What you’ll learn in this article…
- In 2026, 75-84 conference voters reached consensus on just 7 of 11 proposed digital education statements.
- Embedding virtual care training and digital literacy assessment into curricula received clear endorsement.
- Partnerships with informatics leaders are essential for aligning nursing education with clinical digital practice.
- Adaptability and critical digital thinking must replace fixed tool-specific checklists that rapidly become obsolete.
As telehealth, AI-driven clinical decision support, and electronic health records reshape patient care, pre-registration nursing curricula remain largely anchored to pre-digital models. The gap between what students experience in clinical placements and what they learn in class is widening.
In May 2026, a stakeholder consensus led by Matthew Wynn and Dr. Clare Van Miert at Liverpool John Moores University tackled this misalignment head-on. Published in Nursing Times, the process gathered 75 to 84 votes per statement at the Digital Nursing Conference, yet achieved full agreement on only 7 of 11 proposals, underscoring just how contested and urgent the digital capability discussion has become.1
The watershed finding: nursing education must shift from ticking off fixed technology competencies to cultivating adaptable, critical digital thinkers. The strategies that follow translate this consensus into actionable steps for faculty and curriculum redesign, confronting the reality that the next generation of nurses cannot afford to be digitally unprepared.
Why Digital Capabilities Matter More Than Digital Competency
In 2026, when 75 to 84 nursing education stakeholders voted on 11 digital education statements at the Nursing Times Digital Nursing Conference, only 7 achieved full consensus, a clear signal that fixed competency lists cannot keep pace with clinical technology.1
The Competency-Capability Divide
Digital competency suggests a checklist of discrete, measurable skills: logging into an EHR, sending a secure message, updating a patient portal. These are important baseline abilities, but they are narrow and tool-dependent. Digital capability, in contrast, is the adaptive, critical capacity to engage with evolving technologies across varied care contexts. It means a nurse can evaluate new software, integrate it thoughtfully, and even educate peers and patients, not just demonstrate proficiency with today's interface.
Why Fixed Lists Fail in a Rapidly Evolving Field
The stakeholder consensus published in Nursing Times (Wynn & Van Miert, 2026) exposed the core problem: technologies change faster than curricula can be rewritten.1 Proposals for a universal proficiency list generated intense debate, with the advisory panel ultimately concluding that such lists are impractical. What is essential today, a specific telehealth platform, a data dashboard, may be obsolete in three years. Nursing programs that lock curricula to static competencies risk producing graduates stranded when the tools shift.
From Generic Frameworks to Nursing-Specific Digital Judgment
General digital frameworks like the Jisc digital capabilities model provide helpful scaffolding. They highlight domains such as information literacy, communication, and content creation. Yet these alone are insufficient for nursing. The consensus emphasizes that curricula must layer nursing-specific clinical judgment in nursing on top of generic digital skills. For instance, the "4 C's" of digital literacy, critical thinking, creativity, communication, and collaboration, take on distinct meaning in a healthcare setting:
- Critical thinking: Not just evaluating source credibility, but assessing whether an AI-generated risk score aligns with a patient's presentation and social history.
- Creativity: Troubleshooting a video lag during a home dialysis teaching session by pivoting to a phone call while sharing screens.
- Communication: Choosing when a secure text, a video visit, or an in-person encounter best serves a vulnerable patient who is also a digital novice.
- Collaboration: Co-designing digital discharge instructions with a multidisciplinary team so they are accessible, actionable, and culturally safe.
Inextricable from each skill is the ability to teach. Nurses educate patients and families on self-monitoring apps, medication reminders, and virtual ward routines. That pedagogical layer, simplifying, demonstrating, coaching, is absent from generic digital frameworks but central to nursing capability. Educators who want to explore what this teaching dimension looks like across the full nursing education curriculum will find that digital capability threads through nearly every subject.
