What you’ll learn in this article…
- ESL nursing students need five to seven years to develop academic language proficiency.
- Structured NCLEX prep should target linguistic test patterns before clinical content.
- Institutional ESL support models outperform individual faculty efforts long term.
In many associate degree nursing programs, ESL students now make up over 20% of each cohort, but their completion rates lag 15 to 20 percentage points behind native English speakers. Christina Granato's doctoral research at St. John Fisher University examined exactly why: the barriers are linguistic and institutional, not academic.1
That finding reframes the problem for nurse educators. The gap reflects mismatches in how we teach, test, and communicate nursing content, not any deficit in clinical reasoning. Your ESL students can master the material; they need you to make the language of nursing transparent without lowering academic standards.
Closing that gap demands concrete strategies: scaffolding medical vocabulary, redesigning clinical simulations so they assess communication rather than language proficiency, and investing in nursing faculty development that makes these shifts stick across an entire program.
Common Challenges ESL Nursing Students Face
ESL nursing students bring dedication and diverse clinical perspectives to their programs, yet they navigate a set of obstacles that many of their native-English-speaking peers never encounter. Understanding these challenges is the first step toward creating classrooms where every student can succeed.
Language proficiency is the most visible hurdle. Medical terminology is demanding for any learner, but for students whose primary language is not English, absorbing and retaining thousands of clinical terms while simultaneously processing instruction in a second language creates significant cognitive load. Reading comprehension on timed NCLEX-style questions, interpreting complex care plans, and writing detailed nursing notes all require a precision of language that takes time to develop.
Verbal communication in clinical settings adds another layer of difficulty. ESL students must speak clearly with patients, respond quickly to supervising nurses, and participate in handoff reports, often in high-pressure environments where hesitation can be misread as incompetence. Accent differences and code-switching between a home language and clinical English can erode a student's confidence even when their clinical knowledge is strong.
Cultural adjustment compounds these pressures. Many ESL nursing students come from educational traditions where questioning an instructor or admitting uncertainty is considered disrespectful. When faculty in U.S. programs expect students to advocate for themselves, ask clarifying questions, and engage critically with course material, students from those backgrounds may appear disengaged when they are actually deferring out of respect.
Time management and test-taking strategies present additional barriers. ESL students often need more time to process exam questions written in idiomatic English, and many standardized testing formats assume cultural familiarity that international or immigrant students simply do not share. Outside the classroom, students may be juggling family caregiving responsibilities, jobs, and limited access to academic support services, all of which narrow the time available for study.
Research by Christina Granato, Ed.D., FNP, MS, RN, retired dean at Onondaga Community College, focused specifically on these barriers among ESL students in associate degree nursing programs. Her doctoral work identified persistence factors that help students push through these challenges, providing nurse educators with an evidence-based framework for supporting nursing students at risk of dropping out.1 Recognizing which barriers are most prevalent in your own program is the foundation for any meaningful intervention.
Classroom Language Support Strategies for ESL Nursing Students
Surface-level conversational fluency versus deep academic language proficiency: the difference between these two levels of English mastery determines whether your ESL nursing students can chat comfortably at lunch or actually decode a pathophysiology lecture. Understanding that distinction is the starting point for building effective classroom support.
Why CALP Matters More Than Conversational English
Linguist Jim Cummins drew a critical line between Basic Interpersonal Communication Skills (BICS) and Cognitive Academic Language Proficiency (CALP). BICS is the everyday conversational English a student may pick up in one to three years. CALP, by contrast, is the ability to process abstract, context-reduced academic language, and it can take five to seven years to develop fully. In nursing, CALP is what allows a student to interpret a case study prompt, parse an NCLEX-style question stem, or synthesize information from a pharmacology textbook. A student who speaks English fluently in the hallway may still struggle with the dense, jargon-heavy language of nursing coursework. When you share this framework with colleagues, it reframes the conversation: the challenge is not that a student "doesn't know English" but that academic language proficiency requires deliberate, sustained support.
