What you’ll learn in this article…
- Apprenticeship students earn wages during clinical training, unlike unpaid traditional placements.
- Registered Apprenticeships offer federal funding; employer-based models allow hospitals to customize.
- Massachusetts launched state-funded nursing apprenticeship planning grants in 2026.
- Nurse educators now coordinate preceptors and embed paid clinical hours into academic courses.
With nursing vacancies reaching crisis levels across the country, some states report RN vacancy rates above 15%, and apprenticeship models have become a frontline tactic for rebuilding the workforce.
A nursing apprenticeship is an employer-sponsored, earn-and-learn pathway that combines paid clinical employment with a structured academic program, allowing students to graduate with reduced debt and substantial hands-on experience.
For nurse educators, this model demands a new kind of engagement: you must integrate apprenticeship competencies into existing curricula, synchronize work hours with academic calendars, and collaborate closely with employer preceptors. The result is a curriculum that treats the workplace as a formal extension of the classroom, not an adjunct. In the sections that follow, you will find a breakdown of the major apprenticeship models, guidance on curriculum integration, and state-level examples to help you evaluate whether this pathway fits your program.
What Are Nursing Apprenticeships and Why Do They Matter Now?
Healthcare employers and academic institutions alike are rethinking how the nursing workforce is trained, and apprenticeship models are moving from a niche experiment to a central strategy. They matter now because the traditional pipeline of clinical placements and academic schedules has struggled to meet both student demand and employer expectations for practice-ready graduates.
Defining a Nursing Apprenticeship
A nursing apprenticeship is a structured, paid, on-the-job training program that combines supervised clinical practice with classroom-based or online related instruction. Unlike an unpaid clinical rotation, apprentices are employees of a healthcare organization from day one and earn progressively higher wages as competencies are met. Programs typically follow a nationally recognized framework, such as the Registered Apprenticeship model approved by the U.S. Department of Labor, and they can target roles ranging from certified nursing assistant to registered nurse.
Apprentices work alongside a qualified preceptor and are expected to demonstrate mastery of specific skills before advancing. The instructional component is often delivered in partnership with a community college or university, ensuring alignment with licensure or certification requirements.
Why the Model Is Gaining Traction
Several converging factors drive interest in nursing apprenticeships. First, workforce projections point to sustained demand for registered nurses well into the next decade, with many states facing persistent vacancy rates and an aging workforce. Reports from federal health workforce agencies have repeatedly flagged shortages in both acute and long-term care settings, a reality closely tied to the broader nursing faculty shortage.
Second, clinical placement capacity has become a bottleneck. Schools routinely compete for limited slots in hospitals and clinics, and preceptor fatigue is a recognized problem. Apprenticeships formalize the employer's role as a training partner rather than a temporary host, creating a more reliable pipeline of new graduates who are already socialized into the organization.
Third, the economic model appeals to students who need income while in training and to employers who can fund positions through existing workforce development dollars instead of recruiting expensive travelers. For those wondering whether nurse educators are in high demand, the answer is a resounding yes, and apprenticeship programs only increase the need for qualified faculty who can bridge classroom theory and clinical reality.
Key Features and Variations
- Registered Apprenticeship: A federally endorsed model that requires a written training plan, progressive wage scales, and a portable credential upon completion. It is the most structured version and often qualifies for state and federal funding.
- Pre-licensure apprenticeship: Combines training hours required for an RN license with employment, allowing students to sit for the NCLEX upon completion while having accrued paid clinical hours that exceed standard program requirements.
- Employer-sponsored models: Some health systems design internal apprenticeships that align with their own culture and patient populations, sometimes in collaboration with a single academic partner.
Each variation places the nurse educator role at the intersection of curriculum design, competency assessment, and ongoing mentorship.
Nursing Apprenticeship vs. Traditional Clinical Placement
A nursing apprenticeship is an employment-based educational pathway where students earn a wage while completing supervised clinical training as part of their nursing program. In contrast, a traditional clinical placement is an unpaid, school-arranged rotation where students observe and practice under instructor guidance for a set number of hours. Both models aim to produce competent nurses, but they differ significantly in structure, student experience, and outcomes for the healthcare workforce.
