What you’ll learn in this article…
- Over one-third of nurse educators report burnout, driven by excessive workloads and high turnover.
- Nurse educators earn a median $13,000 less than clinical RNs, with gaps exceeding $40,000 in some states.
- The VA Nursing Academy's shared faculty model added 5 FTE educators per 20 students.
- Simulation-based training scales instruction, reducing the need for extensive one-on-one faculty time.
How can nursing programs admit more students when nearly one in five faculty positions sits empty? The vacancy rate has become a bottleneck that caps enrollment, leaving qualified applicants turned away. Meanwhile, healthcare demand escalates, and the pipeline of new nurses narrows, threatening patient care across the country.
This shortage doesn't just strain budgets; it loads burnout onto the educators who remain, forcing larger classes and less mentorship. The result is a vicious cycle: fewer graduates, fewer future faculty, deeper shortages.
Nurse educators are the linchpin. Solving the crisis demands institutional commitment to grow the pipeline from within, going beyond just hiring. This article explores actionable steps to do exactly that.
The State of the Nurse Educator Pipeline in 2026
The numbers paint a stark picture: nursing schools cannot find enough qualified educators, and the nurse educator shortage is leaking at both ends. While demand for nurses continues to rise, the supply of faculty is shrinking, creating a bottleneck that limits the number of students who can enter the profession.
Faculty Vacancies and the Domino Effect on Enrollment
In 2025, a survey of 863 nursing schools across the country found 1,588 unfilled faculty positions, resulting in a national vacancy rate of 7.2 percent.1 The situation forces many programs to cap enrollment, turning away thousands of qualified applicants. In 2024 alone, more than 80,000 qualified nursing school applicants were rejected,2 primarily due to insufficient faculty and clinical placements. This directly constricts the pipeline of new nurses entering the workforce.
The Retirement Time Bomb
The urgency is magnified by retirement projections. According to the American Association of Colleges of Nursing, roughly one-third of current nursing faculty are over 55 and expected to retire within the next decade.1 As these experienced educators leave, the already thin ranks become even more strained. The loss of institutional knowledge and mentorship deepens the crisis, making it harder for early-career educators to step into leadership roles.
A Pay Gap That Deters Talent
Salary disparities between clinical and academic roles continue to discourage nurses from transitioning to education. The Bureau of Labor Statistics reports that the national median annual wage for postsecondary nursing instructors is $79,940, with approximately 74,250 employed nationwide. When compared to the earning potential of advanced practice registered nurses or experienced bedside clinicians, the financial sacrifice is significant. This wage gap not only slows recruitment but also contributes to retention challenges, as educators may return to clinical roles for better compensation.
Connecting the Dots: How the Pipeline Crisis Fuels the Nursing Shortage
The faculty shortage is not an isolated problem; it is a multiplier for the broader nursing shortage. Fewer instructors mean fewer graduates, which in turn leaves hospitals and clinics understaffed. The cycle intensifies as overworked nurses burn out, further shrinking the potential pool of future educators. Addressing the educator pipeline is therefore not just an academic concern; it is a public health imperative that requires immediate, collaborative action.
Nurse Educator Salaries Vs. Clinical Nursing: A State-By-State Reality Check
A state-by-state comparison reveals that nurse educators often earn less than their clinical counterparts, with gaps exceeding $40,000 in some regions. The table below highlights median annual wages for both roles across states with available 2024 data.