Nursing-Specific Vocabulary Building
Medical terminology is built on Latin and Greek roots, and teaching those roots explicitly gives ESL students a decoding tool they can use across every course. Pre-teach common prefixes (hypo-, hyper-, tachy-, brady-) and suffixes (-emia, -itis, -ectomy, -osis) at the start of each unit so students can break unfamiliar terms into recognizable parts. Pair this with unit-specific glossaries that define terms in plain English alongside clinical definitions. Visual aids, such as labeled anatomical diagrams and medication mechanism-of-action charts, reinforce vocabulary through multiple channels. When students see, read, and label terms simultaneously, retention improves.
UDL-Aligned Classroom Techniques
Universal Design for Learning principles benefit every student but are especially powerful for ESL learners. Consider integrating these innovative teaching strategies in nursing education:
- Skeletal outlines: Distribute partially completed lecture outlines before class so students can follow the structure and fill in details rather than scrambling to capture everything from scratch.
- Concept mapping: Use visual maps to connect pathophysiology concepts, helping students see relationships between terms instead of memorizing isolated definitions.
- Think-pair-share: Give students time to formulate thoughts individually, discuss with a partner, and then share with the larger group. This scaffolded approach reduces the pressure of spontaneous oral responses.
- Recorded lectures: Make recordings available for replay so students can revisit complex content at their own pace, pausing to look up unfamiliar terms.
Active Learning That Reduces Language Burden
Not every assessment of clinical reasoning needs to hinge on spontaneous verbal fluency. Simulation labs allow ESL students to demonstrate competence through action, applying skills in a controlled environment where the emphasis is on safe practice rather than polished English. Role-play scenarios let students rehearse patient interactions with a script or outline before performing them independently. Collaborative case studies are another strong option: small groups can work through clinical problems together, and you can assess each student's reasoning through written contributions or structured worksheets rather than relying solely on who speaks up first. These active learning strategies in nursing do not lower the academic bar. They widen the path so students can show what they know without language being the sole gatekeeper.
Questions to Ask Yourself
Teaching Clinical Communication to ESL Nursing Students
The gap between understanding clinical concepts and communicating them confidently at the bedside represents one of the steepest learning curves for ESL nursing students. Language proficiency alone does not guarantee effective clinical communication, because healthcare settings demand specialized pragmatic skills, rapid information exchange, and culturally nuanced interactions that standard English courses rarely address. Nurse educators who treat communication as both a clinical competency and a language competency1 create pathways for ESL students to succeed in high-stakes environments.
Using SBAR as a Structured Communication Framework
SBAR (Situation, Background, Assessment, Recommendation) offers ESL learners a predictable linguistic template that reduces cognitive load during stressful moments. Rather than searching for words while also processing clinical data, students can rely on a consistent structure that signals what information comes next.
A sample script for an ESL learner calling about a deteriorating patient might look like this:
- Situation: "This is Maria, the RN caring for Mr. Johnson in room 412. I am calling because his blood pressure has dropped to 82 over 54."
- Background: "He was admitted yesterday for pneumonia. He has a history of heart failure and diabetes."
- Assessment: "I am concerned he may be septic. His temperature is 38.9 and he appears confused."
- Recommendation: "I would like you to come evaluate him. Would you consider ordering blood cultures and a lactate level?"
Recommended SBAR training components for ESL students include language-aware orientation sessions, scripted rehearsal with peers, structured simulations, focused debriefing that addresses both clinical reasoning and language use, and progressive complexity as students build confidence.2
Bedside Communication Strategies
At the bedside, scripted patient education phrases give ESL students reliable language for common interactions. Phrases like "I am going to check your vital signs now" or "Please let me know if you feel any pain" provide starting points that students can adapt as their fluency grows.
Teach-back methods work particularly well when adapted for ESL learners. Instead of asking "Do you understand?" (which often yields a reflexive "yes"), prompt patients to explain what they heard: "Can you tell me in your own words how you will take this medication at home?" This technique helps ESL students verify comprehension while practicing active listening.
For delivering sensitive information, such as unexpected test results or end-of-life discussions, simulation offers low-stakes rehearsal. Research identifies participatory curriculum design, role-plays with commercial teaching videos, and systematic teaching of pragmatic skills as effective elements in communication programs.2 Video recording and playback allow students to observe their own tone, pacing, and body language, building self-awareness that written feedback cannot replicate.