Employment and Compensation Differences
The most visible distinction is financial. Apprenticeship students are employees of a healthcare facility, receiving hourly wages, benefits, and often tuition assistance. Traditional clinical placements are unpaid, and students typically bear the full cost of their education. This shifts the student's role from learner to contributing team member, fostering accountability and a stronger sense of belonging.
Clinical Hour Structure and Integration
Traditional clinicals are often scheduled in concentrated blocks (one or two days per week for a semester), which can leave gaps between classroom learning and application. Apprenticeships typically spread clinical hours across the entire program, allowing students to continuously integrate theory with practice. The extended timeline and consistent mentorship from experienced nurses build deeper clinical judgment in nursing and procedural skills.
Comparing Outcomes and Evidence
Rigorous, large-scale comparisons of NCLEX pass rates and first-year retention between apprenticeship and traditional graduates are still evolving. National nursing bodies and state boards are beginning to collect program-level data, but comprehensive published reports remain limited. Anecdotal evidence and smaller program evaluations suggest that apprenticeship graduates often transition to practice with greater confidence and may require shorter orientations, but these findings await broader validation. Educators seeking data can monitor updates from state boards, the NCSBN, and professional associations like the NLN. Understanding how changes like the next generation NCLEX affect assessment expectations will also be important as apprenticeship programs mature.
Implications for Nurse Educators
For nursing faculty, traditional placements offer a predictable, centrally managed training model. Apprenticeships require a more complex partnership between schools and employers, with faculty coordinating academic standards alongside workplace learning outcomes. While this demands additional administrative effort, it also opens opportunities for educators to directly shape practice-ready graduates and strengthen workforce pipelines. Faculty interested in developing the competencies this work requires can explore the qualities of a good nurse educator that support both models.
Key Apprenticeship Models: Registered, Pre-Licensure, and Employer-Based
When building or expanding nursing apprenticeship pathways, educators weigh two fundamental options: Department of Labor Registered Apprenticeships that bring federal oversight and funding, or employer-designed models that allow hospitals to tailor training to internal needs. Each carries distinct advantages, and many programs blend elements of both.
Registered Apprenticeships: A Federal Framework
Registered Apprenticeships (RAs) are formal, paid training programs recognized by the U.S. Department of Labor. They require a sponsor, which can be an employer, labor union, or educational institution. A key feature is the use of competency-based standards, ensuring apprentices master specific clinical and professional skills before advancing. Upon completion, participants earn a nationally portable credential, boosting career mobility. For nurse educators, RA designation signals that a program meets rigorous quality benchmarks, which can attract students seeking funded pathways. RAs also unlock federal resources: Workforce Innovation and Opportunity Act dollars, GI Bill benefits for veteran learners, and dedicated apprenticeship grants. Integrating an RA into a nursing curriculum demands alignment with the DOL's work process schedule, but the structure provides a clear roadmap for mapping classroom theory to real-world practice.
Pre-Licensure Apprenticeships: Stacking Credentials
Many nursing apprenticeships follow a pre-licensure model, where students begin as employed certified nursing assistants or patient care technicians while enrolled in an associate or bachelor's program. The apprenticeship provides supervised, compensated clinical experience that directly contributes to licensure requirements. As they progress, learners often achieve interim milestones, such as licensed practical nurse (LPN) status, before sitting for the NCLEX-RN. This progressive credential stacking reduces student debt, sharpens clinical judgment early, and creates a pipeline of practice-ready graduates who are already familiar with the employer's workflows. Educators overseeing these programs take on a coordinating role, ensuring that coursework objectives sync with on-the-job competencies. The model works especially well when nursing schools and healthcare employers share clinical educators in nursing and align practice assessments.
Employer-Based Models: Custom Hospital Pipelines
On the other side of the spectrum, employer-based apprenticeships operate outside the federal registered system. These are typically designed, funded, and managed by a hospital or health system, often in partnership with a single nursing school. Without DOL registration, the program enjoys flexibility: it can set its own length, wage progression, and skill checklists. An employer might, for instance, build a perioperative apprenticeship tailored to its operating room staffing gaps. However, the resulting credential is not nationally portable, and the program may need to cover its own costs without access to public apprenticeship grants. For educators, the primary involvement is in curriculum articulation: ensuring apprentices receive academic credit for their workplace learning and that the school's clinical requirements are satisfied. These models demand strong inter-institutional trust and clearly defined roles. Adopting innovative teaching strategies in nursing education can help bridge the gap between employer-specific training and academic standards.
