What you’ll learn in this article…
- Curriculum mapping to the eight NCLEX test plan categories raises first-time pass rates.
- Early warning systems can flag at-risk students two semesters before graduation.
- Faculty development in clinical judgment teaching directly improves program outcomes.
When a nursing program's first-time NCLEX pass rate falls below 80%, accreditation bodies take notice, and so do prospective students, who increasingly consult public scorecards before committing to a school. Since the 2023 launch of the Next Gen NCLEX, national pass rates have shifted; in 2025, first-time U.S.-educated candidates passed at 86.7%, while repeat test-takers managed just 52.7%. Tools like the NCLEX pass rate scorecard for nursing programs let educators benchmark their outcomes against national and state averages, compare BSN and ADN results, and identify schools that have improved most.
Responding effectively demands more than a last-minute review course. It requires a systematic approach that tightens curriculum alignment, sharpens clinical judgment instruction, and builds early-warning triggers for at-risk students.
Current NCLEX Pass Rate Trends: What Nurse Educators Need to Know
The national first-time NCLEX-RN pass rate for U.S.-educated candidates stood at 86.7% in 2025, with repeat takers passing at a considerably lower 52.7%.1 Early 2026 figures point to an overall pass rate of 72.3% across all candidate types in the first quarter1, a number that reflects the continued recalibration happening across nursing programs nationwide.
These figures are not just statistics to report to accreditors. They are a direct signal of how well your curriculum, clinical preparation, and student support systems are working.
The Next Gen NCLEX Transition and Its Ripple Effects
When the Next Generation NCLEX for nurse educators launched in April 2023, programs that had spent years optimizing for the previous exam format saw an almost immediate disruption. First-time pass rates dipped noticeably in the months following the transition, reflecting the exam's heavier emphasis on clinical judgment rather than discrete knowledge recall. By 2024 and into 2025, many programs began showing recovery trajectories as faculties retooled their teaching approaches and students became more familiar with the new item types, including extended multiple response, bow-tie, and trend questions.
If your program has not yet done a full audit of how your instruction aligns with the NCLEX Clinical Judgment Measurement Model, the 2026 data makes a compelling case for prioritizing that work now.
BSN vs. ADN Pass Rates: What the Gap Tells You
Historically, BSN graduates have outperformed ADN graduates on the NCLEX-RN, and that pattern has persisted through the Next Gen transition. The gap matters less as a prestige argument and more as a curriculum design signal. BSN programs typically include more content on leadership, research, and population health, but they also tend to integrate more sustained opportunities for clinical reasoning across four years of study. ADN programs, often condensed into two years, face a structural challenge in building the same depth of judgment-focused practice.
If you lead or teach in an ADN program, this is not a reason for discouragement. It is a reason to be deliberate about where clinical judgment in nursing education is embedded across your existing courses rather than treated as a standalone NCLEX prep add-on.
State-Level Variation: Why National Averages Only Tell Part of the Story
National pass rates mask significant variation at the state level. Some states consistently outperform the national average by several percentage points, while others fall well below it. Differences in program approval standards, clinical site availability, student demographics, and workforce pipeline pressures all contribute to this spread.
For nurse educators, the practical takeaway is straightforward: benchmark your program against your state average first, then against national figures, and then against peer institutions of similar program type and size. Resources like the NCLEX scorecard available through nurse.org allow you to make those comparisons in context, which is far more actionable than measuring yourself against a national headline number alone.