Shifting the Assessment Question
For nursing educators, the practical reframe is clear: stop asking "Can the student use Tool X?" and start asking "Can the student evaluate, adapt, and teach with any digital tool in a care context?" This means designing assessments that present unfamiliar digital scenarios, not rehearsed click-paths. It also means embedding digital capability early. As the consensus recommends, a baseline digital literacy assessment at program entry ensures students learn to learn digitally, not just to perform digitally.1
What the 2026 Stakeholder Consensus Recommends
The tension between standardising digital competencies and preserving the adaptability required for evolving clinical environments sits at the heart of the 2026 stakeholder consensus published in Nursing Times. Nurse educators face a pressing question: should we pursue a fixed checklist of skills, or cultivate a mindset capable of navigating technology that does not yet exist? The consensus, built on a rigorous three-phase process, provides clear direction.
How the Consensus Was Reached
A group of 28 experts and stakeholders, convened by Matthew Wynn and Dr Clare Van Miert of Liverpool John Moores University, used a three-phase methodology to arrive at actionable recommendations.1 Phase one was a rapid review of 49 articles and 16 digital capability frameworks, establishing the evidence base for nursing's unique digital demands. Phase two gathered qualitative insight from a survey of 34 participants, capturing perspectives from practice, education, and policy. Phase three culminated in live voting (75 to 84 votes per item) and roundtable discussions with 28 attendees at the Nursing Times Digital Nursing Conference. This iterative process ensured that the final guidance reflected frontline realities, not just theoretical ideals.
The Seven Agreed Statements
The consensus achieved agreement on seven out of eleven initial statements, representing a core set of priorities for pre-registration curricula:
- Practice partnerships: Align curricula with clinical practice through formal academic-practice partnerships, including collaboration with informatics leaders.
- Virtual and remote care: Explicitly train students to deliver care via telehealth, remote monitoring, and other virtual modalities.
- Critical engagement: Develop the ability to critically evaluate digital tools, data, and sources of information, rather than simply operating them.
- Clinical data interpretation: Integrate skills for interpreting patient data, dashboards, and digital decision-support tools into clinical reasoning.
- Peer and patient education: Prepare students to educate patients, families, and colleagues in the use of digital health technologies.
- Adaptive troubleshooting: Foster adaptive capabilities for solving novel digital problems, acknowledging that technology and workflows will evolve.
- Baseline digital literacy assessment: Screen students' foundational digital literacy at programme entry to identify support needs early.
These statements shift the focus from static competency checklists to a dynamic, patient-centred approach. Notably, the panel rejected the notion that pre-registration curricula should cover business case writing or digital leadership; those areas, they argued, belong in postgraduate or CPD programmes.1
Who Shaped the Guidance
The advisory panel's breadth signals that digital capability is not solely an educational concern but a whole-system challenge. Members included Professor Dawn Dowding (University of Manchester), Professor Natasha Philips (FutureNurse), Dr Cristina Vasilica (University of Salford), Abigail Swindail (Digital Health and Care Wales), James Freed (NHS Digital Academy), Peter White (Alder Hey Children's Hospital), patient representative George Norton, and Simon Noel (NHS England). This blend of clinical informatics, policy, higher education, and patient advocacy grounded the recommendations in practice and underscored the need for cross-sector ownership.
What Belongs at Postgraduate Level
One of the clearest boundary lines drawn by the consensus is that skills such as digital leadership, business case writing, and system procurement are not entry-level expectations. Instead, they are advanced competencies suited for post-registration specialisation or continuing professional development. This distinction frees pre-registration educators to concentrate on foundational, adaptive capabilities without overloading the curriculum, a concern that resonates given the ongoing nursing faculty shortage. It also signals to employers that newly qualified nurses will be ready to participate in digital practice but may need further development to lead it. The peer and patient education statement, meanwhile, reinforces that nurses teaching patients about digital health tools is not optional; it is a core graduate-level expectation.1
Key Takeaway: Adaptability Over Checklists
Fixed lists of digital proficiencies quickly become outdated as technology evolves. The 2026 stakeholder consensus urges nurse educators to stop chasing tool-specific checklists. Instead, design curricula that build adaptive, critical digital thinking, preparing students to navigate any emerging tool with confidence, not just master today's technologies.
