What you’ll learn in this article…
- Early alert systems can flag at-risk nursing students weeks before failure.
- National nursing program attrition rates range from 20 to 50 percent.
- Retaining one student can save an institution tens of thousands of dollars.
The United States is projected to need more than 190,000 new registered nurses each year through 2030, yet nursing programs across the country lose between 20 and 50 percent of their entering cohorts before graduation. Every student who leaves early widens that gap. Attrition is not simply an enrollment metric. It is a workforce supply problem, and educators sit at the point where it can be interrupted.
This collection of practical tools is written for nurse educators, program directors, and academic advisors who want to move from reactive problem-solving to systematic prevention. The sections ahead examine why students leave, how to measure your program against peer benchmarks, how to build early alert infrastructure, and how to translate evidence into a phased implementation plan.
What makes retention difficult is the absence of a single cause. Financial pressure, academic unpreparedness, schedule conflict, clinical anxiety, and nursing student bullying effects on belonging all contribute, often simultaneously. Addressing one without the others produces marginal results at best.
Why Nursing Students Drop Out: Key Attrition Factors
Most nursing programs lose between 20 and 50 percent of their entering cohort before graduation, yet few institutions conduct a structured root-cause analysis of why those students leave. Understanding the drivers of attrition is the first step toward designing interventions that actually work. The factors rarely arrive in isolation; they tend to compound in a cascade that accelerates departure. For practical purposes, you can organize them into four buckets.
Academic Pressures
Nursing curricula are dense by design. Students face heavy science prerequisites, fast-paced pharmacology and pathophysiology sequences, and the constant drumbeat of NCLEX preparation standards shaping every assessment. When a student enters with gaps in foundational sciences or underdeveloped study skills, each poor exam score erodes confidence and narrows the margin for recovery. In accelerated programs the timeline compresses these pressures even further. A candid Reddit post on r/StudentNurse illustrates the pattern well: a user described dropping an accelerated program because it was "too fast" and their "heart wasn't there," later admitting, "I don't think I'm built for a nursing career and I can't find anything else."1 That trajectory, from overwhelm to disengagement to exit, is one you will recognize if you teach in any fast-track format.
Financial and Opportunity-Cost Barriers
Tuition is only part of the equation. Many nursing students are working adults who sacrifice income to attend clinicals during weekday hours. The opportunity cost of lost wages compounds the direct cost of books, fees, and childcare. When a student picks up extra shifts to stay afloat, study time shrinks, exam scores dip, and demoralization sets in. That cascade, financial stress leading to academic decline, is one of the most common attrition sequences programs fail to interrupt early.
Personal and Psychosocial Factors
Caregiving responsibilities, nursing student mental health challenges, and imposter syndrome each carry enough weight to push a student toward withdrawal. Combined, they can be overwhelming. Students who are first in their families to pursue a health-sciences degree often lack the informal mentorship networks that help peers navigate bureaucratic and academic hurdles. Underrepresented minority students face additional compounding barriers, including stereotype threat, microaggressions in clinical settings, and a scarcity of faculty who share their lived experience. Generic support services frequently miss these intersecting stressors because they are designed around a "typical" student profile that does not actually represent the majority of today's nursing cohorts.
Clinical Environment Stressors
The transition from classroom to clinical site introduces a distinct set of risks. Practice anxiety is normal, but when it meets a hostile or dismissive preceptor, it can become paralyzing. Students who feel unsupported or belittled during clinical rotations sometimes withdraw not because they lack ability but because the learning environment signals that they do not belong. Toxic preceptor relationships are underreported precisely because students fear retaliation or believe the culture is unchangeable. A closer look at clinical placement evaluation for nursing students can help programs identify and address these environmental risks before they drive attrition.
The Cascade Effect
The most important insight for nurse educators is that attrition is almost never a single-cause event. A student dealing with childcare logistics may still succeed, but add a failed pharmacology midterm and a preceptor who questions their competence, and the decision to leave starts to feel rational. Nursing student stigma reduction strategies around academic failure matter here too, since shame often prevents students from seeking help until it is too late. Your retention strategy must account for this layering. Addressing only one bucket while ignoring the others will produce disappointing results. The next sections of this guide walk through how to detect these cascading risks early and intervene before the decision to leave becomes final.
Retention Benchmarks: What Rates Should Your Program Target?