Choosing the Right Model: A Quick Decision Framework
- Registered model: Prioritize this if you want federal funding eligibility, national credential portability, and standardized quality assurance. Best for schools seeking to expand access to under-resourced students or scale statewide.
- Employer-based model: Choose this when speed, customization, and deep alignment with a specific employer are paramount. Ideal for hospitals wanting to immediately address specialty shortages.
- Pre-licensure focus: Regardless of registration status, stacking credentials from CNA to RN works well in both frameworks. It requires careful competency mapping and strong clinical partnerships.
- Hybrid approach: Many programs begin as employer-based pilots and later pursue DOL registration once the curriculum and outcomes are documented.
This decision should be informed by local workforce data, partner readiness for administrative tasks, and the student population's needs. By understanding these models, educators can advocate for the apprenticeship structure that best serves their community and institution.
Questions to Ask Yourself
The Nurse Educator's Role in Apprenticeship Programs
Adopting an apprenticeship model promises deeper student development but also demands a fundamental shift in how you allocate your time as an educator. The personalized structure requires you to step beyond traditional classroom and clinical oversight into a role that blends curriculum design, preceptor coordination, and competency-based assessment. Understanding these core responsibilities, and their workload implications, helps you plan for a sustainable program that benefits both students and your institution.
Core Responsibilities of the Nurse Educator
Your role in an apprenticeship program centers on four interconnected duties:
- Curriculum alignment: Map apprenticeship experiences to program competencies and licensing requirements. This means translating broad educational outcomes into specific, observable skills that students can demonstrate on the job under the guidance of a clinical preceptor.
- Preceptor coordination: Identify, prepare, and support the clinical preceptors who will work directly with apprentice-students. Even if you do not supervise every hour, you remain responsible for ensuring preceptors understand the learning goals and assessment rubrics.
- Competency assessment: Develop and oversee milestone evaluations that verify student progress. Unlike traditional clinical rotations where a single faculty member observes a group, apprenticeship assessment often relies on preceptor feedback, portfolio reviews, and periodic site visits to confirm that standards are being met.
- Mentorship and advising: Serve as the consistent academic touchpoint for apprentice-students. They need help navigating the dual demands of employment and education, and your guidance on career progression and academic challenges becomes even more critical when the learning environment is so closely tied to a workplace.
How Apprenticeship Supervision Ratios Change Your Workload
Traditional clinical groups often place 8 to 10 students under one faculty supervisor. Apprenticeship models shift toward a preceptor-based structure with ratios closer to 1:1 or 1:2. While this dramatically improves the quality of bedside teaching, it multiplies the number of preceptors you must coordinate. Instead of managing five clinical groups, you might support twenty or more individual preceptor-student pairs. The workload therefore moves from direct student oversight to preceptor training, communication, and quality assurance. You will find yourself making more site visits, reviewing more competency checklists, and troubleshooting more interpersonal dynamics, all of which require dedicated time that must be carved out of other faculty responsibilities. If you want a clearer picture of what a nurse educator day looks like before layering on apprenticeship duties, that context can help you plan realistic time blocks.
The Educator-Preceptor Partnership Model
A successful apprenticeship depends on a clear division of labor between you and the clinical preceptor. You set the overarching learning outcomes, design the assessment rubrics, and determine the sequence of competencies. The preceptor provides daily, on-the-job instruction and role modeling. Overlap occurs in the feedback loop: you both need to communicate frequently about student progress, and you may need to coach a preceptor on how to evaluate a particular skill. However, you are not responsible for the preceptor's patient assignments or unit operations, and the preceptor typically does not modify the academic curriculum. Establishing this boundary early prevents role confusion and keeps the program running smoothly.