| State | Clinical RN Median Salary | Nurse Educator Median Salary | Salary Difference |
|---|---|---|---|
| Alabama | $71,040 | $77,270 | +$6,230 |
| Alaska | $110,690 | $92,050 | -$18,640 |
| Arizona | $96,890 | $68,360 | -$28,530 |
| Arkansas | $77,130 | $64,330 | -$12,800 |
| California | $140,330 | $99,010 | -$41,320 |
| Colorado | $96,520 | $80,440 | -$16,080 |
| Connecticut | $101,590 | $81,490 | -$20,100 |
| Delaware | $92,610 | $83,420 | -$9,190 |
| District of Columbia | $104,550 | $103,780 | -$770 |
| Florida | $82,850 | $83,940 | +$1,090 |
| Georgia | $86,560 | $75,950 | -$10,610 |
| Hawaii | $136,320 | $102,180 | -$34,140 |
| Idaho | $86,100 | $75,420 | -$10,680 |
| Illinois | $86,410 | $78,870 | -$7,540 |
| Indiana | $80,740 | $77,270 | -$3,470 |
| Iowa | $76,960 | $71,910 | -$5,050 |
Related Articles
More than one-third of nurse educators report burnout, driven primarily by excessive workloads. This staggering figure underscores the urgent need for systemic solutions. Without institutional change, high turnover will continue to weaken the educator pipeline, compromising nursing education quality. Resilience alone is not enough; workloads, compensation, and support structures must shift.
Why the Shortage Hits Nurse Educators Hardest
The faculty shortage is often measured in unfilled positions, but its real impact is felt in the hearts and minds of nurse educators who show up every day.
The Hidden Emotional Price
Behind every empty classroom seat is a working educator juggling heavier course loads, larger clinical groups, and the weight of knowing that even more students could be trained if only there were enough instructors. Research from the National Institutes of Health reveals that as of 2023, 85.2% of nurse educators were experiencing moderate to high burnout.1 More than a third felt emotionally drained (37.5%), and 42.4% reported feeling 'used up' at the end of a typical workday. The Oldenburg Burnout Inventory scores show a mean emotional exhaustion score of 21.24, with depersonalization at 5.88, numbers that signify deep disengagement from the teaching role that once brought professional fulfillment.2
This emotional toll is compounded by the unique position nurse educators occupy: they are seasoned clinicians who made a nurse to teacher career change, yet they often feel caught between the clinical demands of preparing students for high-stakes patient care and the systemic pressures of academia. The compassion fatigue that drives nurses from the bedside does not disappear when they step into a classroom; it transforms into a constant worry about whether they are doing enough for the next generation.
When Ratios Rise, Quality Suffers
As vacancies persist, with an 8% national faculty vacancy rate reported in 20244 and 1,588 full-time positions unfilled in 2025, the educators who remain must stretch further. Higher faculty-to-student ratios mean less time for personalized feedback, decreased mentoring, and a reliance on standardized assessments that cannot replace one-on-one clinical guidance. This not only erodes teaching quality but directly fuels the frustration that pushes skilled educators toward the exit. In 2024 alone, over 80,000 qualified nursing student applications were turned away because of the nursing faculty shortage.4 Each rejection letter is a silent blow to the morale of the faculty who want to say yes.
Burnout and Retention: The Unsustainable Loop
The link between burnout and intention to leave is stark: 84.9% of nurse educators reported moderate to high levels of disengagement, a predictor of turnover.1 Midcareer faculty, who should be the backbone of any program, showed even higher emotional exhaustion scores (23.55), suggesting that experience does not confer resilience under current conditions.3 Addressing burnout is no longer optional, it is the linchpin of retention and demands dedicated nurse educator burnout prevention. Without systemic support, even the most innovative recruitment strategies will fail, because new hires will enter the same draining environment that drove their predecessors out. The nurse educator pipeline will not strengthen until we treat the educators already in it as the precious resource they are.
Recruitment Strategies: Tapping Overlooked Talent Pools
Traditional faculty hiring pipelines are no longer enough. To close the educator gap, nursing programs must look beyond the obvious and actively court four underutilized talent pools: retired faculty, nurse practitioners, experienced clinical nurses, and their own alumni. Each group brings distinct strengths, and targeted incentives can make the leap into teaching both attractive and sustainable.
Tapping Retired Faculty
Seasoned educators who recently left the classroom often miss the connection with students and are willing to return, if the terms are right. Return-to-teach stipends, phased retirement tracks that blend mentoring with reduced courseloads, and flexible schedules that respect their lifestyle can draw them back. Faculty-sharing agreements between neighboring institutions also let retirees teach a single course without a full-time commitment. These approaches keep institutional knowledge alive while easing the onboarding burden.