Simulation-Based Training Protocols
Simulation combined with structured courses or workshops emerges as the most effective format for improving patient-centered communication, according to systematic reviews of 19 studies that found significant improvement in 13 of them.3 Common modalities include standardized patients, role-playing, and high-fidelity manikins.
For ESL students specifically, simulations should rehearse complex interactions like handoff reports, SBAR telephone calls, and conflict situations with family members.1 A notice-understand-practice cycle helps students first observe expert communication, then analyze why certain phrases work, and finally practice in progressively realistic scenarios.2 Some programs incorporate accent modification work with speech-language pathology support, typically spanning 8 to 12 weeks, with targeted focus on intelligibility for clinical phrases, numbers, and medication names.1
Interprofessional Team Communication
Rapid-fire interdisciplinary rounds, telephone orders, and assertive communication with physicians require preparation that goes beyond language mechanics. ESL students often hesitate to speak up not because they lack clinical knowledge, but because they need extra processing time or feel uncertain about professional norms.
Role-playing scenarios that mimic real rounds help students practice concise contributions under time pressure. Teaching assertive communication scripts, such as "I need to share a concern about this patient" or "I want to clarify the order before I administer it," gives students language they can deploy when advocating for patient safety. Clinical judgment in nursing develops alongside these communication skills, and educators who integrate both dimensions help ESL students perform more confidently during rounds.
Practical Tips for Clinical Preceptors
Preceptors play a critical role in ESL student success. Simple adjustments make a significant difference:
- Speak at a measured pace: Slow down slightly without being patronizing, and avoid idioms or slang that may not translate.
- Confirm understanding thoughtfully: Ask students to summarize rather than simply nodding along. "Walk me through what you will do next" reveals comprehension more accurately than "Does that make sense?"
- Distinguish hesitation from uncertainty: A pause before speaking may reflect language processing rather than clinical doubt. Give students a moment before jumping in, and ask clarifying questions when unsure whether the hesitation is linguistic or clinical.
A four-hour pre-placement workshop, as used in the Finding a Voice program, can orient preceptors to these strategies while giving ESL students a chance to practice key interactions before entering clinical sites.2
Related Articles
Assessment and Testing Accommodations for ESL Nursing Students
Assessment accommodations for ESL nursing students are formal adjustments to how a test is delivered or scored so the exam measures nursing knowledge rather than English fluency. In practice, that means things like extra time on written exams, use of an approved bilingual glossary of non-clinical terms, or rewording of convoluted question stems so a student who understands cardiac physiology is not tripped up by an idiom about "putting the cart before the horse."
Separating Language Skill from Clinical Knowledge
The central question in every accommodation decision is whether the item is testing what it claims to test. A question meant to assess prioritization in a post-op patient should not fail a student because the stem uses unfamiliar colloquial phrasing. When you build or review test items, scan for cultural references, double negatives, and low-frequency English words that carry no clinical weight. Keep the clinical vocabulary intact (patients and NCLEX will not simplify "auscultate" or "orthostatic"), but strip out linguistic noise that has nothing to do with nursing judgment.
Where to Ground Your Policies
Before designing accommodations on your own, look at what is already documented:
- Your institution's policies: Most nursing programs publish accommodation procedures through the disability services or accessibility office. Review these alongside your program handbook so faculty apply them consistently.
- Professional organizations: Frameworks from groups like the American Association of Colleges of Nursing (AACN) and the National League for Nursing (NLN) offer guidance on equitable and valid assessment design.
- State boards and NCLEX policy: State boards of nursing and the NCSBN publish rules on what accommodations are permitted for the licensure exam. Aligning classroom accommodations with Next Generation NCLEX policies prevents a mismatch at the finish line.
- The literature: CINAHL and PubMed searches using terms like "ESL nursing assessment validity" or "test accommodations language barriers" surface studies on rubric design and whether specific accommodations preserve rigor.
Practical Rubric and Delivery Choices
For written work and case analyses, use analytic rubrics that score clinical judgment in nursing separately from grammar and mechanics. That way an ESL student's clinical thinking is visible even when their prose is still developing. For oral exams and simulation debriefs, allow brief pauses for word retrieval and evaluate the accuracy of the assessment or intervention, not accent or fluency.