Managing the Administrative Load
Apprenticeship coordination adds a layer of administrative work that goes well beyond a typical teaching assignment. Site visits to multiple employers, documentation of competency attainment across dozens of students, and ongoing communication with human resources and unit managers all compound quickly. Institutions that underestimate this burden often see faculty burnout or program quality issues. Reviewing strategies for nurse educator burnout prevention is a practical first step before you take on these additional responsibilities. Effective planning includes building in release time for you or designating a dedicated apprenticeship coordinator role. Some programs use a team approach, spreading duties among several educators. The investment in administrative infrastructure pays off in a more consistent student experience and less stress for the educators who make the model work.
Surprisingly, few resources explain what nurse educators actually do in an apprenticeship. This article fills that gap with the first concrete job description for the role, outlining responsibilities from preceptor coordination to curriculum integration.
How to Integrate Apprenticeships Into Existing Nursing Curricula
Integrating an apprenticeship into a nursing curriculum means embedding paid, on-the-job training into a program's existing course sequence so students earn credits for their clinical work while meeting academic and regulatory standards. It's not about starting from scratch: it's about smart mapping and phased implementation.
Assess Where Apprenticeship Hours Fit in Your Clinical Course Sequence
Start by auditing every clinical course in your pre-licensure track. Identify which courses already deliver supervised direct patient care hours that align with the apprenticeship role. In many programs, the later semesters' clinical rotations map neatly onto apprenticeship positions in acute care or long-term care settings. For these courses, you can often designate the apprenticeship site as an approved clinical placement, provided the partner employer meets faculty supervision and evaluation criteria. Understanding what subjects nurse educators teach can help you pinpoint exactly where apprenticeship hours overlap with existing course objectives. Courses that don't naturally align may need a new clinical elective shell or a special topics designation to house the apprenticeship credits without disrupting the program's credit distribution. The goal is to avoid inflating total credit loads while giving apprenticeships a legitimate academic home.
Align Apprenticeship Milestones with QSEN Competencies and AACN Essentials
Both CCNE and ACEN currently allow apprenticeship clinical hours to count toward program requirements on a conditional, case-by-case basis, as long as the program retains authority over supervision, evaluation, and documentation.12 To meet those conditions, link every apprenticeship competency checkpoint to the Quality and Safety Education for Nurses (QSEN) competencies and the 2021 AACN Essentials. For example, an apprentice's progress in medication administration or patient education can be assessed using rubrics anchored in safety, evidence-based practice, and patient-centered care domains. Map each apprenticeship milestone to specific course objectives and student learning outcomes. This brings apprenticeship learning into the formal assessment structure, satisfying both accreditor expectations and Department of Labor apprenticeship standards.
Document Clinical Hours to Satisfy DOL and Accreditor Expectations
Documentation is the linchpin. Create a shared tracking system, often a digital log co-signed by the apprentice, preceptor, and faculty member, that records hours, skills performed, and competency demonstrations. The log should clearly indicate how many hours are applied to each course and distinguish between paid employment hours and academic clinical hours when necessary. Both ACEN and CCNE emphasize that the program must verify supervision and evaluation meet the same standards as traditional clinical placements.32 Keep a syllabus addendum for each course that incorporates apprenticeship hours, noting the clinical site, faculty role, and evaluation methods. This paper trail is essential for program reviews and accreditation site visits.
Start Small with a Phased Rollout
Trying to scale too quickly can fracture relationships with clinical partners and overwhelm faculty. Instead, pilot the apprenticeship model with one cohort at a single trusted clinical partner. Build the infrastructure for scheduling, competency tracking, and faculty liaison support during that first year. Collect data on NCLEX pass rates, retention, and preceptor feedback, then use those results to refine the documentation processes and competency assessments before expanding to additional sites or cohorts. If you want to build a research culture in nursing education, this pilot phase is also an ideal time to embed a small outcomes study into the rollout. This phased approach prevents over-promising before your systems are sturdy, and it gives your faculty and accreditors confidence that the model works.