Engaging Nurse Practitioners and Advanced Practice Nurses
NPs and other advanced practice nurses bring clinical depth and are often eager to teach but can’t afford the pay cut. Joint appointment models bridge this gap: institutions partner with health systems to offer salary enhancements, so NPs can teach one or two days a week while maintaining their clinical caseload. The model works especially well in Dedicated Education Units, innovative teaching strategies in nursing education where students learn on designated hospital units under the same clinicians who teach their coursework.1 For the practitioner, it offers career flexibility without financial penalty.
Clinical Nurses: The Bedside-to-Classroom Bridge
Many of the most effective faculty start as bedside nurses who try adjunct teaching. The Northeast Ohio Nursing Clinical Adjunct Faculty Initiative, led by the Cuyahoga County Healthcare Sector Partnership and funded by Cleveland Clinic and University Hospitals, exemplifies this pathway.2 It recruits experienced clinical nurses into part-time instructor roles, directly reducing student waitlists and expanding program capacity. Similar partnerships across the country offer onboarding support, tuition assistance for online nursing education degrees, and the promise of full-time tracks after a successful adjunct stint. For nurses, it’s a low-risk way to test the educator waters.
Alumni: Growing Your Own Educators
Graduates who already know a program’s culture, values, and clinical partners are prime recruitment candidates. Internal graduate pipelines, where schools intentionally mentor BSN or MSN alumni into faculty roles, can shorten hiring timelines and boost retention. The Nurse Faculty Loan Repayment Program helps make this path financially viable by forgiving portions of educational debt for those who teach in accredited nursing schools. When combined with alumni networking and dedicated “faculty fellow” roles, these pipelines turn loyal graduates into the next generation of educators.
Prioritizing Diversity in Recruitment
A faculty that mirrors the student body improves educational outcomes and helps close equity gaps. Strategies include targeted outreach at minority-serving institutions, mentoring circles for underrepresented students who express teaching interest, and partnerships with diverse clinical sites that naturally surface potential instructors. Assigning diverse search committee members and advertising roles in community and professional networks that reach minority nurses also moves the needle.
Proven Programs Delivering Results
Successful initiatives are already making a difference. The Northeast Ohio initiative has moved into full implementation, showing that clinical-to-classroom pipelines can be built when academic and healthcare employers share the investment. Meanwhile, the Nurse Faculty Shortage Reduction Act, introduced in Congress, proposes grants to schools that close the compensation gap between clinical nursing and faculty roles.3 At the institutional level, schools that combine joint appointments, loan repayment, and flexible return-to-teach pathways report more robust applicant pools and lower faculty turnover, proving that when the profession invests in its teachers, nurses answer the call.
Building Academic-Practice Partnerships That Last
The VA Nursing Academy (VANA) demonstrated a shared faculty model that adds 5 full-time equivalent (FTE) educators for every 20 students, keeping a 4:1 student-to-faculty ratio while meeting hiring targets.1 This scalable approach helps schools struggling to recruit faculty by tapping into the expertise of practicing nurses.
The Shared Faculty Model: Bridging Education and Practice
In a shared faculty arrangement, clinicians work part-time in both classroom and bedside. Hospitals gain staff current with evidence-based teaching; nursing programs benefit from instructors with real-world clinical currency. Cost-sharing splits salaries between the institution and clinical partner, and MOUs formalize workload, compensation, and liability.
Case Studies: Partnerships That Delivered Results
Several partnerships demonstrate results: an academic medical center and college of nursing partnership, documented by the American Organization for Nursing Leadership (AONL), created six new faculty positions with a $1.5 million grant and lifted nurse retention from 68% to 84% at the affiliated hospital.2 An Alabama university and medical center partnership reduced hospital-acquired pressure injuries from 2,000 per year to 10 per month and opened two new clinics.2 Illinois State University's CAUSE project added four clinical preceptors, expanding placement capacity.3
Blueprint for a Sustainable Partnership
To build lasting collaboration, start with an MOU that defines funding splits, faculty oversight, and shared metrics. A joint steering committee ensures equal voice. Align incentives: hospitals gain a recruitment pipeline and professional development, while schools gain clinical placements and adjunct faculty. Regular data sharing keeps the partnership responsive.