Global Digital Capability Frameworks Compared: ANMF, RCN, Jisc, TIGER, and ANA
When selecting a digital capability framework, educators face a fundamental choice: adopt a broad, cross-sector model or commit to a nursing-specific scaffold. While generic frameworks offer flexibility, the 2026 stakeholder consensus makes clear that nursing education requires tailored guidance to prepare students for the unique digital demands of clinical practice.
Why Generic Frameworks Fall Short
The consensus process highlighted that frameworks like the Jisc Digital Capability Framework, while valuable for baseline digital literacy, lack the clinical context nursing students need. They do not address critical tasks such as interpreting patient data from electronic health records, conducting virtual consultations, or navigating the ethical complexities of digital professionalism in healthcare. Nursing-specific adaptation ensures that digital capabilities are woven into patient-centred care rather than treated as a separate skillset. If you are already rethinking how to structure course content around these capabilities, our overview of innovative teaching strategies in nursing education offers complementary ideas.
Side-by-Side Framework Comparison
The five frameworks below represent the most commonly cited models in nursing education. Each offers a different lens: generic versus nursing-specific, competency-based versus capability-oriented.
- ANMF National Nursing and Midwifery Digital Health Capability Framework (Australia): Developed by the Australian Digital Health Agency and targeted to all nurses and midwives across roles, settings, and career stages.1 Five domains: Digital professionalism, Leadership and advocacy, Data and information quality, Information-enabled care, and Technology.2 Structured into Formative, Intermediate, and Proficient levels for self-assessment, curriculum mapping, and CPD planning.3 Updated to version 1.1 in 2024.4
- RCN Digital Literacy Framework (UK): Designed for nurses and nursing students. Domains include digital literacy, digital professionalism, data management, and technology use. Nursing-specific and actively maintained by the Royal College of Nursing, with regular sector guidance.
- Jisc Digital Capability Framework (UK): Cross-sector for higher education and research. Six elements: ICT proficiency, information literacy, digital creation, communication and collaboration, digital identity and wellbeing, digital learning and development. Generic, updated periodically, with the most recent version reflecting post-pandemic digital shifts.
- TIGER Competencies (US/EU): Developed through international collaboration for nursing informatics. Covers areas such as clinical information management, data analytics, and system design. Nursing-specific but with a sharper focus on informatics roles. Has evolved through TIGER 2.0 and regional adaptations in Europe.
- ANA Informatics Competencies (US): Outlines expectations for nurses at all levels. Domains span data use, technology, and health policy. Nursing-specific and embedded within the ANA Scope and Standards of Practice, with the most recent guidance issued in 2015 and incremental updates thereafter.
How to Select a Starting Framework
Educators should begin by mapping their program's current digital learning outcomes against a nursing-specific framework such as the ANMF or RCN model. These offer domain language and progression levels that translate directly into clinical education. The Jisc framework can supplement foundational digital literacy, while TIGER and ANA serve programs emphasizing informatics or leadership. The consensus recommends avoiding rigid checklist adoption; instead, use a framework as a conversation tool with practice partners to tailor digital capability development to local healthcare realities. Faculty who want to pursue this kind of curriculum research more formally may find practical guidance in our article on fostering research culture in nursing education.