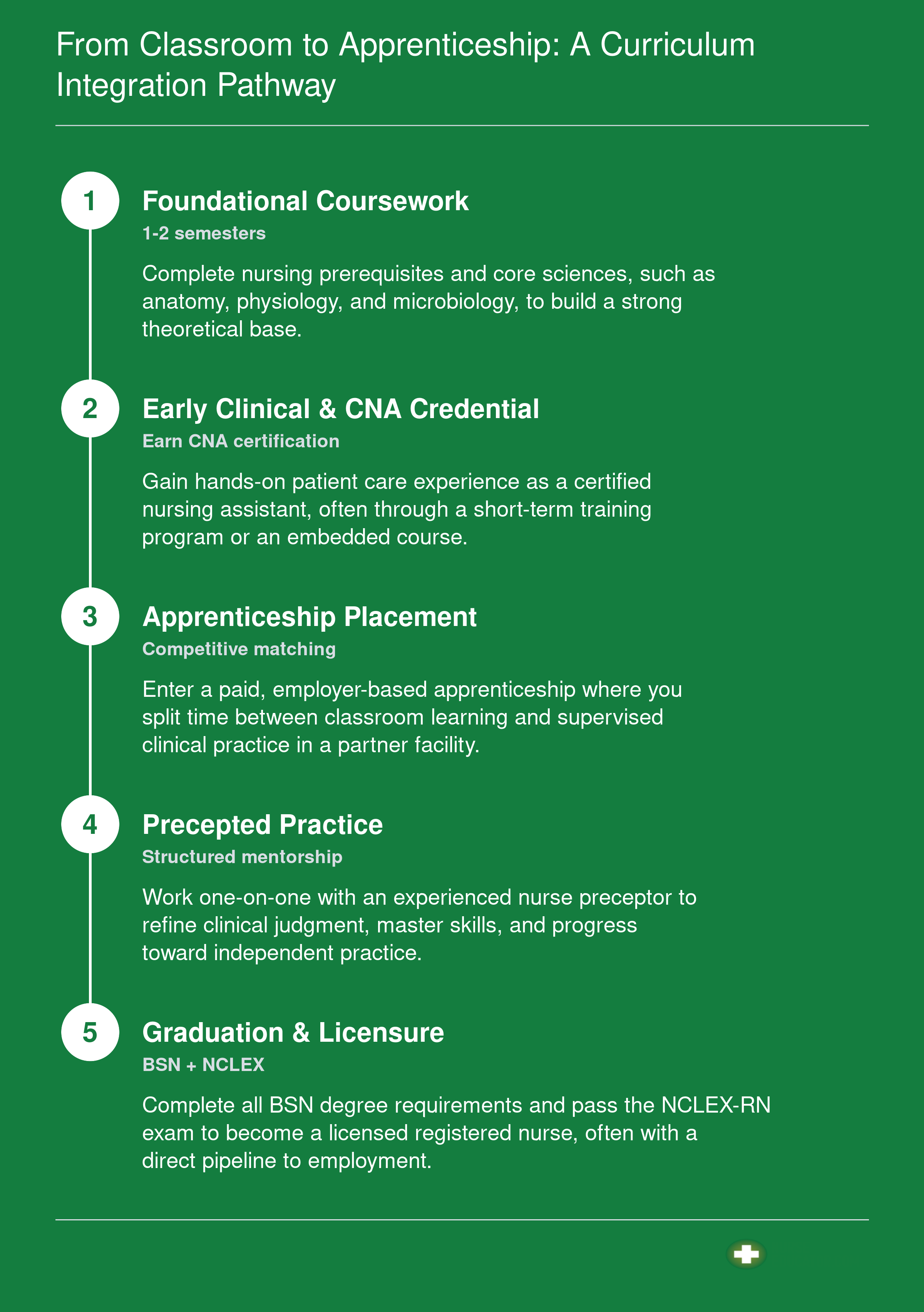
From Classroom to Apprenticeship: A Curriculum Integration Pathway
Nursing apprenticeships blend classroom education with paid, on-the-job training. Here’s how a traditional BSN program can incorporate an apprenticeship track from the first semester through licensure.
Accreditation, Regulation, and Legal Considerations
Do state boards of nursing recognize apprenticeship hours as clinical hours, and what happens if an apprentice makes a mistake? The answer determines whether programs can launch, so verifying your state's stance is step one. Accreditation and regulation for nursing apprenticeships sit at the intersection of nursing education standards and federal workforce rules. Nurse educators must navigate both, often without clear precedent.