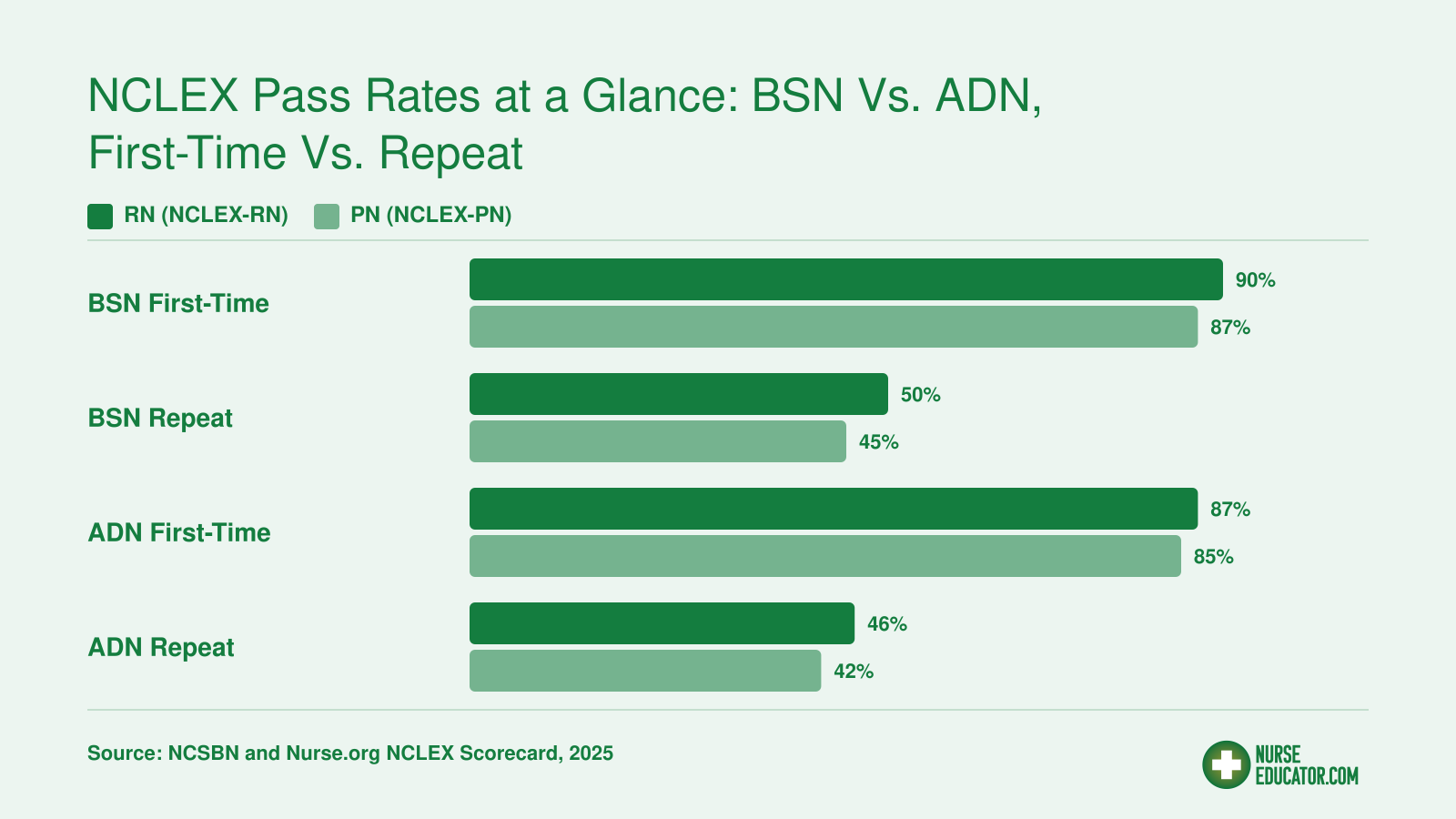
NCLEX Pass Rates at a Glance: BSN Vs. ADN, First-Time Vs. Repeat
Understanding how pass rates differ by degree type and attempt status gives you an immediate benchmark for your own program. The grouped comparison below highlights a consistent pattern: first-time test-takers outperform repeat candidates across both BSN and ADN tracks, and BSN programs tend to edge ahead of ADN programs on first attempts. Use the national first-time average (roughly 87-89% in recent reporting cycles) as your reference point when evaluating where your students stand.
How to Benchmark Your Program Using NCLEX Scorecards and Dashboards
How does your nursing program's NCLEX pass rate stack up against similar programs in your state, and are you comparing apples to apples when you look at that number?
Benchmarking is not just a "nice to have" administrative exercise. It is the foundation for every curriculum decision, remediation strategy, and faculty development plan you will make this year. Without a clear picture of where your program stands relative to peers, you risk misdiagnosing the root cause of any pass-rate dip. Here is a practical workflow you can implement right away.
Start With the Nurse.org NCLEX Scorecard
One of the most accessible tools for a quick benchmark is the Nurse.org NCLEX Scorecard, which aggregates national NCLEX pass rates, breaks them down by state, and compares BSN versus ADN outcomes so you can filter to your program type. Two features are especially valuable for educators:
- Consistently high-performing schools: These are programs that sustain strong pass rates over multiple testing cycles, not just a single standout year. They serve as aspirational benchmarks and potential sources of best practices.