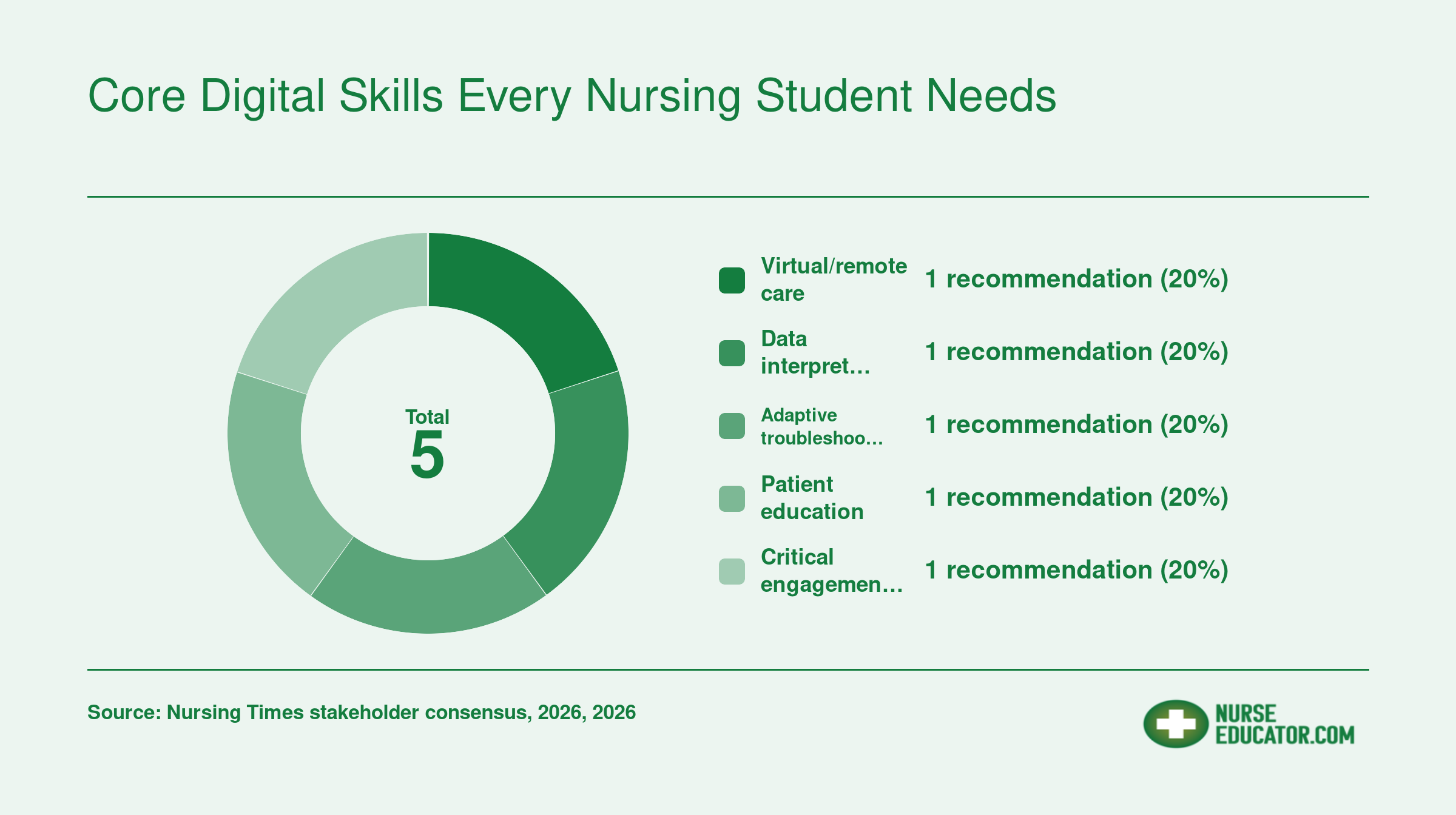
Core Digital Skills Every Nursing Student Needs
Based on the 2026 Nursing Times Digital Nursing Conference stakeholder consensus, five core digital skill clusters emerged as essential for pre-registration nursing students. Each area below is anchored by a specific recommendation.
Assessing Baseline Digital Literacy at Program Entry
What validated tools can nursing programs use to assess incoming students' digital literacy for clinical practice?
Why Baseline Assessment Matters
Nursing students arrive with vastly different digital experiences. Some have only basic smartphone skills, while others are comfortable with data analysis or coding. The 2026 stakeholder consensus recommends assessing digital literacy at entry to pre-registration programs, not as a gatekeeper but to identify gaps early. Without a structured baseline, educators risk assuming a false level of readiness, leaving some students struggling and others unchallenged.