You know your program loses students each semester, but without a baseline you cannot tell whether a 10 percent attrition rate signals a systemic problem or reflects the national norm. Benchmarking against peer programs and national data gives you the context to diagnose gaps, defend budget requests, and set meaningful retention goals.
Start with National Trends from NCSBN
The National Council of State Boards of Nursing publishes annual reports that aggregate program completion and NCLEX pass rates by state and program type. Visit ncsbn.org and download the most recent annual report PDF to see how ADN, BSN, and accelerated programs perform nationally. These reports do not always break out retention rates explicitly, but completion percentages and time-to-degree distributions offer a useful proxy: if 80 percent of admitted students graduate on time, the inverse signals attrition or delayed progression. Cross-reference next generation NCLEX changes for nurse educators with completion data to identify whether students are dropping before finals or failing licensure after graduation.
National averages currently hover around 80 percent retention across all nursing programs.2 Programs that partner with ATI Testing report an 89 percent retention rate as of 2026, suggesting that structured curriculum support and early assessment systems can lift outcomes well above the baseline.2
Cross-Reference with AACN and NLN for Program-Type Breakdowns
Once you have national context, drill down by degree level. The American Association of Colleges of Nursing surveys member schools annually and publishes retention and graduation rates in the Research & Data section of aacn.nche.edu. These reports are especially useful for BSN and accelerated BSN programs, which often enroll more competitive cohorts but also face higher stress and time-compression challenges.
For ADN programs, the National League for Nursing releases Nursing Data Review reports that summarize two-year program outcomes, including enrollment, completion, and attrition by demographic subgroup. These reports help you benchmark against community colleges and identify whether your ADN retention mirrors state or regional patterns.
Use State and School Data for Quartile-Level Precision
State boards of nursing publish program-specific data, often including annual retention and NCLEX pass rates for every approved school. Search your state board's website for annual reports or school scorecards. Connecticut data from 2024 illustrates the spread: ADN programs retained 94 percent of students with a 6 percent attrition rate, while BSN programs posted 97 percent retention and accelerated BSN programs landed at 96 percent.1 These numbers cluster tightly because Connecticut regulates minimum standards, but not every state enforces similar thresholds.
Finally, visit individual program websites. Many schools publish outcome dashboards with retention, graduation, and employment rates broken out by cohort year and sometimes by quartile. If your program retention falls below the 25th percentile of peer schools, you have a documented case for intervention funding. If you sit at the median, your challenge is proving that incremental gains justify the cost.
The Bureau of Labor Statistics at bls.gov does not track retention directly, but employment outcomes by credential and region offer a downstream signal: if graduates from your program struggle to find jobs or earn below market wages, retention problems may reflect deeper curriculum or placement misalignment.
Questions to Ask Yourself
Building an Early Alert System to Identify At-Risk Students
Proactive intervention when early warning signs appear beats reactive response after a student fails. That contrast defines the difference between traditional advising and a true early alert system. In nursing education, where a single failed exam or missed clinical can derail an entire semester, structured early identification is not just helpful but essential to retention.
What an Early Alert System Is and Why It Works
An early alert system in nursing education is a structured process that uses academic, behavioral, and self-reported data to flag students before they fail or withdraw. Rather than waiting for a final grade or a withdrawal form, these systems monitor real-time indicators, trigger alerts when thresholds are crossed, and route students to support services before problems become insurmountable. Programs with robust early alert systems have documented retention improvements of up to 10 percent and withdrawal reductions of 10 percent compared to baseline cohorts.1 One multi-institution study found that students flagged and contacted early saw a 1.4 percent GPA increase over peers who received no outreach, demonstrating that timely intervention changes trajectories.1
Concrete Threshold Examples from Published Case Studies
Effective early alert systems rely on clearly defined trigger points. Published case studies from 2023 through 2026 reveal common thresholds across nursing programs:2
- Exam score below 75 to 80 percent on the first two exams: This range captures students whose foundational knowledge gaps will compound without immediate remediation.3
- GPA falling below 2.0 to 2.5: Most nursing programs require a minimum 2.5 to progress; flagging students at or near this cutoff allows time for tutoring and study-skills coaching.1
- Attendance trigger of two to three absences: Missing even two lectures or clinical sessions correlates strongly with eventual failure in high-stakes nursing courses.2
- Declining LMS login frequency: A student who logged in daily during week one but only once in week three signals disengagement before it shows up on a transcript.