- Programs that improved dramatically: These schools made measurable gains. Studying what they changed (curriculum restructuring, remediation overhauls, faculty training) can give you a realistic improvement roadmap.
Pull up the scorecard, locate your state, and compare your most recent first-time pass rate to both the state and national averages. That single comparison will tell you whether you are leading, on par, or trailing.
Dig Deeper With NCSBN Program Reports and State Board Dashboards
The Nurse.org tool is a great starting point, but your state board of nursing and the National Council of State Boards of Nursing (NCSBN) publish program-level reports that provide additional granularity. These reports let you:
- See cohort-by-cohort pass rates over multiple years, not just the latest cycle.
- Identify whether a recent dip is isolated to your program or reflects a broader statewide or national trend (this distinction matters enormously for determining root cause).
- Compare your outcomes to peer programs of the same degree type within your state, which removes the noise introduced by comparing a community college ADN program to a large research-university BSN program.
If your state board publishes a dashboard, bookmark it and check it on a regular schedule.
Adopt a Quarterly Benchmarking Cadence
Pass-rate data is often reviewed once a year, usually in a panic if the numbers drop. A quarterly cadence is far more effective:
- Quarter 1: Pull the most recent annual data from NCSBN and your state board. Compare to the prior year and note any directional shift.
- Quarter 2: Cross-reference with the Nurse.org Scorecard for national and state averages. Identify peer programs that improved and investigate what changed.
- Quarter 3: Review internal predictive data (standardized exam scores, course grades, clinical evaluations) for the upcoming graduating cohort. Flag at-risk students early.
- Quarter 4: Compile a year-end benchmarking summary for faculty and administration. Document interventions implemented and their preliminary outcomes.
This rhythm transforms benchmarking from a reactive annual event into a proactive planning tool.
Ask Yourself the Hard Questions
Before moving on, take a moment for honest self-reflection:
- Do you know your program's current first-time pass rate and how it compares to your state average?
- If your rate dipped after the transition to the Next Generation NCLEX, have you isolated whether the drop is a curriculum gap (content or clinical judgment skills in nursing not adequately covered) or a test-format adjustment issue (students unfamiliar with new item types)?
- Are you benchmarking against programs of the same degree type, or are you inadvertently comparing your ADN outcomes to BSN outcomes and drawing flawed conclusions?
If you cannot answer these questions with confidence, that is your signal to start benchmarking this week, not next semester. The data is available; the discipline of using it regularly is what separates programs that plateau from those that boost NCLEX pass rates year over year.
Curriculum Mapping to the NCLEX Test Plan: An Actionable Framework
Topic-focused lectures versus concept-integrated teaching: this structural divide determines whether your curriculum mirrors NCLEX logic or merely covers NCLEX content. The 2026 NCLEX-RN Test Plan, effective through 2029, demands the latter.1 Programs that map content to the exam's eight weighted domains and embed clinical judgment as a continuous thread outperform those that treat NCLEX alignment as a senior-year sprint.
Obtain and Deconstruct the Current NCSBN Test Plan
Download the 2026 NCLEX-RN Test Plan PDF from NCSBN and build your mapping around its eight content areas.1 Management of Care carries the heaviest weight at 18 percent, followed by Pharmacological and Parenteral Therapies at 16 percent, Physiological Adaptation at 14 percent, and Safety and Infection Control at 13 percent. Reduction of Risk Potential and Psychosocial Integrity each account for 12 percent, while Health Promotion and Maintenance and Basic Care and Comfort round out the plan at 9 percent apiece.1
Your first task: create a matrix with these eight domains as column headers and your course sequence as rows. For each course, note where each domain appears, estimate instructional hours devoted to it, and calculate your program's aggregate percentage allocation. Programs frequently discover that management-of-care skills receive 8 percent of teaching time despite representing 18 percent of test weight, or that redundant pharmacology lectures consume hours better spent on clinical judgment practice.
Shift from Topic Silos to Concept-Based Integration
The NCLEX does not ask students to recall drug names in isolation; it asks them to recognize an adverse reaction, prioritize competing nursing actions, and evaluate the outcome. Concept-based curriculum design organizes learning around clinical reasoning patterns rather than body systems or disease chapters. Integrate assessment questions that mirror NCLEX item logic: bow-tie items, matrix-grid scoring, and curriculum mapping for NGN item sets that span recognize-cues through evaluate-outcomes.2
NCSBN guidance for 2026 emphasizes embedding the Clinical Judgment Measurement Model across the curriculum, not bolting it onto a capstone seminar.1 The six-step model should appear in every simulation debrief, every case discussion, and every high-stakes exam. When students encounter the same cognitive framework in fundamentals, med-surg, pediatrics, and mental health, they internalize the pattern and apply it automatically under testing conditions.