NCLEX Preparation Strategies for ESL Nursing Students
Traditional NCLEX review courses assume native English fluency. ESL-specific preparation programs address the linguistic architecture of test items before tackling clinical content.
Why NCLEX Language Challenges ESL Test-Takers
NCLEX questions use linguistic structures that amplify difficulty for non-native speakers beyond clinical knowledge gaps. Double negatives appear frequently (e.g. "Which action would NOT be inappropriate?"), forcing ESL students to parse layers of negation before analyzing the clinical scenario. Priority-ranking language such as "which action should the nurse take FIRST" or "what is the MOST important" requires students to distinguish subtle qualifiers that native speakers process automatically. Distractor options often share similar phrasing or root words, creating cognitive load when students must differentiate between "assess," "reassess," "continue to assess," and "notify the provider to assess."
The Next Generation NCLEX changes for nurse educators, launched in 2023, introduced case studies, matrix grids, extended multiple response, cloze drop-down, bow-tie, and drag-and-drop item types.2 Research from 2023 shows native English speakers averaged 90 to 98 seconds per Next Generation item.3 ESL students typically need additional processing time for these complex formats, which layer clinical decision-making onto multi-step reading tasks.
Analysis by the National Council of State Boards of Nursing found that 82 to 83 percent of NCLEX items showed no differential difficulty between ESL and native English speakers.1 However, 8 to 9 percent of items favored native speakers, while a comparable 8 to 9 percent favored ESL students, suggesting that question construction and linguistic features can unpredictably shift difficulty.1
A Phased Preparation Framework
Effective ESL-focused NCLEX preparation follows a structured progression rather than jumping directly into practice exams. Begin with vocabulary-building around NCLEX-specific terms: pharmacology prefixes and suffixes, priority verbs (initiate, implement, evaluate), and assessment descriptors (pallor, diaphoresis, dyspnea). Create glossaries that include pronunciation guides and sample sentences.
Move to question deconstruction exercises. Teach students to identify the "ask" in each stem by circling the actual question and underlining qualifiers (first, most, initial, priority). Practice rephrasing complex stems into simple declarative statements. Demonstrate elimination strategies: cross out options that answer a different question than the one asked, identify "absolutes" (always, never, all, only) that rarely reflect nursing practice, and flag distractors that repeat stem language without addressing the clinical need.
Only after students demonstrate deconstruction skills should you introduce timed practice under exam conditions. Simulate Next Generation NCLEX item types using case study formats that require students to navigate multi-step clinical scenarios. Language-focused instruction and explicit teaching of test language structure are recommended strategies,4 along with deliberate simulation of new item formats.2
Addressing American Healthcare Idioms
NCLEX items include colloquial healthcare language that ESL students may never encounter in textbooks. Phrases such as "the client voices concerns," "the nurse should advocate for," or "implement fall precautions" carry specific professional meanings. Create idiom reference sheets and integrate these phrases into classroom discussions and clinical post-conferences so students internalize the language before seeing it on high-stakes exams.
While comprehensive pass-rate data specific to ESL versus native English-speaking graduates is not widely published across all programs, targeted ESL preparation strategies that address linguistic complexity alongside clinical content have shown promise in narrowing performance gaps. Programs that boost NCLEX pass rates often embed language instruction throughout review courses, reporting improved confidence and first-attempt pass rates among ESL cohorts.