These thresholds are not punitive gates but early warning signs that prompt outreach and support.
Who Triggers Alerts, Who Responds, and When
Successful early alert systems clarify roles and timelines. Faculty typically trigger alerts when they observe red flags: a failing exam, a missed clinical, or a student who stops participating. Learning management systems can also automate flags based on login patterns, assignment submissions, or quiz performance. Once an alert is raised, responsibility shifts to an academic coach, peer mentor, faculty advisor, or counselor, depending on the nature of the concern. Best-practice programs recommend contact within 24 to 48 hours of the alert. East Carolina University's nursing program uses the Starfish early alert warning system to route alerts directly to advisors, who then schedule check-ins and connect students to tutoring or nursing student mental health support services as needed.
Responsible Use of Predictive Analytics
While data-driven flags improve outcomes, programs must avoid over-surveilling students or using predictive analytics as punitive gatekeeping. Pair every data flag with supportive, nonjudgmental outreach. Students should understand that alerts exist to help, not to track or discipline. Transparency matters: let students know what behaviors trigger alerts and what support they can expect when one is raised.
Named Platforms and Outcome Data
Several early alert platforms are in use across nursing programs. Palm Beach Atlantic University's PASS program uses Enflux to track student engagement and coordinate interventions.3 Franciscan Missionaries of Our Lady University implemented Ellucian CRM Advise and documented measurable retention gains.4 East Carolina University relies on Starfish, which integrates with their LMS to flag academic and attendance concerns in real time. QuadC offers both rule-based triggers and machine learning algorithms that predict risk based on historical cohort data.1 One institution using QuadC aimed for an 89 percent retention improvement goal in 2017 and achieved 40 percent improvement, illustrating both the potential and the practical challenges of scaling these systems.2
Building an early alert system requires upfront investment in software, training, and personnel, but the alternative, losing students who could have succeeded with timely support, carries a far higher cost.
Related Articles
Evidence-Based Retention Strategies: What Works and Why
Which nursing student retention strategies actually move the needle, and how strong is the evidence behind them?
Not every intervention carries the same weight. To help you prioritize where to invest time, budget, and faculty energy, it helps to organize retention strategies into tiers based on the strength of published evidence and reproducibility across programs.
Tier 1: High-Impact Strategies
These interventions have the most consistent track record and should form the backbone of any retention plan.
- Structured peer tutoring: Programs that pair upper-level nursing students with first-semester peers in organized weekly study sessions have reported retention gains of 10 to 15 percentage points over comparison cohorts. The key word is "structured." Drop-in tutoring centers alone are not enough; scheduled sessions with trained peer tutors and curriculum-aligned content produce measurably better outcomes.
- Faculty mentorship programs: Assigning each student a dedicated faculty mentor, rather than relying on general office hours, creates a relationship that catches early warning signs. Published case studies from BSN programs show that students paired with mentors in their first semester are significantly more likely to persist through clinicals.
- Embedded academic remediation: Instead of waiting for a student to fail an exam, high-performing programs embed remediation into the course itself. Think weekly low-stakes quizzes linked to immediate review modules, or mandatory small-group content review sessions triggered when a student scores below a set threshold. This approach normalizes help-seeking and reduces the nursing student stigma around academic struggles.
Tier 2: Moderate-Impact Strategies
These strategies address the non-academic pressures that frequently push students out.
- Financial aid counseling: Many students leave nursing programs not because of grades but because of money. Proactive financial counseling, ideally integrated into orientation and revisited each semester, helps students identify scholarships, loan options, and emergency funds before a crisis hits.
- Emergency microgrants: Small, fast-disbursement grants (often $500 or less) that cover car repairs, childcare gaps, or utility bills can prevent a temporary crisis from becoming a permanent withdrawal. Several institutions have documented that microgrant recipients return the following semester at rates above 85 percent.
- Mental health first-aid training for faculty: When faculty members can recognize signs of anxiety, depression, or burnout and respond with a warm handoff to counseling services, at-risk students are more likely to access support early. Faculty training for mental health support in nursing programs is especially important in high-pressure environments like accelerated programs.
Tier 3: Promising but Emerging
These newer approaches show encouraging early results but need more longitudinal data.