Embed the Clinical Judgment Measurement Model as a Curriculum-Wide Thread
Each NCLEX candidate now encounters three clinical judgment case studies, with six items per case, totaling 18 scored items that demand layered reasoning.1 Programs that teach clinical judgment as a standalone module produce students who can define the model but struggle to apply it under adaptive testing pressure. Instead, code every syllabus objective and every rubric criterion to at least one of the six clinical judgment steps. Faculty should explicitly name which step an assignment targets and use consistent language: recognize cues, analyze cues, prioritize hypotheses, generate solutions, take action, evaluate outcomes. Active learning strategies in nursing reinforce exactly this kind of repeated, deliberate practice across all course levels.
Conduct a Gap-and-Redundancy Mapping Exercise
Convene your curriculum committee for a half-day workshop. Populate the test-plan matrix together, using actual syllabi and exam blueprints rather than aspirational descriptions. Highlight cells where coverage falls below NCLEX weight by 3 percent or more (the adaptive testing variation threshold).1 Mark redundant cells where multiple courses duplicate the same content without advancing clinical judgment complexity. Reallocate teaching hours based on findings: reduce repeated lectures, expand underweighted domains, and convert passive review sessions into active case-study practice. Programs that complete this exercise annually report tighter alignment, reduced content bloat, and measurable gains in first-time pass rates within two cohorts.
Teaching Clinical Judgment for the Next Gen NCLEX
Clinical judgment is the mental process nurses use to observe a patient situation, recognize what matters, decide what to do, and evaluate whether that action worked. The NCSBN Clinical Judgment Measurement Model breaks this process into six cognitive steps: recognizing cues, analyzing cues, prioritizing hypotheses, generating solutions, taking action, and evaluating outcomes. Every Next Generation NCLEX item type, from extended drag-and-drop questions to matrix grids and highlight exercises, is designed to measure one or more of these steps. Nurse educators who understand how item formats map to cognitive processes can teach students to think like the exam thinks.
The Six Cognitive Processes in Practice
The first two processes, recognizing and analyzing cues, ask students to notice relevant data in a patient scenario and determine what those findings mean together. NGN highlight items often test this by requiring students to select abnormal lab values or concerning assessment findings from a block of text. The next two, prioritizing hypotheses and generating solutions, push students to rank possible explanations and identify appropriate interventions. Matrix items frequently assess these skills by presenting multiple patient conditions alongside possible nursing actions. Finally, taking action and evaluating outcomes focus on implementation and reflection. Extended drag-and-drop questions may ask students to sequence interventions or match evaluation criteria to expected patient responses.
Classroom and Simulation Strategies That Work
Unfolding case studies remain one of the most effective tools for building clinical judgment. Present a patient scenario in stages, adding new data at each step: initial assessment, evolving vital signs, lab results, response to treatment. Students must revise their thinking as the case unfolds, mirroring real clinical practice. Innovative teaching strategies in nursing education such as think-aloud protocols during simulation debriefs can surface decision-making gaps effectively. Ask students questions like "What made you notice that change?" and "What would have happened if you had waited?"
Trend identification exercises are especially valuable. Give students a series of vital sign readings or intake-output logs collected over several shifts and ask them to spot patterns that signal deterioration. This trains the pattern recognition that underlies cue analysis.
- Unfolding case studies: Build multi-stage scenarios that require students to adjust plans as new information emerges.
- Think-aloud debriefs: Have students narrate their reasoning during simulation replay to surface decision-making gaps.
- Trend exercises: Use evolving patient data sets to practice early recognition of clinical changes.
- Peer reasoning challenges: Pair students to defend different intervention choices, strengthening hypothesis prioritization skills.
Integrate NGN-Style Items Early
Waiting until a capstone course to introduce NGN-format questions leaves students underprepared. Build matrix, highlight, and extended drag-and-drop items into course exams starting in the first semester. Early exposure normalizes the format and reinforces that clinical judgment is a skill developed across the curriculum, not a test-taking trick learned at the end.
The Dual Benefit for Curriculum Change
Teaching clinical judgment does more than raise NCLEX scores. Students who learn to recognize cues and prioritize actions in the classroom carry those habits into clinical rotations. Faculty advocating for curriculum updates can point to this dual payoff: better exam outcomes and safer, more confident novice nurses entering practice.