Validated Instruments for Nursing-Specific Digital Literacy
Generic IT confidence surveys do not reliably predict clinical digital competence. Instead, nurse educators can choose from several tools designed with healthcare contexts in mind.1
- Digital Health Nursing Competency Scale (DHNCS): Developed by South Korean researchers in 2024, this instrument contains 20 to 40 items and measures self-assessed competency in digital nursing practice. It was validated with Korean nurses and nursing students and showed a Cronbach's alpha of 0.80, indicating good internal consistency. It is not open access, so institutions may need to contact the authors for permission.
- C-DMLIT (Chinese Digital Media Literacy Tool): This scale focuses on digital media literacy within health professions education. Validation details remain limited in English-language publications, but it provides a structured self-assessment for students in Chinese-speaking contexts. Programs serving diverse cohorts may find it useful after local validation.
- Teacher Digital Literacy Questionnaire: Developed by researchers of nurse educators in 2024, this tool assesses academic staff's own digital literacy with a reliability of 0.70. It is freely available and can be adapted to probe students' perceptions of their educators' digital readiness, which indirectly highlights areas where students may lack role models.
- Northstar Digital Literacy Assessments: These publicly available digital literacy assessments are psychometrically validated and measure basic computer and internet skills. While not health-specific, they offer a low-stakes way to verify essential tasks like navigating learning management systems or using spreadsheet functions. Modules can be cherry-picked for nursing contexts.
An upcoming tool, NURS-DIAL, developed by the AI4Health consortium, promises to assess both digital literacy and AI competencies specifically for nurses and nursing students.2 It remains in early development and is not yet ready for classroom use.
Designing a Phased Assessment Approach
A single snapshot at orientation is insufficient. A phased strategy aligns with the consensus call for adaptability. Educators who already excel at qualities of a good nurse educator like adaptability and learner-centered design will find this framework intuitive.
- Entry: Self-assessment. Use a short, custom questionnaire on students' comfort with common digital tasks (e.g., telehealth platforms, electronic health records, data privacy). Pair it with a Northstar module to ground-truth skills.