- Virtual simulations for clinical confidence: Immersive simulation platforms that allow students to practice clinical decision-making before entering real patient settings appear to reduce the anxiety-driven attrition that often spikes during the first clinical rotation. Early adopters report improved student self-efficacy scores, though retention-specific data is still being collected across multiple sites.
- Culturally responsive advising: Advising models that account for a student's cultural background, family obligations, and community context are showing promise at institutions with diverse student bodies. Rather than a one-size-fits-all advising script, these programs train advisors to ask different questions and connect students with identity-concordant mentors.
Why Layering Matters
No single strategy works in isolation. The programs with the strongest retention outcomes use a wraparound model that layers interventions across all three tiers. A student might benefit from peer tutoring (Tier 1), receive an emergency microgrant when their car breaks down (Tier 2), and feel more confident entering clinicals after virtual simulation practice (Tier 3). When these supports operate as a coordinated system rather than disconnected services, the cumulative effect is far greater than any one piece alone.
Equity-Focused Retention: A Non-Negotiable Layer
Retention strategies must be intentionally designed to serve underrepresented students, not just adapted after the fact. Federal programs like the HRSA Nursing Workforce Diversity Program1 fund nursing schools that recruit and support students from diverse and disadvantaged backgrounds. The HRSA Scholarships for Disadvantaged Students program1 and the Nurse Corps Scholarship Program2 specifically target low-income, first-generation, and racially or ethnically minoritized nursing students.
The evidence-based model for equity-focused retention combines several interlocking components: holistic admissions that look beyond GPA, targeted financial support, culturally responsive curricula, mentorship from faculty who share students' backgrounds, and structured transition-to-practice pathways. The HRSA-funded SDOH-Based APRN Retention Framework in Oklahoma, for example, applies this layered approach to support nurse practitioner students from underrepresented, rural, and disadvantaged communities.3
HRSA grant programs now require evaluation plans that disaggregate outcomes by race, ethnicity, first-generation status, and socioeconomic background.4 This is a signal to every nursing program: tracking retention data in the aggregate is no longer sufficient. You need to know which students are leaving and why, broken down by the populations you serve.
Start by auditing which tiers your program already covers, identify the gaps, and build from there. The next section provides a visual overview to help you map your current state against these strategies.
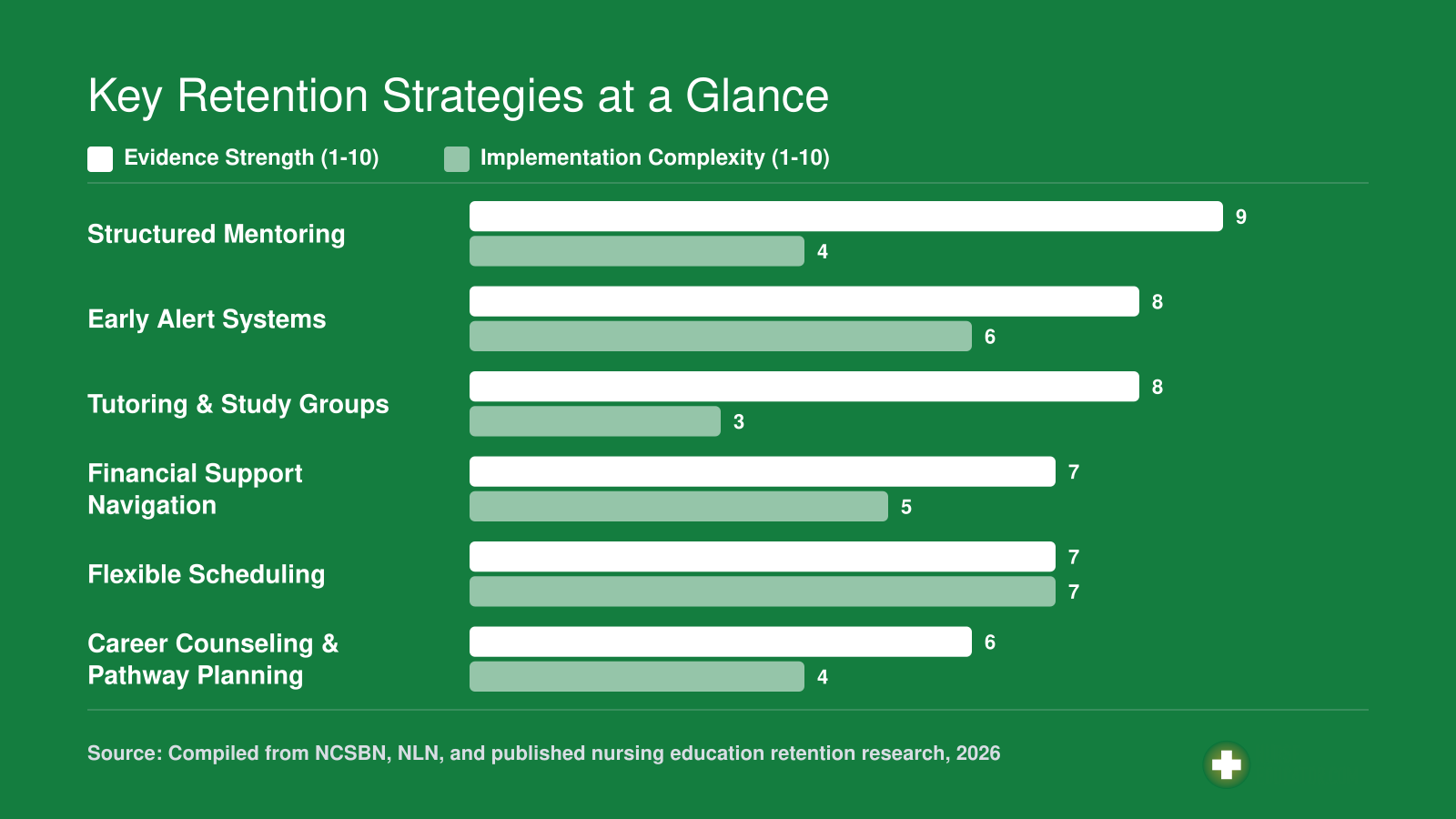
Key Retention Strategies at a Glance
Use this comparison to prioritize retention strategies based on the strength of supporting evidence and the effort required to implement them. Evidence strength and implementation complexity are each rated on a 1 to 10 scale. Strategies with high evidence and lower complexity offer the fastest wins for your program.