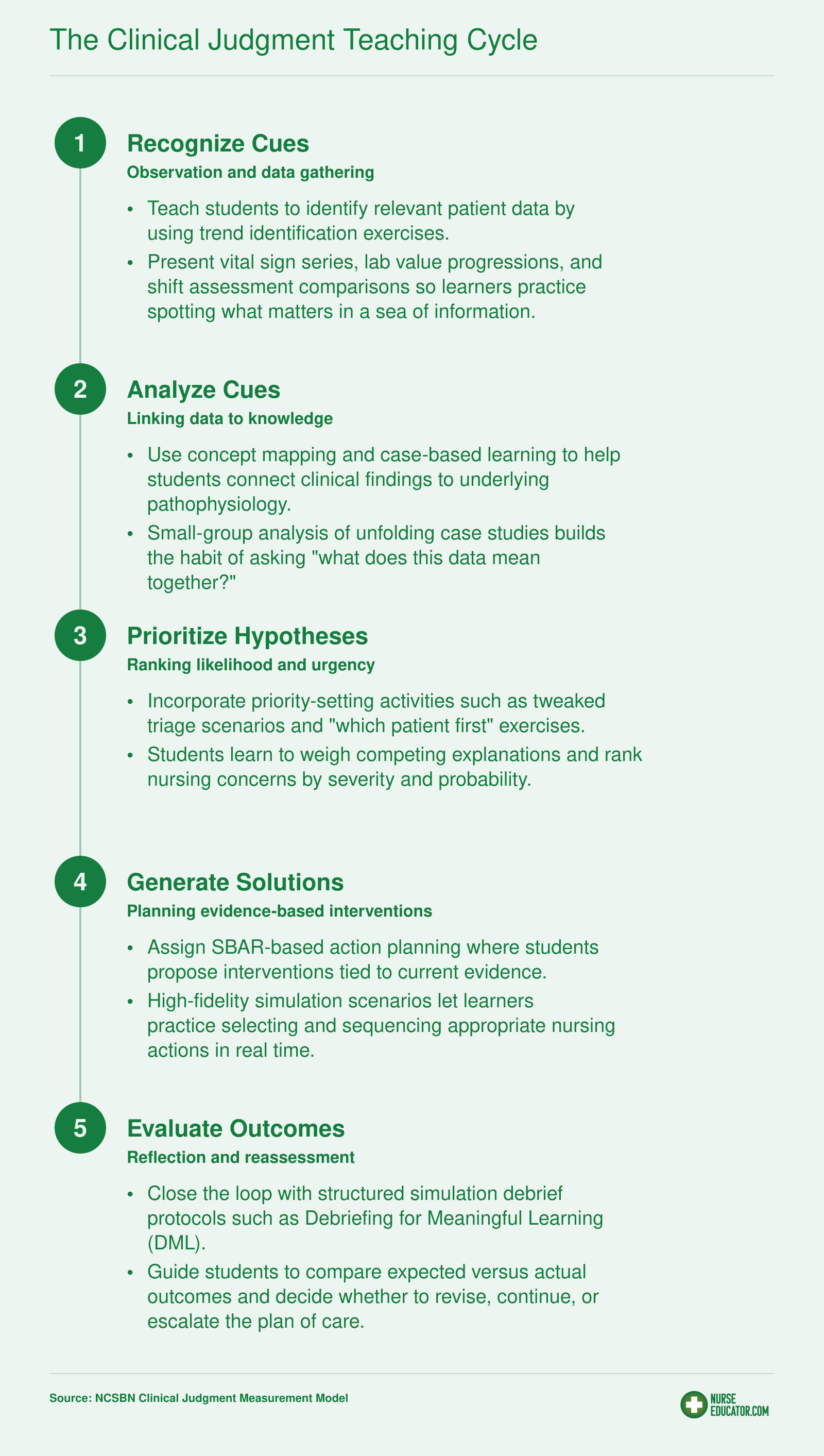
The Clinical Judgment Teaching Cycle
The NCSBN Clinical Judgment Measurement Model (NCJMM) forms the backbone of the Next Generation NCLEX. As a nurse educator, you can build your teaching around a five-step cycle that mirrors this model, pairing each cognitive phase with a concrete classroom or clinical strategy.
