What you’ll learn in this article…
- In 2024, 80,162 qualified nursing applicants were turned away while faculty vacancy rates reached 7.64%.
- McLeod Health's $75,000 investment in Florence-Darlington Technical College ensures a continuous ADN pipeline.
- Shared faculty positions and joint appointments let experienced nurses teach without leaving clinical practice.
- Grow-your-own models cover tuition for bedside nurses pursuing graduate educator degrees.
Why are nursing schools closing their doors to tens of thousands of qualified applicants each year? In 2024, over 80,000 aspiring nurses were turned away, and a 7.64% faculty vacancy rate was the primary bottleneck. Open educator positions slash enrollment capacity, no matter how many qualified students apply. This math is unforgiving.
Clinical partnerships offer a direct way to break that bottleneck. When hospitals and health systems share faculty, co-fund positions, and expand clinical sites, they grow the pipeline at both ends: more instructors teach more students in more placements.
Hospitals that invest in these partnerships are no longer just clinical rotation sites. They are becoming co-educators, deliberately building the faculty workforce that will train their next generation of nurses.
Why Academic-Clinical Partnerships Matter Now
Every nursing program director today feels the pinch: expanding healthcare demand collides with shrinking educator supply, putting quality clinical training at risk. The numbers behind this tension make a compelling case for bold, collaborative action.
The Faculty Pipeline Is Running Dry
Nationwide, the nursing faculty shortage left 7.2 percent of positions vacant in the 2024, 2025 academic year, representing 1,588 full-time roles that schools could not fill.1 The outlook is even starker when you zoom in regionally: vacancy rates hit 10.0 percent in the West, 9.8 percent in the South, and a staggering 12.3 percent in Delaware,2 showing the variation in the nurse educator shortage by state. Compounding the shortage, one-third of the current faculty workforce is projected to retire by 2025.4 Meanwhile, the pipeline of new educators is thinning. Master’s nursing programs saw enrollment dip 0.9 percent in 2022, 2023, and PhD enrollment dropped 3.1 percent, extending a 17.5 percent decline since 2013.5
How Faculty Gaps Choke Clinical Capacity
A missing faculty member does more than leave a podium empty. Because faculty supervise student clinical groups, each unfilled position directly reduces the number of students a program can accept. This creates a bottleneck: clinical sites may stand ready to host learners, but without enough instructors to oversee them, enrollment caps stay in place. The result is a heartbreaking waste of talent. In 2023, 65,766 qualified nursing applicants were turned away from entry-level programs, a figure that AACN ties overwhelmingly to faculty shortages.5 The students are there; the teachers are not.
Dual Benefits of Academic-Clinical Partnerships
Academic-clinical partnerships attack this problem from two sides at once. When hospitals and health systems share expert clinicians as joint-appointment faculty or adjunct instructors, they immediately add teaching capacity without lengthy hiring searches. At the same time, formal collaboration agreements expand the number of clinical placement slots, ensuring that enrolled students get the supervised hours they need. These arrangements turn a zero-sum game (more students means overstretched faculty) into a positive-sum model where clinical partners invest directly in growing their own future workforce.
By the Numbers: A Snapshot of the Crisis
- National facility vacancies: 7.2% (2024, 2025), with 1,588 full-time roles unfilled1
- Retirement cliff: One-third of faculty expected to retire by 20254
- Enrollment disruption: 65,766 qualified applications denied in 2023 due largely to instructor gaps5
- Regional extremes: Delaware 12.3%2, West 10.0%, South 9.8%, North Atlantic 8.1%, Midwest 6.9%
- Pipeline decline: Master’s enrollment down 0.9%, PhD enrollment down 3.1% (2022, 2023)5
These figures are not abstractions; they are the daily reality for deans, program directors, and the students whose ambitions are deferred. Partnerships offer the most immediate lever to reverse the trend, if we act now.
Proven Partnership Models: From Joint Appointments to Shared Faculty
Academic-practice partnership models in nursing education have evolved into structured arrangements that bridge clinical expertise and classroom instruction, yet comparative data on their effectiveness remains fragmented. Understanding the distinct designs and benefits of joint appointments and shared faculty positions is essential for institutions aiming to address the nursing faculty shortage and scale their nurse educator workforce.