Lessons From the Front Lines: What a Reddit Thread Reveals About Accelerated Program Attrition
What can a single Reddit thread teach us about why nursing students drop out? In a recent r/StudentNurse post, user Inner-Frame6570 shared a raw, unfiltered account of leaving an accelerated program because it was "too fast" and "my heart wasn't there."1 Their follow-up comment, "I don't think I'm built for a nursing career and I can't find anything else," captures the crisis of confidence many accelerated students face when the intensity overwhelms their identity. The thread serves as a real-time pulse check on the pressures that drive attrition. While one story is not data, the reactions it sparked reveal patterns every nurse educator should notice.
A Candid Look at Accelerated Attrition
The original poster's words hit on three common attrition triggers: pace mismatch, emotional disconnect, and career identity doubt. Accelerated programs compress years of learning into months, and students who struggle early often internalize the experience as a personal failing rather than a program-structure mismatch. The user acknowledged the speed was the primary barrier, not the content itself. When a student says their heart isn't in it, faculty need to distinguish between burnout, clinical disillusionment, and a lack of alignment with the profession's core demands. Recognizing these signals is part of teaching emotional intelligence to nursing students, a skill that helps faculty move beyond surface-level disinterest to uncover what's really going on. In this case, the student's eventual pivot suggests the issue was more about fit with pace and delivery model than a rejection of nursing altogether.
The Community Response: Career Alternatives Emerge
What followed in the comments was a cascade of alternative career suggestions: rad tech, respiratory therapist, dental hygienist, sonography, and even LPN programs at community colleges.1 One commenter asked whether the poster disliked healthcare generally or just nursing, while another suggested considering the booming nuclear industry. This rapid reframing points to a gap many students face: they lack structured career counseling within their programs. When the primary solution offered by peers is to leave nursing entirely, it signals that students do not see a supported path to adjust course within nursing education. For educators, the takeaway is clear. Career advising must be proactive, not reactive, and should normalize pathways like ADN or LPN as honorable, strategic options rather than consolation prizes.
The Pivot: When ADN Becomes the Answer
Later in the thread, the original poster wrote, "Maybe I will look into ADN programs and see what I can do."1 That single sentence reframes the entire narrative. This student was not abandoning healthcare or even nursing. They were rejecting the accelerated format, likely due to its compressed timeline, limited remediation windows, and emotional toll. A well-timed advising intervention could have identified this mismatch weeks earlier. Admission screening for accelerated programs often focuses on GPA and prerequisites, but screeners should also assess learning style, support systems, and stress resilience. Midpoint check-ins help catch students who are silently struggling with pace before they conclude they are not built for nursing.