State Board Approval: A Patchwork of Policies
Some state boards of nursing have explicitly approved apprenticeship clinical hours as counting toward licensure requirements, while others have not yet issued guidance. A few states have amended their nurse practice acts or issued declaratory rulings confirming that supervised apprenticeship hours fulfill clinical hour mandates. Many boards, however, still rely on traditional academic-clinical partnership models and may not have addressed apprenticeships directly. Educators should contact their state board early to request a written opinion or determine if a formal program approval process exists. Launching without clarity risks students completing hours that are later rejected for licensure eligibility. If you are evaluating programs across multiple states, reviewing the best states for nurse educator programs can help you identify which regulatory environments are most receptive to innovation.
Liability: Who Bears Responsibility?
When an apprentice makes a clinical error, the liability question can stall program development. Apprentices hold a dual status: they are employees of the healthcare facility and students enrolled in an academic program. The general legal framework places primary liability on the employer for employee actions under the doctrine of respondeat superior, but the educational institution may also carry exposure if it provides oversight or places the student in the setting. Many programs address this through indemnification agreements and shared risk provisions in affiliation contracts. Because legal precedent in nursing apprenticeships is limited, institutions must consult legal counsel to draft clear agreements defining each party's responsibility for supervision, training, and insurance coverage. Without a written framework, a clinical mistake could lead to costly disputes between the school and employer.
Scope of Practice: Credential Boundaries Are Non-Negotiable
Apprentices cannot perform tasks beyond their current credential level, even under preceptor supervision. For instance, a CNA-level apprentice must operate strictly within the certified nursing assistant scope; preceptors cannot delegate registered nurse tasks to them, even for learning purposes. This constraint often surprises educators accustomed to clinical placements where students may practice advanced skills under instructor license coverage. Understanding the difference between a nurse and a nurse educator helps clarify why supervision models differ so significantly between apprenticeship and traditional clinical settings. State nurse practice acts define scope, and violating these boundaries can expose both the apprentice and the supervising nurse to disciplinary action. Educators must ensure that apprenticeship learning plans map only to legally permitted activities and that preceptors are trained to recognize and enforce these limits.
Federal Registered Apprenticeship Requirements
If a program seeks status as a U.S. Department of Labor Registered Apprenticeship, it must meet additional compliance obligations. These include: - Written standards: A detailed training outline with competency milestones approved by DOL or a state apprenticeship agency. - Wage progression: Apprentices must receive scheduled pay increases as they gain skills. - Equal Employment Opportunity plan: A nondiscrimination and affirmative action plan for recruitment. - Reporting: Periodic submission of apprentice progress and program data.
These administrative duties fall partly on the educational partner, which must maintain records and coordinate with the employer sponsor. For nursing schools, this often means designating a staff member to manage DOL paperwork and updates, adding a layer of complexity beyond typical clinical coordination.
Related Articles
Funding and Cost Models for Nursing Apprenticeships
Funding and cost models for nursing apprenticeships describe where the money comes from to pay for apprentice wages, instruction, equipment, and program administration. This includes a mix of federal grants, state workforce dollars, employer investments, and sometimes union sponsorships. Educators who understand these financial structures can advocate for sustainable apprenticeship expansion in their institutions, ultimately helping address the ongoing nursing faculty shortage solutions.
Federal Grant Programs
Federal agencies offer competitive grants that can offset start-up and operational costs for nursing apprenticeships.
- Registered Apprenticeship grants: The U.S. Department of Labor periodically opens competitive grant cycles specifically for healthcare apprenticeships. These can fund program development, equipment, and support services for apprentices.
- HRSA Title VIII: The Health Resources and Services Administration supports nursing workforce development through programs that may fund clinical training innovations aligned with apprenticeship structures.
State and Regional Workforce Boards
State apprenticeship agencies and workforce boards often allocate funds for high-demand sectors like nursing.
- State agency programs: Many states have dedicated apprenticeship expansion funds. Visit your state workforce board's website for current requests for proposals.