- Mid-program: Validated instrument. Administer the DHNCS or an adapted Teacher Digital Literacy Questionnaire to measure growth in clinical digital reasoning, not just tool use.
- Exit: Portfolio demonstration. Students compile evidence of digital competency, such as a telehealth simulation recording, a data analysis project, or patient education materials, evaluated against program learning outcomes.
Interpreting Results and Building Remediation Pathways
Avoid the common pitfall of assuming a student's comfort with social media or basic office software translates to clinical digital readiness. Instead, map results to specific curriculum objectives. For students scoring low on the DHNCS or Northstar, design modular remediation pathways: digital skills bootcamps, peer mentoring, or supplementary online modules focused on clinical scenarios. Track progress and reassess before high-stakes placements.
Ask Yourself: Is Your Program Ready?
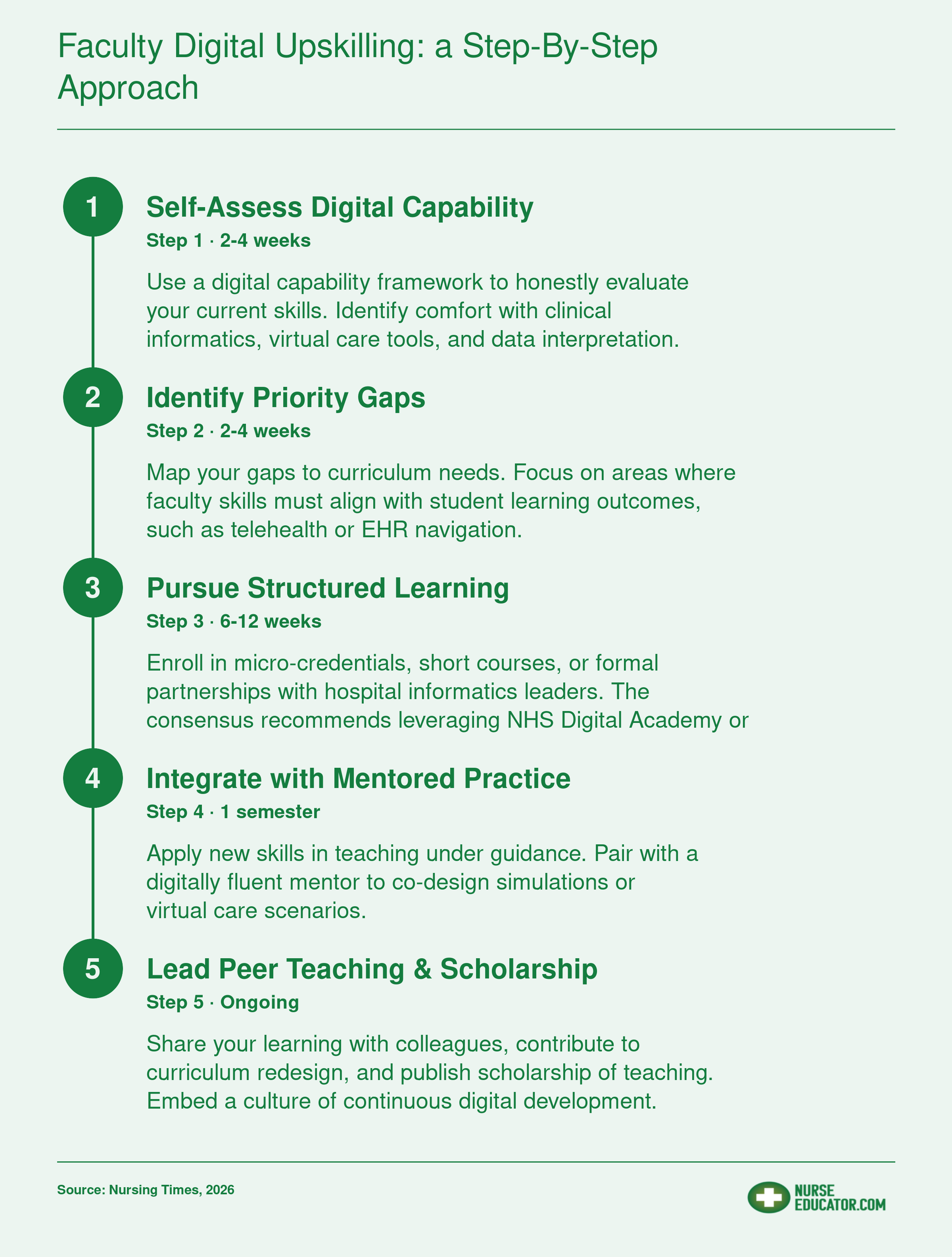
Faculty Digital Upskilling: A Step-by-Step Approach
No other resource offers nursing programs a systematic step-by-step plan for faculty digital upskilling. The 2026 stakeholder consensus specifically calls for partnerships with digital health informatics leaders, not just as a student resource but as a core faculty development strategy.
How Nursing Programs Are Actually Doing It: Implementation Examples
Some programs bolt a digital health module onto an unchanged curriculum; others rebuild clinical placements and simulation around telehealth, informatics, and data literacy. The programs seeing the strongest outcomes adopt the second approach, and they share a common thread of deep academic-practice partnership, exactly as the 2026 consensus recommends.
Australian Innovation: La Trobe and James Cook Lead the Way
La Trobe University launched an online course, "Digital Health Foundations for Nursing and Midwifery," in 2023, targeting undergraduate students.1 The course introduces digital health concepts, including electronic health records, telehealth, and cybersecurity, so that learners enter placements with a solid foundation. This directly operationalises the consensus call for baseline digital literacy assessment at program entry, though La Trobe integrates it as a proactive learning module rather than a gatekeeping test. Early feedback suggests students feel more confident navigating digital systems during clinical experiences, though formal outcome data is still being gathered.