What Educators Can Learn From This Thread
This Reddit exchange offers three actionable lessons for nursing programs. First, accelerated tracks need robust pre-admission screening that goes beyond academic records. Use structured interviews or readiness inventories to gauge whether a student truly understands the compressed calendar and has the emotional and logistical support to handle it. Second, career counseling should be embedded throughout the curriculum, not just at graduation. Introduce ADN, LPN, and bridge options as legitimate pathways early on, so students know there is a Plan B within nursing before they feel trapped. Third, train faculty to recognize emotional signals like "my heart wasn't there" as cues for deeper conversation. Supporting nursing students with academic failure stigma matters here too: students who feel they have failed the program often carry shame that makes them less likely to seek help. Simple check-in protocols, paired with mental health resources, can prevent a temporary overwhelm from becoming a permanent exit. When a student voices doubt, the response should be, "Let's explore what's behind that feeling," not a silent nod that lets them walk away.
Adapting Strategies by Program Type: ADN, BSN, Accelerated, and Online
The central challenge in nursing student retention is that no single intervention works across every program format. A working parent in an 18-month ADN program1 faces fundamentally different pressures than a 22-year-old in a traditional four-year BSN1 or a career changer compressing a degree into 15 months.2 Effective retention requires matching your strategies to your student population's actual risk profile.
ADN Programs: Flexibility and Financial Safety Nets
Associate degree in nursing programs typically span 18 to 24 months and attract a higher proportion of nontraditional students, including working adults, parents, and first-generation college students.1 For these learners, financial strain and time scarcity are the dominant attrition drivers.
Your retention toolkit should emphasize:
- Flexible scheduling: Evening, weekend, or hybrid clinical rotations that accommodate work obligations.
- Emergency aid funds: Small grants of $500 to $1,500 can prevent a student from dropping out over a car repair or childcare gap.
- Childcare partnerships: On-campus or subsidized arrangements remove a persistent barrier.
- Financial literacy workshops: Help students navigate loan deferment, budgeting, and benefit programs before crises escalate.
Benchmark target: ADN programs with robust flexibility and aid infrastructure often achieve retention rates of 75 to 80 percent, compared to national averages closer to 70 percent for community college health programs.
BSN Programs: Cohort Strength and Faculty Connection
Traditional four-year BSN programs, typically 48 months, enroll younger students who often arrive with limited clinical exposure.3 Their top risk factors include academic rigor shock, clinical anxiety, and social isolation when cohort bonds weaken.
Prioritize interventions that build community and academic confidence:
- Peer cohort models: Assign students to stable study groups that persist across semesters.
- Faculty mentorship programs: Pair each student with a faculty advisor who meets at least monthly, not just during advising windows.
- Simulation confidence building: Extra lab time before high-stakes clinical rotations reduces anxiety and failure rates.
- Academic success coaching: Embedded tutoring and study skills workshops in the first two semesters, when attrition peaks.
Benchmark target: Well-resourced BSN programs often achieve retention above 85 percent. Programs below 80 percent should audit their first-year support structures.
Accelerated Programs: Screening and Safety Valves
Accelerated BSN programs compress the nursing curriculum into 15 to 21 months, attracting career changers who already hold a bachelor's degree in another field.2 The intensity is the point, but it is also the primary risk. As the Reddit thread discussed earlier illustrates, students who enter without full clarity on whether nursing fits them can hit a wall fast.
Effective accelerated program retention requires front-loading support:
- Pre-admission screening: Use structured interviews, realistic job previews, and self-assessments to identify candidates whose expectations align with the program's pace.
- Mental health support: Embed faculty training for mental health support in nursing programs rather than relying on general campus services.
- Alternative pathway counseling: When a student realizes nursing is not the right fit, help them pivot to related fields like respiratory therapy, radiology technology, or healthcare administration before they simply disappear.
- Pacing transparency: During orientation, provide a week-by-week calendar so students can visualize the workload before committing.
Benchmark target: Accelerated programs with strong screening and early support often retain 75 to 82 percent of students. Programs below 70 percent may be admitting students who would thrive in a longer-format program instead.