Elevating Student Outcomes
When faculty still practice, students develop clinical judgment in nursing beyond textbooks. These partnerships boost NCLEX pass rates and shorten the transition to practice. Preceptorships and dedicated education units give more hands-on time, building confidence. Graduates often stay local, strengthening the workforce and sometimes returning as future educators.
Federal and State Funding to Grow the Pipeline
Securing funding for nurse educator programs often means choosing between short-term staffing needs and long-term pipeline investments. While every dollar spent on faculty development today delays filling a vacant clinical or classroom position, the cost of inaction , a shrinking educator workforce that can’t support student enrollment , is far greater. Smart institutions and individual educators are leveraging a mix of federal, state, and institutional dollars to break this cycle.
Federal Lifelines: Title VIII and the Nurse Faculty Loan Program
The Health Resources and Services Administration (HRSA) administers Title VIII Nursing Workforce Development programs, a cornerstone of federal support. These grants fund advanced education, traineeships, and loan repayment for nurses who commit to teaching. The Nurse Faculty Loan Program (NFLP) is particularly attractive: it provides loans to graduate students in approved programs, with up to 85% forgiveness for those who serve as full-time nurse faculty after graduation. Eligibility typically requires enrollment in a participating institution and a commitment to a faculty role. Application deadlines and funding cycles vary annually, so checking the HRSA website regularly is essential. Since federal appropriations shift with each budget cycle, don’t assume these opportunities will remain unchanged; proactive monitoring is key.
State-Level Grants and Workforce Initiatives
Many states operate nursing workforce centers or allocate funds through boards of nursing specifically to bolster the educator pipeline. These grants may cover tuition for graduate courses, salary supplements for new faculty, or stipends for preceptors. State programs often prioritize rural or underserved areas, creating a chance for smaller nursing schools to compete. To uncover these opportunities, visit your state board of nursing website or connect with your state’s nursing workforce center , if one exists. Even when grants aren’t advertised widely, a direct inquiry can reveal pilot programs or planning funds.
How to Find and Secure Funding
Professional organizations like the American Association of Colleges of Nursing (AACN) and the National League for Nursing (NLN) frequently announce funding opportunities, scholarships, and research grants tailored to educator development. Subscribe to their newsletters or member alerts. At the institutional level, nursing schools often have internal grants, loan forgiveness, or tuition remission for faculty-track students. Financial aid offices can point you toward these, but don’t overlook informal channels: a conversation with a department chair or dean can surface discretionary funds set aside for pipeline building. By combining multiple sources , a federal loan, a state stipend, and an institutional scholarship , you can significantly lower the financial barrier to entering the educator workforce.1
Questions to Ask Yourself
Innovating Education: Simulation, Preceptorships, and Technology
Traditional clinical placements, while essential, often strain faculty resources with high student-to-instructor ratios; in contrast, simulation-based training offers a scalable, controlled environment where students build competence with less one-on-one instructor time. This shift is not just about logistics; it's about reimagining how we prepare nurses for a complex healthcare landscape.
Simulation and Virtual Reality: Scaling Clinical Learning
High-fidelity mannequins and virtual reality (VR) platforms create immersive, repeatable clinical scenarios without requiring a faculty member at every bedside. Students can practice rare, high-stakes situations, like a pediatric code or anaphylactic shock, multiple times until mastery, receiving immediate, standardized feedback. For faculty, this means one instructor can oversee several simulation stations simultaneously, dramatically extending reach. Institutions adopting these tools report that up to 50% of clinical hours can be replaced with simulation without compromising competency, per national guidelines.