James Cook University integrated an Academic Electronic Health Record (AEHR) platform across several undergraduate nursing subjects in 2024.2 Students use the AEHR to document care, interpret clinical data, and simulate real-time decision-making. The result? Measurably improved student confidence and perceived work readiness, according to institutional surveys. This example aligns with the consensus emphasis on training students in critical engagement with digital tools and clinical data interpretation, as well as fostering adaptability through hands-on practice. The university achieved this through a close partnership with health service providers, ensuring the platform mirrors actual clinical environments. A broader review of digital health education in Australian universities confirms that these gains in knowledge and self-efficacy are consistent across multiple institutions adopting similar models.
United States: Telehealth and EHR Integration Scale Up
American nursing schools have increasingly embedded telehealth and virtual care modules, often in partnership with hospital systems and EHR vendors. A 2024 scoping review found statistically significant gains in digital health knowledge, self-efficacy, and perceived competence among students.3 Many of these interventions also include high-fidelity simulation and virtual reality scenarios that replicate remote patient encounters, directly addressing the consensus recommendation to train students in virtual and remote care. Employer feedback from these partnerships indicates that graduates arrive better prepared to function in technology-rich care settings.
United Kingdom: Virtual Care Simulations Build Real-World Confidence
In the UK, nursing programmes have prioritised video-consultation simulations and remote triage exercises, often co-developed with NHS Digital Academy and local trusts.4 These modules teach students to communicate effectively via digital platforms, manage remote patient assessments, and troubleshoot common technical issues, all skills that map to the consensus's adaptive troubleshooting and virtual care goals. While rigorous outcome metrics are still emerging, early employer feedback points to stronger graduate confidence and faster onboarding in digitally enabled roles. The collaborative design process itself embodies the consensus call for academic-practice partnerships to align curricula with real-world needs, and it reinforces the importance of building a research culture in nursing education to evaluate these emerging pedagogies over time.
Digital Tools and Technologies Reshaping Nursing Education
What digital tools are actually making a measurable difference in nursing students' clinical readiness today? The landscape has matured considerably in 2025 and 2026, moving from pilot curiosity to core curricular components. Below we break down four tool categories that are reshaping how nursing faculty teach and how students learn.
VR and Immersive Simulation Platforms
Virtual reality simulation has expanded beyond task repetition, now fostering clinical reasoning, communication, and empathy.1 Several platforms have emerged as leaders in nursing education.
- vrClinicals for Nursing (Wolters Kluwer & Laerdal Medical, 2025): This platform integrates conversational AI, enabling students to practice natural-language interactions with virtual patients. It is aligned with Lippincott CoursePoint for seamless curriculum mapping.2 Schools report improved student confidence, communication skills, and clinical decision-making, though direct NCLEX outcome evidence remains insufficient.3
- UbiSim: A VR platform built exclusively for nursing, offering multi-patient, multi-scenario immersion adaptable across program levels. It is praised for boosting self-efficacy and knowledge retention.4
- Oxford Medical Simulation and SimX: These provide interprofessional, multi-user VR environments. Studies note enhanced empathy and teamwork, alongside high student satisfaction.5
Telehealth and Virtual Care Training Platforms
The shift toward virtual care demands that students master webside manner just as thoroughly as bedside manner. Training now occurs through dedicated telehealth OSCEs, vendor-supplied VR modules, and EHR-integrated video encounters.6
Typical formats include synchronous video visits with standardized patients, asynchronous case management exercises, and combined EHR/video sandbox simulations. These modalities improve students' comfort with remote assessment, coaching, and documentation in a distributed care environment.
AI-Assisted Clinical Decision Support in Education
Artificial intelligence is increasingly woven into simulation platforms to provide real-time, adaptive feedback. While standalone AI decision-support tools for prelicensure education remain rare, the conversational AI now embedded in vrClinicals for Nursing represents a significant leap.2 Students receive dynamic cues, evaluate patient data critically, and adjust their clinical reasoning on the fly, skills central to the 2026 stakeholder consensus. For faculty looking to pair these tools with broader active learning strategies in nursing, the combination can reinforce clinical judgment far more effectively than either approach alone.
