving unprofessional conduct, it was the dread of academic payback. When an instructor holds power over grades and clinical placements, a complaint can feel like a gamble. Programs that do not address that power imbalance structurally are, in effect, complicit. The connection between unchecked instructor authority and faculty incivility in nursing education is well documented, and it reinforces why structural safeguards matter more than written policy alone. Mandating annual training for faculty on anti-retaliation obligations,5 monitoring grading patterns for complainants versus non-complainants, and publicly affirming that interim measures (like moving a student to another clinical group) will be non-punitive can shift the culture. Until students believe that reporting is safe, even the best-written policy remains theory.
A complaint process is only as strong as its anti-retaliation protections. If students believe reporting will cost them their grade or their seat in the program, the process exists on paper only.
Student Rights in Clinical Rotations
As of 2024, nursing programs are required to uphold fair testing obligations, which extend directly to clinical evaluations.1 That mandate, reinforced by the National League for Nursing, sets a baseline for what students should expect during hands-on training. When those expectations aren't met and a complaint arises, knowing the rights students already hold makes the process clearer for everyone.
Core Rights in Clinical Education
Every nursing student enters a clinical rotation with certain fundamental protections. The National League for Nursing's vision statements and state board endorsements, including Minnesota's 2024 endorsement of the Fair Testing Imperative,2 outline a consistent set of expectations:
- Physical and emotional safety: The clinical environment must be free from harassment, discrimination, and conditions that threaten a student's well-being. Instructors are obligated to maintain a supportive learning environment.3
- Equitable, criteria-based evaluation: Assessments cannot rely on subjective preference. Programs must use standardized clinical evaluation tools and multiple sources of evidence, not a single instructor's impressions.1
- Diverse specialty exposure: When a curriculum promises broad clinical experiences, students have a right to placements that align with course objectives. A pediatric rotation, for instance, should involve pediatric nursing in a healthcare setting unless the program explicitly defines an alternative.
- Access to an appeal process: Every student must have a defined path to challenge an evaluation, clinical placement, or instructor conduct. This typically includes an informal review, an appeal to a committee, and, if needed, an institutional grievance process with clear timelines.1
What Fair Clinical Evaluation Looks Like in Practice
The term "fair testing" often conjures images of exams, but in nursing clinical placement quality assessment it translates to everyday practices. Programs that meet the 2024 standards build evaluation systems around:
- Rubric-based assessments that tie every competency to observable behaviors, removing guesswork for both student and instructor.4
- Multiple evaluators whenever possible, so one person's perspective doesn't dominate the final grade. The NLN emphasizes that clinical educators must rely on consistent evaluation criteria, not personal bias.3
- Mid-rotation check-ins where students receive formative feedback and a clear picture of where they stand before a summative judgment is made.1
- Written criteria shared before the rotation begins, so students understand exactly how they'll be assessed. Without this transparency, even a well-intentioned instructor can appear unfair.1
When a Rotation Falls Short
The Reddit post that sparked this guide described a pediatric rotation held at a daycare center rather than a hospital. That gap raises a question every program must answer: Is the school meeting its advertised clinical standards? If a student's experience doesn't match the published curriculum, they have grounds to seek a reassignment. A sound reassignment process, according to current standards, should be documented, time-stamped, and explained with reference to program policies, not left to an instructor's personal preferences.1
Making Rights Visible
Rights that live only in accreditation documents don't function as rights. Programs protect students best by publishing clinical rights plainly in student handbooks and reviewing them during orientation. When a complaint arises, both parties can turn to a shared written standard rather than an unwritten assumption. That shared standard becomes the foundation for every other step in the complaint management workflow, and the strongest guard against the kind of retaliation students fear.1
How External Bodies Handle Clinical Complaints
Clinical education complaints rarely stop at the program door. Three distinct external channels now shape how concerns get investigated, and nurse educators should understand what each one actually reviews before advising a student (or defending a colleague).
State Boards of Nursing
Every state board of nursing accepts complaints against licensed nurses, and that includes clinical instructors who hold RN or APRN licensure. Boards typically investigate conduct that touches licensure standards: patient safety violations, impairment, boundary breaches, fraud, or documented unprofessional behavior. They generally do not adjudicate personality conflicts, grading disputes, or scheduling gripes.
To locate the right procedure, start at the NCSBN member board directory (ncsbn.org) and follow the link to your state's board site. Look for navigation labeled "Complaints," "File a Complaint," or occasionally "Discipline" or "Student Concerns." Most boards offer an online form, a downloadable PDF, or both, along with guidance on what evidence to attach.