Preceptorships: Leveraging Clinical Expertise
Preceptorships pair students with experienced clinical nurses who mentor them in real patient settings. This model shifts day-to-day supervision to practicing professionals, freeing academic faculty to focus on curriculum design, evaluation, and student support. Preceptors gain leadership experience, while students get hands-on, real-world learning. Crucially, this partnership strengthens the bridge between academia and practice, helping retain expert nurses who might otherwise leave the bedside.
Online and Hybrid Teaching Models
Online and hybrid programs break geographic barriers, allowing one master educator to reach hundreds of students asynchronously. Interactive modules, discussion boards, and virtual office hours help educators build more engaging online courses, maintaining engagement without demanding on-campus presence. Modular, self-paced content can be updated quickly and reused across cohorts, reducing the need for multiple instructors teaching identical material. This model is especially powerful for didactic components, reserving in-person time for simulation and clinical experiences.
Evidence of Effectiveness
- NCLEX pass rates: Multiple studies show that programs heavily utilizing simulation and preceptorships maintain or exceed national average pass rates on the Next Generation NCLEX, with some reporting increases of 3, 5 percentage points.
- Student satisfaction: Surveys consistently indicate higher engagement and confidence among learners exposed to VR and realistic simulations, as they feel better prepared for clinical rotations.
- Scalability: As highlighted by Wolters Kluwer, simulation and preceptorships are scalable solutions that directly address the faculty shortage, enabling programs to expand enrollment without proportionally increasing faculty headcount.1
These innovations not only mitigate the educator shortage but also create a more dynamic, resilient nursing workforce ready for tomorrow's challenges.
Nurse Educators Earn $13,000 Less Than RNs
The national median salary gap remains a persistent deterrent to entering academia.
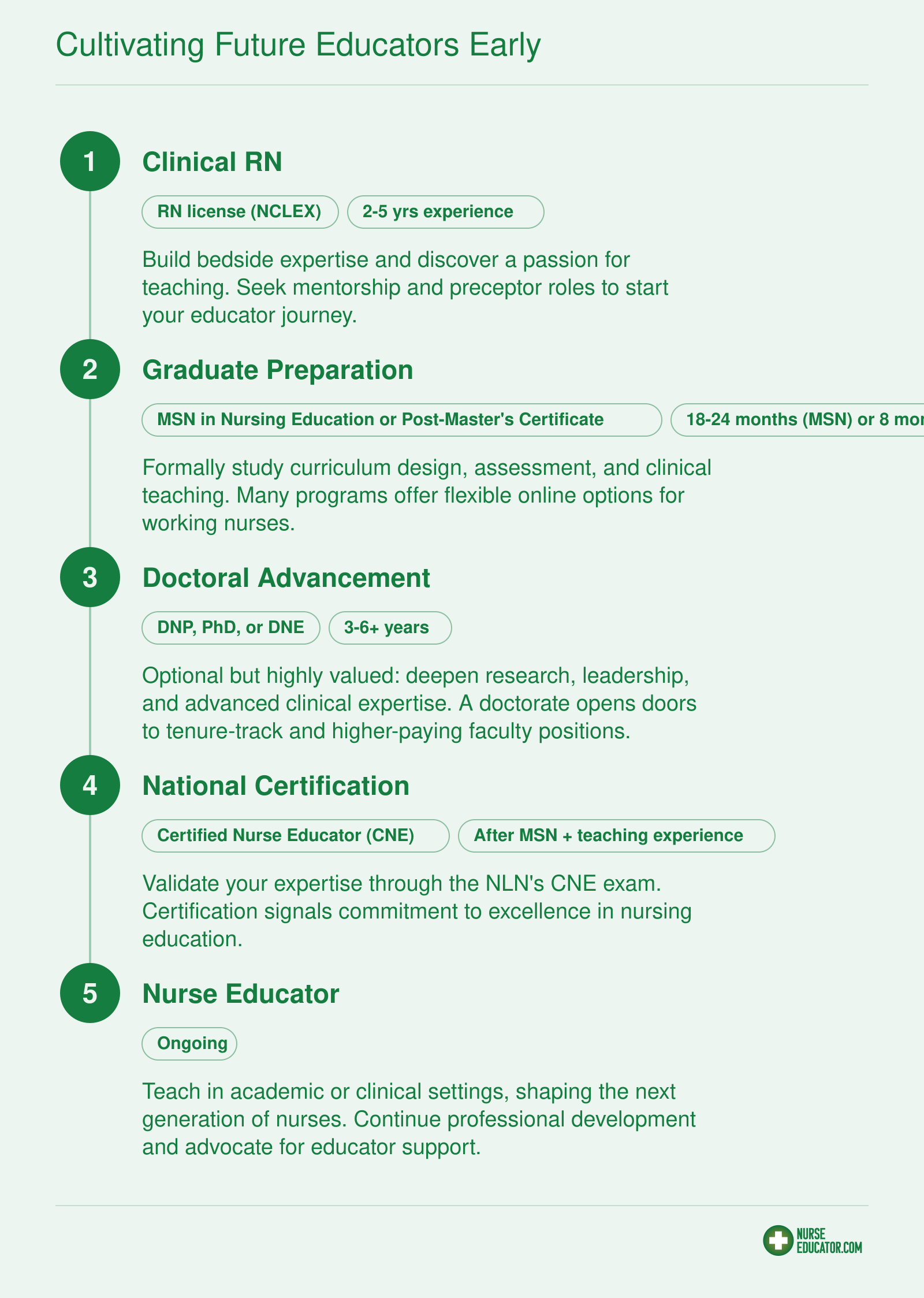
Cultivating Future Educators Early
Building the nurse educator pipeline starts with a clear, accessible career pathway. By embedding teaching tracks early and offering flexible educational options, we can inspire more clinical nurses to become faculty.
Questions to Ask Yourself
Your Action Plan: From Individual to Systemic Change