Related Articles
Early Warning Systems: Identifying At-Risk Students Before the NCLEX
Catching students who are struggling before they sit for the NCLEX is far more effective than responding after a failed attempt. The challenge for nurse educators is building a reliable system that identifies risk early enough to make a real difference, rather than relying on gut instinct or end-of-program assessments alone.
What the Research Points To
Nursing education literature, including studies published in journals such as the Journal of Nursing Education and Nurse Educator, consistently points to a cluster of indicators that correlate with NCLEX outcomes. Academic performance measures, particularly cumulative GPA across nursing coursework, tend to be among the strongest early signals. Students who fall below certain GPA thresholds in core science and clinical courses are generally at elevated risk, though the specific cutoff varies depending on the program and its student population.
Standardized assessment tools like ATI and HESI products are widely used precisely because they were designed to predict NCLEX readiness. Programs typically set internal benchmark scores on these assessments, and students who score below program thresholds are flagged for additional support. What the research makes clear is that a single low score matters less than a pattern: a student who underperforms on multiple proctored assessments across different content areas is signaling something more systemic than a bad test day.
Building Your Own Early Warning Framework
A practical early warning system does not require sophisticated technology. At its core, it needs two things: agreed-upon indicators and a process for acting on them promptly. Most programs find it useful to layer several data points together rather than relying on any single predictor.
Indicators worth tracking include:
- Academic performance: GPA in nursing-specific courses, particularly pharmacology and medical-surgical content.
- Standardized testing: Scores on ATI, HESI, or similar tools at key program milestones.
- Clinical evaluation: Faculty observations about a student's clinical judgment and decision-making patterns in practice settings.
- Progression patterns: Any history of course failures, extended leaves, or repeat testing attempts within the program.
The National League for Nursing (NLN) and the American Association of Colleges of Nursing (AACN) both publish resources and white papers on student success strategies that include guidance on early identification. Reaching out to these organizations, or accessing their member surveys and toolkits, can supplement what your own program data reveals.
Turning Identification Into Action
Identifying an at-risk student is only the first step. The system breaks down if there is no clear protocol for what happens next. Best practice involves assigning a point of contact, whether a faculty advisor or success coach, who connects with the student quickly, assesses barriers, and co-develops a remediation plan. The goal is to make early warning feel supportive rather than punitive, so students engage with the process rather than withdraw from it.
For programs dealing with the deeper personal and academic barriers that put students at risk, understanding how nursing students experience academic failure stigma can help faculty approach these conversations with greater empathy and effectiveness. Reviewing what high-performing programs make publicly available can surface ideas worth adapting to your own setting, and resources from nursing student retention strategies for educators offer concrete frameworks for keeping vulnerable students on track toward licensure.
Building an Effective NCLEX Remediation Program
A well-structured remediation program is not a last-resort intervention but a core component of any nursing curriculum that takes licensure preparation seriously.
Start with a Clear Philosophy
Before selecting tools or scheduling review sessions, your program needs a shared understanding of what remediation is meant to accomplish. Remediation is not punishment for poor performance. It is a structured, targeted response to identified gaps in knowledge, reasoning, or test-taking readiness. Framing it this way for both faculty and students removes stigma and increases the likelihood that struggling learners will actually engage with the support being offered.
Addressing academic failure stigma in nursing students early matters here: the most effective programs treat remediation as an ongoing process rather than a one-time event before graduation. Students who receive early, low-stakes intervention tend to show stronger outcomes than those who encounter formal remediation only after failing a milestone exam.
Layering Your Remediation Approaches
No single tool or strategy works for every student population. A layered approach that combines multiple modalities tends to produce more consistent results across diverse learner groups.
Common components worth evaluating for your program include:
- Adaptive learning platforms: Tools that adjust question difficulty based on student performance can help learners focus their study time on genuine weak areas rather than reviewing content they have already mastered.
- Success coaching: One-on-one coaching that addresses study habits, test anxiety, and time management alongside content knowledge often reaches students that purely academic interventions miss.
- Peer tutoring: Structured peer support can reinforce content for both the tutor and the student being helped, and it builds a culture of collaborative learning within your cohort.
- Capstone review courses: Intensive, near-graduation review experiences help students consolidate knowledge and practice the kind of clinical reasoning the Next Gen NCLEX requires.
When evaluating which tools to invest in, look at vendor-provided outcome data with a critical eye. Ask for results from programs with student populations similar to yours in terms of size, degree level, and clinical exposure.