Programmatic Accreditors: ACEN and CCNE
Accreditors investigate the program, not the individual instructor. ACEN (acenursing.org) and CCNE (ccneaccreditation.org) both publish formal complaint policies, usually under a "Policies," "Complaints," or "Third-Party Comments" heading. Their scope is whether the program is meeting accreditation standards: clinical hour requirements, faculty qualifications, curriculum breadth across specialties, student support, and outcome data.
A single unprofessional instructor generally will not trigger accreditor action. A pattern (missing rotations, unqualified faculty, chronically shortened clinical days, retaliation against complainants) can, particularly in programs where nursing faculty shortage has led to underqualified or overburdened instructors filling clinical roles. Complainants are typically asked to show they first attempted resolution through the institution.
Institutional Ombuds
Many universities house an ombuds office under Student Affairs, the Provost, or as a standalone unit. Ombuds are confidential, informal, and neutral. They do not investigate or discipline; they coach students through options, facilitate conversations, and flag systemic patterns to leadership without naming individuals. For a student unsure whether to file formally, the ombuds is often the safest first stop.
Build Your Own Reference List
Advise students (and keep for yourself) a short personal directory with three entries: the state board complaint page, the program's accreditor complaint page, and the institutional ombuds contact. Check each source directly rather than relying on hearsay. Knowing exactly where a concern belongs prevents both wasted filings and unheard complaints.
Related Articles
Building a Culture That Prevents Complaints
Reactive damage control versus proactive prevention: most clinical programs unknowingly choose the first option until a formal complaint forces their hand. Shifting to a prevention-first mindset is the single highest-ROI investment a nursing education program can make, because most student grievances stem from structural gaps, not instructor malice.
Mandatory Onboarding for Adjunct and New Clinical Faculty
Clinical instructors often come directly from practice with deep clinical expertise but minimal teaching preparation. A required orientation module on professional boundaries, ethical student interactions, and clinical teaching fundamentals closes this gap before the first shift. Include realistic scenarios: how to handle a student who challenges your authority, appropriate use of social media, and managing dual relationships. This is not bureaucracy; it is protection for both the instructor and the students.
Structured Mentorship Pairings
Pair every novice clinical instructor with an experienced faculty mentor for at least their first full rotation. The mentor should observe a clinical day, review student evaluations mid-cycle, and hold debrief sessions focused on teaching strategies, not just clinical content. This normalizes reflective practice and catches small issues before they become formal complaints. Mentorship also signals that nursing faculty retention strategies are an institutional priority, not an afterthought.
Anonymous Mid-Rotation Feedback Loops
Traditional end-of-course evaluations come too late to help the current cohort. Insert a brief, anonymous survey at the midpoint of every clinical rotation, routed to the course coordinator, not the instructor. Ask students to rate fairness, availability, clarity of feedback, and whether they feel safe reporting concerns. Aggregate results inform just-in-time coaching for the instructor without exposing individual students. This closes the "too afraid to speak" gap that Reddit posts reveal.
Annual Self-Assessment Against Competency Frameworks
Clinical instructors should complete a yearly self-audit mapped to published competencies like the NLN Clinical Nurse Educator Competencies. This is not a punitive checklist; it is a reflective tool that identifies growth areas and documents teaching development. Programs can tie this to contract renewal for adjuncts, reinforcing that teaching quality is measured and valued. Ongoing self-assessment also supports nursing student mental health support by ensuring instructors recognize when their behavior affects student well-being.
Recognize the Adjunct Reality
Many clinical programs rely heavily on part-time adjuncts who juggle practice, graduate school, and teaching. Expecting them to intuit professional teaching standards without onboarding is unrealistic. Investing in a structured prevention system (onboarding, mentorship, feedback, self-assessment) transforms a fragmented workforce into an aligned teaching community. Programs that do this do not just prevent complaints; they retain students who would otherwise leave disillusioned, and they protect hard-won accreditation standing by demonstrating a culture of continuous improvement.
Common Questions About Reporting a Clinical Instructor
These are some of the most common questions nursing students and educators ask about the complaint process. Each answer points you to the relevant section of this guide for a deeper dive.
Every complaint a student files is also a data point about your program's clinical culture. When the institution's response is slow, opaque, or punitive toward the person who spoke up, students read that response accurately: the process exists to protect the program, not them. The paramedic-turned-nursing student who posted on Reddit, paying $130,000 in tuition while watching clinical hours get cut short and ER exposure disappear, did not lack evidence. What she lacked was confidence that reporting would lead anywhere safe.
The fix is not another policy document. Audit your complaint workflow this semester, share it with every clinical faculty member, and then ask a sample of current students whether they know it exists. If they do not, the workflow is invisible, and invisible processes do not build trust. Preventing faculty incivility in nursing education requires the same discipline: close that gap before the next complaint arrives, not after it does.