EHR Training Environments
Electronic health record fluency is no longer optional. Academic EHRs (like those from Cerner/Oracle Health and Epic sandboxes) give students a safe space to practice documentation, order entry, and data interpretation. Programs using these report markedly improved documentation accuracy.6 Integration with existing learning management systems is often available through LTI standards, though costs vary widely based on concurrent users and institutional licensing.
Practical Guidance for Evaluating and Adopting Digital Tools
When selecting any of these technologies, consider three criteria:
- Educational fit: Does the tool address a clearly defined learning gap? Pilot it with a small cohort and measure outcomes such as skill gain, clinical judgment, or student satisfaction. Avoid tools that merely replicate didactic content without meaningful interactivity.
- Cost and infrastructure: VR platforms require headset investments and IT support. Web-based simulations may run on existing hardware. Clarify whether pricing is per student, per year, or a perpetual license, and budget for faculty training.
- LMS integration: Seek tools with LTI 1.3 or SCORM compliance so assignments and grades flow automatically into your existing system (Canvas, Blackboard, etc.). This reduces administrative friction and supports scalable adoption.
As you evaluate options, nurse educator resources and tools on our site can help you compare platforms and build a business case for adoption.
Unresolved Debates and Future Research Priorities
The 2026 stakeholder consensus delivered clear guidance, yet it also spotlighted tensions that have no universal answer. Wrestling with these openly strengthens programs far more than pretending they are settled.
Where Consensus Leaves Off: Three Areas of Active Debate
- Nursing theory and digital curricula: Some argue that established nursing models must explicitly frame digital practice, while others see them as flexible enough without a dedicated overhaul. The debate centers on whether adding new theoretical layers risks diluting core nursing philosophy.
- Coding and design skills: Stakeholders disagree about whether every nurse should gain basic technical proficiencies like coding or interface design. Proponents see these as empowering for clinical innovation; critics warn of scope creep and unrealistic expectations for pre-registration education.
- A universal proficiency list: The consensus rejected a fixed checklist, but the feasibility of any shared national or international list remains contested. Educators worry about fragmentation without common standards, yet a rigid list may age quickly and stifle local adaptation.
Six Research Priorities the Field Must Tackle Next
The conference and survey surfaced six urgent areas for investigation, each directly informing curriculum renewal.1
- Digital literacy assessment design: How to measure entering students' baseline digital skills reliably and equitably.
- Nursing roles in digital healthcare: Conceptual models that define nurses' unique contributions in tech-enabled settings.
- Preparing for virtual care: Effective pedagogies for remote assessment, monitoring, and therapeutic communication.
- Adaptive and critical skills: Learning experiences that build troubleshooting, critical appraisal, and rapid learning habits.
- Structuring peer and patient education: Strategies to teach nurses how to educate patients and colleagues using digital tools.
- Sustaining academic-practice partnerships: Blueprints for ongoing collaboration between universities and clinical informatics leaders.
Turning Debate into Program Strength
These unresolved questions are not weaknesses. They are invitations for educators to shape the future. Programs that engage the debates locally, drawing on the nurse-led research in education tradition, build curricula that are responsive, context-aware, and anchored in real practice needs.
Your next step: Convene a small stakeholder group within your institution, including informatics leads, practice partners, and students, to discuss which debated area matters most in your setting. Use that conversation to set a 12-month inquiry agenda, whether that means piloting a digital literacy assessment or redesigning a virtual care module. The consensus gives you permission to explore, and the research priorities offer a ready-made roadmap.
Frequently Asked Questions
Related Articles
The path to digital-ready nursing graduates begins not with technology procurement, but with people. Your first move: this month, assess your faculty's specific digital capability gaps using a tool like the TIGER-based self-assessment mentioned earlier. Next semester, pilot a validated student entry-level digital literacy screen so you can baseline cohort readiness before clinical exposure. Within 90 days, initiate at least one formal academic-practice partnership by inviting an informatics leader to co-design a virtual care simulation or guest lecture.
These three actions embed the 2026 consensus's core message: adaptability and authentic partnerships move the needle, not static checklists. If you are ready to move from bedside to classroom, this is the moment to bring your clinical digital fluency into teaching. Start before the curriculum committee meets again.