Matching Interventions to Student Needs
Effective remediation programs do not apply the same intervention to every at-risk student. A student struggling with content retention needs something different from a student who understands the material but freezes under timed conditions. Build a simple triage process that helps faculty and advisors match students to the right level and type of support quickly.
Documentation matters here as well. Tracking which students entered remediation, what interventions they received, and what their eventual NCLEX outcomes were gives your program the longitudinal data it needs to refine its approach over time. Without that feedback loop, even a well-funded remediation program operates on assumption rather than evidence.
Resourcing Remediation Sustainably
Faculty time is finite, and remediation programs that rely entirely on volunteer faculty effort tend to erode under workload pressure. Keeping an eye on nurse educator burnout prevention is essential when building or expanding your program. Be realistic about what can be sustained: a smaller, consistently delivered intervention will outperform an ambitious program that runs well for one semester and then collapses. Explore whether peer tutor stipends, academic support staff, or platform-based self-paced tools can extend your reach without burning out your faculty.
Faculty Development and Its Impact on Pass Rates
Faculty development isn't just an HR checkbox. It's one of the most direct levers a nursing program can pull to move NCLEX pass rates. When instructors are equipped with up-to-date teaching methods, clinical judgment in nursing frameworks, and collaborative review practices, their students consistently outperform peers at programs where faculty are left to figure things out on their own.
The emerging evidence base
Research increasingly links structured faculty development to measurable NCLEX gains. In one multi-program analysis published in PMC, programs that implemented targeted faculty coaching and NGN-aligned training saw first-time pass rates rebound sharply, even among at-risk cohorts where predicted pass probability had dipped below 90%.1 A ScienceDirect study documented how structured faculty-to-student mentoring programs, supported by planned faculty development hours, correlated with a rise from 90% to 96.1% first-time pass rates in a single academic year.2
These numbers aren't accidental. The 2023 landscape revealed that 71% of nursing faculty nationally reported not feeling fully prepared for Next Gen NCLEX item types.1 Yet programs that closed that gap through systematic workshops, simulation training, and item-writing retreats began seeing dramatic improvement. The NCSBN's CJE-RN examination sets a score threshold of 84%, and faculty who participated in intensive clinical judgment education consistently saw their students clear that bar at higher rates.3
What accreditation reports tell program leaders
Both ACEN and CCNE accreditation standards now explicitly call for evidence of ongoing faculty development and its impact on student outcomes. In recent review cycles, programs that could demonstrate a documented cycle, identifying faculty skill gaps using NGN readiness surveys, implementing evidence-based workshops, measuring impact on HESI or ATI scores, and tracking NCLEX pass rates, received stronger evaluations and avoided citations. nursing faculty retention strategies also factor into these evaluations, since turnover disrupts the continuity that sustained improvement requires. Nurse.org's NCLEX Scorecard highlights that five nursing programs dramatically improved their pass rates between 2005 and 2023 by investing heavily in faculty training and curriculum realignment.4
Action steps for directors and deans
- Audit faculty readiness now. Use a simple anonymous survey aligned with the NCSBN clinical judgment model to pinpoint where your team needs support, whether that's building NGN-style items, teaching clinical reasoning, or designing remediation plans.
- Partner with professional organizations. The NLN offers faculty development toolkits, the AACN publishes competency-based education guides, and the NCSBN provides free Next Gen item-writing resources. Many of these include ready-to-use modules.
- Create a coaching loop. Pair experienced faculty with newer instructors for quarterly item review sessions. Wolters Kluwer's data shows that programs with a formal faculty coaching structure saw a 5, 8% pass rate increase within two testing cycles.3
- Hire for teaching ability, not just clinical expertise. Advanced practice nurses transitioning to education benefit immensely from structured onboarding in pedagogy, not just content expertise.
Faculty development isn't a one-time workshop. It's a continuous quality-improvement mindset that, when executed well, turns a program's NCLEX performance from a source of anxiety into a competitive strength.
Case Studies: Programs That Dramatically Improved NCLEX Pass Rates
Nursing programs across the country have documented significant turnarounds in NCLEX pass rates, and the common thread in nearly every published success story is a multifaceted, sustained approach rather than a single quick fix. As a nurse educator, studying these examples can help you identify which interventions are most likely to move the needle at your own institution.