- WIOA funds: Workforce Innovation and Opportunity Act dollars can sometimes be used for apprenticeship-related instruction or supportive services.
Employer-Led Cost Models
Many nursing apprenticeships are employer-sponsored, with healthcare facilities covering the bulk of training costs in exchange for a service commitment.
- Wage support: Employers typically pay apprentices for on-the-job training hours, with rates often increasing as skills are mastered.
- Tuition assistance: Some employers cover or reimburse tuition for the related classroom instruction, often in return for a multi-year work commitment.
Association and Advocacy Resources
Professional nursing organizations compile funding information and advocate for policies that support apprenticeship growth. Educators exploring careers in nurse education will find that many of these groups also connect faculty with funding opportunities tied to innovative training models.
- Policy guidance: Groups like the American Nurses Association and the National League for Nursing track legislation affecting apprenticeship funding and provide advocacy toolkits.
- Model sharing: These organizations frequently highlight successful programs, which can help educators craft grant proposals and connect with potential funders.
By tapping into these diverse funding streams, nurse educators can help design apprenticeship programs that are financially viable for students, employers, and schools alike.
State-Level Examples and National Trends
Nursing apprenticeships are gaining traction across the country, with several states launching coordinated initiatives that others can adapt.
Massachusetts Leads with Planning Grants
In 2026, Massachusetts made a significant commitment to nursing apprenticeships through its Nursing Apprenticeship Planning Grants, administered with the Nursing Council on Workforce Sustainability (NCWS) based at UMass Medical School.1 The state allocated a total of $240,000, with individual awards ranging from $30,000 to $60,000.2 Applications were due on March 6, 2026, following a webinar held on February 17.3 Eligible entities include healthcare employers and public higher education institutions, fostering direct collaboration between clinical sites and academic programs.1 These grants support the development of registered apprenticeship programs that lead to LPN or RN credentials. While Quinsigamond Community College is exploring an LPN apprenticeship, the program is not yet in place, indicating that most efforts remain in the planning or early implementation stage.4 Educators interested in similar initiatives can contact the NCWS at [email protected] for guidance.
Other State Models: Minnesota, Missouri, and Texas
Several other states have launched nursing apprenticeship programs, though details vary widely. In Minnesota, Missouri, and Texas, sponsoring organizations often include state hospital associations or Departments of Labor. For the most current information, visiting each state's Department of Labor website or major healthcare association portals is recommended, as program designs and cohort sizes can shift quickly based on local workforce needs and employer engagement. These models frequently involve partnership agreements between community colleges, university nursing programs, and hospital systems, with shared responsibility for on-the-job training and academic instruction.
National Trends and the Data Picture
Nationally, registered apprenticeships in healthcare are expanding, fueled by nursing workforce shortages. Data from the Bureau of Labor Statistics continues to project strong demand for nurses, but apprenticeship-specific outcomes, such as completion rates, credential attainment, and long-term earnings, are still being compiled and are not yet broadly published. Early anecdotal evidence suggests improved retention and readiness, but educators should treat current benchmarks as preliminary. Professional organizations, including the American Association of Colleges of Nursing (AACN) and the American Nurses Association (ANA), offer periodic reports on program design and cohort size benchmarks. What is clear is the growing federal recognition of nursing apprenticeships as a legitimate pathway, with more states adopting registered models that blend classroom and clinical work.
What Educators Can Learn from These Programs
For nurse educators, these state-level experiments offer a roadmap. Key takeaways include the value of employer-academic partnerships, the need for flexible curricula that accommodate apprentices' work hours, and the importance of early engagement with state workforce councils. If you are building your own nursing education curriculum, studying these pilot structures can help you design programs that align with apprenticeship standards. Monitoring pilot results from Massachusetts and other states can help inform new program proposals, while existing grant opportunities may provide funding to support design and startup costs. As data matures, these early adopters will shape national best practices.
Questions to Ask Yourself
Common Questions About Nursing Apprenticeships for Educators
As nursing apprenticeships gain traction, educators often have pressing questions about their design and implementation. The following answers draw from the program models, funding options, and curriculum strategies discussed throughout this guide.