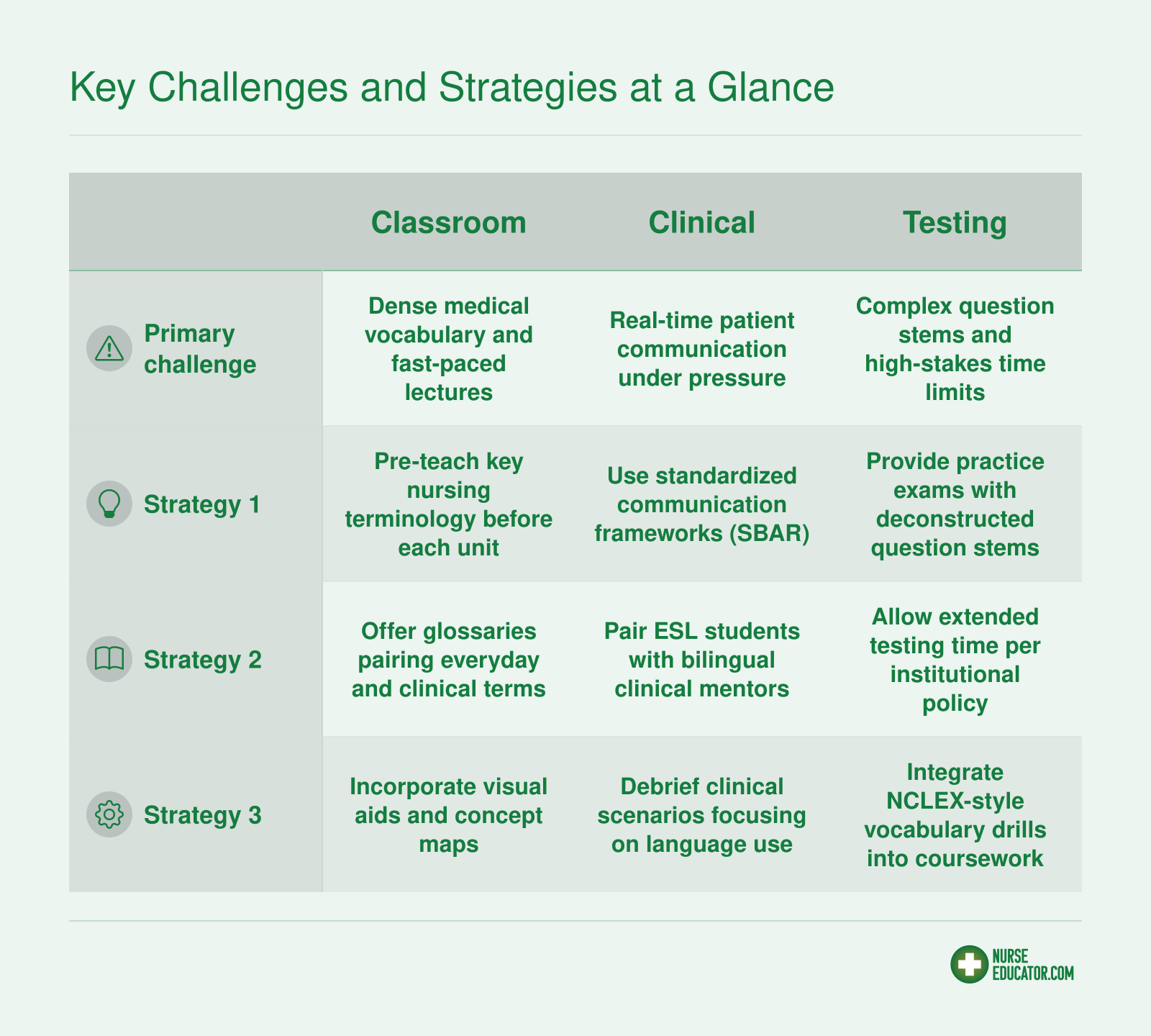
Key Challenges and Strategies at a Glance
ESL nursing students face distinct hurdles across three core areas of their education. This quick-reference summary pairs each challenge area with practical strategies you can implement right away. For deeper guidance on any column, see the dedicated sections above and below.
Building Cultural Competence as a Nurse Educator
Balancing standardized nursing competencies with the cultural realities your students bring to class is one of the toughest parts of teaching diverse cohorts. You want every graduate to meet the same high bar, yet you know that a one-size-fits-all approach can inadvertently exclude learners who communicate, relate, or prioritize differently. Building cultural competence as a nurse educator isn't about memorizing lists of cultural traits; it's about developing a mindset that continuously adapts to your students while keeping patient safety central.
Cultural Humility vs. Cultural Competence
Cultural competence suggests a destination, a point at which you know enough about other cultures to be effective. Cultural humility, by contrast, is an ongoing process of self-reflection, curiosity, and respectful partnership. In the ESL nursing classroom, that means acknowledging that you will never fully understand every student's lived experience, but you commit to learning alongside them. Practice both: build a foundation of knowledge about common health beliefs and communication patterns, then layer on humility by checking your interpretations and inviting student input. For example, instead of assuming why a student hesitates during a skills check-off, ask open-ended questions about how they learned similar tasks in their home country.