Where to Find Published Case Studies
Several peer-reviewed journals regularly publish detailed accounts of programs that raised NCLEX outcomes. The Journal of Nursing Education, Nursing Education Perspectives, and the Journal of Professional Nursing are your best starting points. A PubMed search using terms like "NCLEX pass rate improvement" combined with "nursing education" and "case study" will surface relevant articles, many of which include specific before-and-after data, timelines, and the interventions used. Filter your results by these journals to focus on the most practice-relevant scholarship.
The National Council of State Boards of Nursing (NCSBN) also publishes research reports and annual NCLEX examination statistics that sometimes highlight program-level improvements. The National League for Nursing's Center for Excellence in Nursing Education maintains benchmark data that can help you contextualize any case study findings against national norms.
Common Patterns in Successful Turnarounds
While specific numbers vary by institution, published case studies tend to share several recurring themes:
- Comprehensive curriculum revision: Programs that improved most often began by mapping every course to the current NCLEX test plan, closing content gaps, and ensuring clinical judgment was threaded throughout, not just addressed in a capstone review.
- Structured remediation: Rather than offering optional tutoring, successful programs embedded mandatory remediation checkpoints tied to standardized exam benchmarks at multiple points in the curriculum.
- Early identification of at-risk students: Programs that used predictive analytics or standardized testing early in the program, sometimes as early as the first semester, reported stronger outcomes than those relying solely on late-stage exit exams.
- Faculty development: Several case studies explicitly credit ongoing faculty training in test-item writing, clinical judgment pedagogy, and evidence-based teaching strategies as a key factor in sustained improvement.
- Culture shift: Many accounts describe a deliberate move from treating NCLEX preparation as an "add-on" to embedding it as a shared, program-wide responsibility across every faculty member and course.
In general, the programs that achieved the most dramatic gains did not rely on a single intervention. Instead, they layered multiple strategies and sustained their efforts over two to four years. nursing student retention strategies for educators describe a similar pattern: early, structured support consistently outperforms last-minute intervention.
How to Access Program-Level Data
If you want to see how specific schools have improved over time, several resources can help. The Nurse.org NCLEX Scorecard allows you to compare programs nationally and by state, and it highlights schools with consistently high pass rates as well as those that have shown notable improvement. You can also review individual nursing school websites, where many institutions publish outcomes data in their accreditation self-studies and annual reports. Accreditation bodies like CCNE and ACEN require programs to report NCLEX outcomes, and some of these reports are publicly accessible.
Applying Lessons to Your Own Program
When reviewing case studies, focus less on the exact percentage-point gain and more on the process each program followed. Ask yourself:
- Did the program start with a formal gap analysis of its curriculum against the NCLEX test plan?
- How early in the student journey did the program intervene with at-risk learners?
- What role did faculty buy-in and professional development play?
- Was improvement sustained over multiple testing cycles, or did it spike and then fade?
Document what resonates and share it with your faculty team. The most useful case studies are those whose institutional context, whether community college ADN or university BSN, most closely mirrors your own. A strategy that worked at a large research university may look different in implementation at a smaller associate degree program, even if the underlying principles are the same.
Building a library of these published examples, and revisiting them during faculty retreats or curriculum committee meetings, keeps your team grounded in evidence rather than guesswork. Over time, qualities of a good nurse educator become visible in the data: programs led by reflective, evidence-driven faculty are the ones most likely to sustain their gains. Your own program's outcomes can become the next case study others learn from.
Common Questions About Improving NCLEX Pass Rates
Below are the questions nurse educators most frequently ask when working to raise their program's NCLEX outcomes. Each answer is written with the educator, not the student, in mind, so you can translate these insights directly into curriculum changes, advising conversations, and faculty meetings.
How do you translate everything you have learned about NCLEX improvement into a realistic action plan you can start this week?
Phase 1, Month 1, focuses on benchmarking. Pull your program's pass rate data, compare it against state and national figures using resources like the Nurse.org NCLEX Scorecard, and pinpoint your specific gaps by cohort, degree type, and content area. Phase 2, Month 2, turns analysis into structure: map your curriculum to the 2026 NCLEX Test Plan, align clinical judgment teaching with the NCJMM cycle, and activate your early warning system to flag at-risk students. Phase 3, Month 3, brings intervention: launch your remediation program, schedule faculty development on Next Gen NCLEX strategies, and begin tracking student progress weekly.
Revisit the NCLEX Scorecard quarterly to measure whether your changes are moving the needle. For programs ready to deepen that work, strategies nurse educators use to boost NCLEX pass rates can help you refine each phase with evidence-based detail. Sustained improvement demands sustained attention.