Online and Hybrid Programs: Proactive Connection
Online and hybrid RN-to-BSN or MSN programs, often 12 to 18 months, serve working nurses seeking advancement.4 Isolation and self-regulation challenges are the primary threats. Students who feel invisible to their instructors are far more likely to disengage.
Build retention through deliberate outreach:
- Proactive advisor contact: Require advisors to reach out at set intervals, not just respond when students initiate.
- Virtual cohort communities: Create discussion spaces, video meetups, or peer accountability partnerships that mimic in-person connection.
- Structured check-ins: Automated progress alerts combined with personal follow-up when engagement drops.
- Clear milestone mapping: Help students see exactly where they are in the program and what remains.
Benchmark target: Online programs with strong engagement infrastructure often retain 80 percent or more. Those relying on passive support typically fall below 70 percent.
Tailoring your retention strategy to your program type is not optional. It is the difference between interventions that land and interventions that miss entirely.
Faculty Workload, Cost, and ROI: Making the Case for Retention Investment
Every nursing student who walks out the door before graduation represents a specific, calculable loss to your institution. We are not talking about an abstract setback. We are talking about tuition revenue that stops, a clinical placement slot that goes to waste, and the recruiter hours spent filling the seat again the following cycle.
What Attrition Actually Costs
BSN programs nationally see attrition rates around 20%,1 and across nursing programs broadly, dropout rates can range from 10 to 30 percent depending on program type and institutional context.1 When you multiply even a modest attrition rate against your cohort size, the financial picture sharpens quickly.
Here is a concrete way to think about it. If a student leaves midway through a four-semester program, the institution loses the remaining tuition those semesters would have generated. A clinical placement that took months to negotiate sits unused. Faculty time spent on that student's onboarding, advising, and remediation produces no graduation outcome. There is no precise published figure for what one unfilled seat costs a nursing program in isolation, but the downstream numbers from healthcare workforce research give a useful frame: replacing a single registered nurse in clinical practice costs institutions roughly $49,500 to $72,700, according to 2026 workforce data.2 The pipeline starts in your program. Every student your program fails to retain is a future vacancy that hospitals will pay dearly to fill.
The ROI Argument for Retention Investment
Consider a retention coordinator role budgeted at $50,000 per year. If that coordinator's early outreach, advising, and remediation support keeps five additional students enrolled through graduation each year, and each of those students pays tuition across two or three remaining semesters, the position pays for itself within the first cohort cycle. That is not speculative math. It is the same logic hospitals apply when they calculate that reducing nurse turnover by two percentage points saves nearly $578,000 annually.2 Your program is the front end of that pipeline.
The American Association of Colleges of Nursing reported that nursing schools turned away more than 65,000 qualified applicants in 2023, largely because of faculty and resource shortages.3 That context matters when you make the budget case: your institution is not recruiting from an unlimited pool. Every seat you fill and then lose is a seat that a qualified applicant could have occupied. The nursing faculty shortage compounds this reality, since fewer instructors mean fewer sections, less advising capacity, and thinner safety nets for at-risk students.
Addressing Faculty Workload Honestly
Retention strategies do add work. Mentorship hours, early-alert follow-up conversations, and remediation sessions are real time commitments that fall disproportionately on already stretched faculty. Pretending otherwise undermines faculty trust and makes programs less likely to sustain these efforts. Nurse educator burnout prevention deserves its own budget line alongside retention investment, because the two challenges feed each other directly.
Offsets worth proposing to administration include:
- Course release: Faculty leading formal mentorship cohorts receive one course release per semester in exchange.
- Adjunct support: Hire adjunct clinical instructors specifically to handle remediation labs, freeing full-time faculty for advising and curriculum work.
- Technology automation: Early-alert platforms that pull attendance, grade, and clinical-completion data automatically reduce the manual monitoring burden, so faculty receive a flagged list rather than hunting for struggling students themselves.
Your Elevator Pitch for Deans and Provosts
When you sit down with administration, lead with the workforce pipeline argument, not the student welfare argument. Both matter, but budgets respond to workforce data. A version you can adapt: "Our program loses students at a rate that mirrors national benchmarks, and each departure represents lost tuition, a wasted clinical seat, and a future RN vacancy that regional hospitals will spend $49,500 or more to fill. A targeted retention investment of $50,000 to $75,000 annually, structured around an early-alert system and dedicated advising capacity, can demonstrably reduce that attrition. It also protects our NCLEX pass rates and the accreditation standing that depends on them. This is not a student-services expense. It is a workforce infrastructure investment with a measurable return."