Recognizing Implicit Bias
Assumptions about accent, formality, or nonverbal cues can lead you to underestimate the clinical judgment of ESL students. You might interpret a soft-spoken student as lacking confidence, when in their culture, direct eye contact with an authority figure is considered disrespectful. Or you might misread a student's formal, memorized-sounding responses as a lack of understanding, when they are actually working hard to translate complex concepts under pressure. The first step is to notice these automatic reactions. Then, deliberately separate language proficiency from clinical reasoning. Use structured observation tools that evaluate skills objectively, and solicit self-reflections from students about how their cultural background shapes their communication style. This helps you see ability where bias might have hidden it. Educators who commit to this kind of reflective practice are demonstrating the qualities of a good nurse educator that make a lasting difference for students from all backgrounds.
Students' Cultural Backgrounds as Teaching Assets
Multilingual nursing students bring tremendous value to patient care. They often serve as informal interpreters, bridge cultural gaps in health teaching, and pick up on subtle cues that monolingual providers miss. In your classroom, invite ESL students to share healthcare practices from their home countries during relevant lessons. A student from a community that relies heavily on herbal remedies, for instance, can help the class understand why a patient might combine prescribed medication with traditional treatments. This not only validates the student's background but equips the entire cohort with cross-cultural health perspectives that no textbook can deliver. It also positions ESL learners as experts, boosting their confidence and engagement. Strategies like these connect directly to the broader work of addressing healthcare disparities as nurse educators by promoting equity inside the classroom before students ever enter clinical settings.
Practical Steps to Build Inclusion
- Attend workshops: Seek out cultural humility training designed for health professions educators. Even a single session can surface blind spots and offer new facilitation techniques.
- Invite sharing: Create low-stakes opportunities for ESL students to present on a health belief or practice from their culture, tying it to a course objective. This normalizes diversity as a learning resource.
- Audit your syllabus: Review readings, case studies, and examples to ensure they reference global nursing contexts, not just Western models. Include authors from varied backgrounds and scenarios that reflect your student body.
- Partner with ESL resources: Collaborate with campus language support services to design inclusive assignments and assessments that accurately measure content knowledge, not just language fluency.
These moves shift the classroom from a place where ESL students must constantly adapt to a space where all students grow by learning from one another.
Christina Granato (Ed.D., FNP, MS, RN) built her expertise from the ground up, starting as a critical care cardiac nurse, advancing to Family Nurse Practitioner, and eventually serving as Dean for Health and Community Services at Onondaga Community College. Her doctoral research at St. John Fisher University zeroed in on the specific barriers and persistence factors affecting ESL students in associate degree nursing programs, turning lived institutional experience into evidence-based action. Her career offers a concrete model that other nurse educators can study and adapt.
Faculty Development and Institutional Support Models
Individual effort versus institutional investment: that tension defines how successfully nursing programs support ESL students. A single committed educator can move the needle, but durable change happens when departments build structures that outlast any one person's tenure. The good news is that both paths are available to you, and they reinforce each other.
A Competency Framework for Nurse Educators
Effective support for ESL nursing students starts with educators who have developed a specific set of competencies. Think of these as five interlocking skills:
- Linguistic awareness: Recognizing how academic and clinical English creates barriers, and knowing how to reduce unnecessary complexity without lowering rigor.
- Assessment literacy: Designing tests and clinical evaluations that measure nursing knowledge rather than English proficiency alone.
- Clinical mentoring skills: Coaching students through the real-time, high-stakes communication demands of patient care settings.
- Cultural humility: Approaching each student's background as an asset rather than a deficit, and staying curious about your own assumptions.
- Resource navigation: Knowing what support services exist on campus and how to connect students to them without stigma.
Few faculty arrive with all five already developed. Building them is an ongoing process, not a one-time training event.
What Institutional Support Actually Looks Like
Programs that retain ESL nursing students tend to share a few structural features. Formal partnerships with campus writing centers and tutoring services make a measurable difference, especially when nursing faculty communicate directly with tutors about course-specific vocabulary and high-stakes assignments. Nursing faculty retention strategies like faculty learning communities, where instructors meet regularly to share what is and is not working for linguistically diverse cohorts, normalize the conversation and distribute expertise across a department. Mentorship pairing programs, matching ESL students with bilingual upper-level peers or recent graduates, address the social isolation that compounds academic stress.