Transforming the nurse educator pipeline requires action, not just awareness. Whether you are a faculty member, department chair, or clinical instructor, the strategies below give you a concrete starting point. Pick one initiative, gather allies, and let results fuel broader institutional change.
The Five-Step Action Checklist
- Audit compensation: Compare your department's salaries to local clinical nursing roles using publicly available data. Present evidence of the gap to administration and human resources, framing it as a recruitment and retention risk. Even a partial parity adjustment can shift morale.
- Explore joint appointment models: Partner with a nearby hospital or health system to create shared educator-clinician roles. These positions let nurses teach part-time while maintaining clinical hours, bringing current practice into the classroom and easing salary pressure.
- Apply for Title VIII or state grants: Federal Nursing Workforce Development programs and many state-level initiatives offer funding for faculty development, loan repayment, and program expansion. Designate a grant-writing lead, even if it is a rotating faculty role, to pursue these dollars annually.
- Introduce simulation technology: High-fidelity manikins, virtual reality, and standardized patient encounters can reduce demands on clinical placement sites and allow educators to manage larger groups without sacrificing quality. Pilot one module, measure student outcomes, and use the data to justify investment.
- Start a mentorship program: Pair experienced educators with bedside nurses who show teaching aptitude. A structured, low-cost mentorship that includes co-teaching, shadowing, and guided lesson planning can cultivate the next generation of faculty from within your own ranks.
Start Small, Build Momentum
Institutional change can feel overwhelming. Begin with the action that requires the least upfront cost or political capital, perhaps a three-month mentorship pilot or a single grant application. Publicize early wins through faculty meetings and newsletters to demonstrate that the pipeline can be strengthened with existing resources. As support grows, advocate for formalized policies and budget lines.
A Collective Effort with Far-Reaching Impact
Solving the nurse educator shortage is not a single department's responsibility; it is a profession-wide challenge. Every preceptor who sparks a student's desire to teach, every dean who reallocates funds toward faculty support, and every policymaker who champions loan forgiveness contributes to the solution. By acting together, we do more than fill vacancies, we ensure that nursing education remains vibrant, evidence-based, and capable of preparing the clinicians our communities will need for decades to come.