When a nursing student drops out midway through a program, the institution can lose tens of thousands of dollars in tuition revenue, but the ripple effect reaches further: every departure during a national nursing shortage means one fewer prepared nurse entering a workforce that desperately needs them. Retention is not just a financial issue; it is a public health imperative.
Implementation Playbook: A Step-By-Step Timeline for Your Program
Retention work fails when it launches as a scattered set of well-intentioned pilots. A phased two-year timeline, with named owners at each step, is what turns retention from a hallway conversation into a program-level system. Use the playbook below as a scaffold and adapt the pacing to your academic calendar.
Semester 0: Pre-Launch (Audit and Buy-In)
Before you change anything, understand what you have.
- Audit current attrition data: Pull three to five years of withdrawal, failure, and completion figures broken out by cohort, course, and demographic slice. Owner: program director with institutional research support.
- Identify stakeholders: Map every person who touches student progress, course faculty, clinical coordinators, academic advisors, financial aid, counseling. Owner: program director.
- Secure buy-in: Present the attrition audit to the dean and faculty assembly with a proposed retention charter and a modest resource ask. Owner: program director plus one faculty champion.
Semester 1: Pilot
Start small, measure everything.
- Launch an early alert system for one cohort: Configure LMS flags for missed assignments, low quiz scores, and clinical absence. Owner: IT/LMS admin plus faculty champion.
- Assign peer mentors: Pair each first-semester student with a second- or third-semester mentor. Owner: academic advisor.
- Establish baseline metrics: Define your target retention rate, response time to alerts, and mentor contact frequency. Owner: faculty champion.
Year 1: Expand
Once the pilot cohort shows signal, widen the footprint.
- Add financial support mechanisms: Small emergency grants, textbook lending, and childcare stipends often prevent the exits that GPA alone would not predict. Owner: program director with financial aid.
- Train faculty on warning signs: Run two workshops on recognizing burnout, imposter feelings, and clinical anxiety, and on how to refer without stigma. Owner: faculty champion. Faculty training for mental health support in nursing programs can help you structure these sessions around evidence-based referral protocols.
- Begin an equity audit: Disaggregate outcomes by race, first-generation status, and part-time work hours. Owner: program director with institutional research.
Year 2: Sustain
Move from project to practice.
- Analyze first full-cycle outcomes: Compare pilot and expansion cohorts against the baseline. Owner: faculty champion.
- Iterate on interventions: Cut what did not move the needle. Double down on what did.
- Publish results for accreditation: Package the data for CCNE, ACEN, or state board reporting, and for your own faculty newsletter. Owner: program director.
Quick Wins You Can Start This Week
Zero budget, zero committee approval:
- Review last semester's withdrawal roster and note patterns in course, timing, and stated reason.
- Email every student currently flagged in your gradebook as at-risk, with one specific offer of help.
- Schedule a faculty brown-bag lunch on retention and invite one academic advisor to co-lead.
Sustainability: Build It Into the Culture
Retention is not a project with an end date. It is a lens you apply to every annual program review, every curriculum revision, and every hiring decision. Add a retention section to your yearly self-study. Ask about retention in faculty evaluations. Report cohort-level outcomes to students themselves. Fostering a research culture in nursing education gives you a framework for documenting and disseminating those outcomes so they carry weight beyond your own program walls. The programs that hold onto their students are the ones where holding onto students is simply how the work gets done.
Frequently Asked Questions About Nursing Student Retention
These are the questions nurse educators ask most often when building or refining a retention plan. Each answer offers a concise starting point; for deeper guidance, the corresponding sections of this guide walk you through evidence, benchmarks, and implementation steps.
Most programs lose 20 to 50 percent of their entering cohort before graduation. But when a student like the Reddit user who said "my heart wasn't there" walks away, the signal was present long before the departure. Build an early alert system, invest in equity-focused wraparound support, and track your benchmarks against the data in this guide. The highest-leverage move this week: download your program's attrition data and measure it against the benchmarks you just read. That first honest look turns anonymous forum confessions into conversations that happen in your office, while there is still time to act. Careers in nurse education depend on educators who treat retention not as a side project but as a core professional responsibility.