Christina Granato's doctoral research at St. John Fisher University illustrates why these structures matter. Using semi-structured interviews in a qualitative phenomenological study with eight ESL nursing students in associate degree programs across Central New York, she identified language and cultural barriers, discrimination, financial strain, and time constraints as the primary obstacles students faced.1 What kept students enrolled was equally instructive: a strong motivation to care for others, clear goal orientation, and the desire for a better life.1 Peer support groups emerged as a key recommendation, and the research informed the ESL persistence strategies Granato developed during her tenure as Dean of Health and Community Services at Onondaga Community College.2
Starting Without Top-Down Support
You do not need a formal institutional mandate to begin. A single nurse educator can take concrete steps right now:
- Propose a small pilot: a six-week peer mentoring cohort, a vocabulary workshop series, or a standing consultation with the campus writing center.
- Document outcomes from the start, even informally. Completion rates, NCLEX pass rates, and student feedback give you evidence to take to administration.
- Connect with colleagues who share the concern and form an informal faculty learning community. A monthly lunch conversation counts.
- Frame the ask in terms leadership responds to: retention, accreditation standards, and workforce pipeline.
Granato's career, from critical care nursing through doctoral research to academic leadership, demonstrates how clinical insight and scholarly rigor can combine to reshape how programs serve vulnerable student populations. Her path is a reminder that the most effective advocacy often starts with one educator who decides the status quo is not good enough.
Nurse Educator Salary Overview
Understanding compensation is an important part of planning your career in nursing education. The figures below reflect 2024 data from the U.S. Bureau of Labor Statistics for Nursing Instructors and Teachers, Postsecondary. As nursing programs across the country work to serve increasingly diverse student populations, educators who develop specialized skills (such as ESL teaching strategies) bring added value to their institutions, a differentiator that can strengthen both career satisfaction and professional positioning in a growing field.
| State | Median Salary | 25th Percentile | 75th Percentile | Mean Salary | Estimated Employment |
|---|---|---|---|---|---|
| District of Columbia | $103,780 | $85,070 | $122,260 | $107,570 | 130 |
| Hawaii | $102,180 | $82,380 | $109,370 | $97,820 | 370 |
| California | $99,010 | $65,510 | $124,290 | $101,770 | 6,120 |
| Texas | $97,610 | $73,670 | $123,360 | $104,640 | 5,940 |
| New York | $93,640 | $63,540 | $128,930 | $99,170 | 5,380 |
| Alaska | $92,050 | $82,800 | $105,590 | $94,990 | 190 |
| Nevada | $84,660 | $63,070 | $97,040 | $86,640 | 920 |
| Montana | $84,550 | $66,280 | $105,390 | $85,630 | 230 |
| Florida | $83,940 | $66,100 | $104,120 | $88,970 | 4,990 |
| Delaware | $83,420 | $65,190 | $106,410 | $89,730 | 250 |
| North Dakota | $83,130 | $64,360 | $102,080 | $83,460 | 120 |
| Connecticut | $81,490 | $63,780 | $101,600 | $93,090 | 1,160 |
| New Hampshire | $81,260 | $65,850 | $83,790 | $80,760 | 530 |
| Maryland | $80,990 | $64,780 | $103,350 | $85,580 | 860 |
| Michigan | $80,740 | $60,640 | $101,450 | $83,140 | 1,680 |
| Colorado | $80,440 | $63,330 | $103,140 | $84,730 | 1,160 |
| Massachusetts | $80,140 | $72,920 | $102,140 | $90,830 | 2,860 |
| Pennsylvania | $79,920 | $59,330 | $98,430 | $82,980 | 4,860 |
| South Carolina | $79,900 | $62,920 | $95,750 | $85,470 | 1,150 |
| Wisconsin | $79,810 | $51,930 | $94,090 | $79,410 | 1,620 |
Frequently Asked Questions About Teaching ESL Nursing Students
These questions come up frequently among nurse educators working with linguistically diverse student populations. Each answer provides a concise overview, and you will find deeper discussion in the corresponding sections of this guide.