Joint Appointments: Bridging Clinical Practice and Academia
In the academic-practice joint appointment model, Advanced Practice Registered Nurses (APRNs) maintain a dual role: practicing clinically within a health system while holding a teaching position at a university. The funding structure typically preserves the nurse’s clinical salary, with teaching duties compensated through adjunct pay or formal inter-organizational agreements. Key benefits include a direct increase in clinical placement capacity and preceptor availability, as well as improved learner readiness thanks to exposure to current, real-world practice. Data from the American Association of Colleges of Nursing (AACN) highlights that such partnerships also strengthen the alignment between academic curricula and workforce needs1, though standardized metrics on long-term faculty retention are still developing. Conceptual analyses published in ScienceDirect emphasize that clear workload expectations, balancing clinical productivity with academic output, are critical to burnout prevention and ensuring model sustainability.2
Cross-Institution Research Joint Appointments
A less common but impactful variant, the university-non-university research joint appointment, places a single researcher in a professorship and a leadership or research role across two institutions. In nursing education, this might pair a nurse scientist with a health system’s research institute. The funding is shared, with differentiated salary components and cost-sharing agreements. This structure not only strengthens institutional competitiveness for grants but also reduces the traditional divide between academic research and clinical innovation. While not directly focused on teaching, such roles can incorporate student mentoring and contribute to evidence-based curriculum updates, supporting the broader faculty pipeline.
Shared Faculty Within a Single Institution
Intra-university shared appointments distribute a faculty member’s teaching and service responsibilities across multiple departments or units, with a single institutional salary budgeted proportionally. For nursing programs, this could mean joint roles with public health, health administration, or simulation technology departments. The primary advantage is fostering interdisciplinary innovation, which aids student learning and faculty recruitment. The University of Memphis has documented that shared appointments can enhance faculty diversity and retention by offering varied career pathways without forcing a full departure from clinical teaching.4 However, administrative complexity requires transparent workload splits and clear tenure guidelines, areas where the Leibniz Association’s guides on joint appointments provide valuable frameworks.3
Today's hospitals are no longer just clinical placement sites: they are stepping into the role of co-educators. By investing directly in faculty development pipelines, they are building the educator workforce that will train their future nurses.
Expanding Clinical Placement Capacity Through Partnerships
Expanding clinical placement capacity is the single most immediate lever for increasing the number of qualified nursing graduates. When clinical sites are scarce, programs cap enrollment, even when qualified applicants are plentiful. Academic-clinical partnerships directly address this bottleneck by creating more student slots, sharing teaching loads, and deploying hospital-based educators. The result: more nurses enter the workforce each year without overstretching overburdened faculty.
The Capacity Bottleneck and How Partnerships Unlock It
Nursing schools routinely cite clinical placement shortages as the top reason for turning away applicants. A single faculty member can supervise only 8 to 10 students in a typical hospital unit, and competition for floor time is fierce. Partnerships flip the equation: clinical organizations that commit dedicated units, shared simulation space, and practicing RNs as adjunct instructors can double or triple a program's clinical throughput. For example, McLeod Health's $75,000 contribution to Florence-Darlington Technical College's ADN program in June 2026 helped sustain a five-semester pathway that relies on clinical slots at McLeod facilities, protecting placement capacity for a full cohort of aspiring registered nurses.
Dedicated Education Units: A Force Multiplier for Faculty
Dedicated education units (DEUs) are hospital floors or units where staff nurses are formally trained and compensated to serve as preceptors for students. In a DEU model, one academic faculty member can oversee an entire unit of students because the day-to-day guidance comes from the unit's clinicians. This innovative teaching strategy easily expands capacity: a unit that previously accommodated 6 students under direct faculty supervision can host 12 to 16 when preceptors share the teaching load. Many DEU agreements include preceptor stipends funded by the clinical partner, making it financially feasible for hospitals to participate without straining their own budgets.
Sharing Simulation Resources to Ease Clinical Demand
Clinical hours spent in high-fidelity simulation can substitute for up to 50% of traditional clinical hours in many state boards of nursing, yet simulation labs are expensive to build and staff. Partnerships allow academic institutions and hospitals to share these resources. A hospital might fund a simulation suite on campus in exchange for priority access for its own staff training, while the college uses it to deliver clinical experiences in maternal-child, critical care, and other high-acuity areas. This shared model reduces the total number of live clinical placements needed per student each semester, effectively freeing up hospital-based slots for additional students.
Clinical Faculty Associates: The Bridge Between Bedside and Classroom
A growing number of partnerships formalize the role of clinical faculty associates: hospital-employed RNs who are taking steps toward becoming a nurse educator by teaching one or two clinical groups per semester while maintaining their practice roles. These associates bring current bedside expertise into the educational setting and allow programs to add sections without hiring full-time faculty. A single clinical faculty associate can oversee 8 students for a rotation, adding that many slots to a program's capacity. The hospital typically compensates the nurse for teaching time, while the academic institution provides orientation and pedagogical support. This shared appointment model has been shown to increase a nursing school's annual enrollment by 10 to 15 percent within two years of implementation.
Questions to Ask Yourself
Building a Nurse Educator Pipeline From Clinical Sites
What Is the Grow-Your-Own Model?
The grow-your-own model mirrors clinical ladder programs: it identifies highly competent bedside nurses who show teaching potential that align with the qualities of a good nurse educator and invests in their graduate education. A hospital might cover tuition for a nurse to earn an MSN or DNP with a nurse educator concentration via online nurse educator programs while the nurse continues to work part time. In return, the nurse commits to serve as preceptor, clinical instructor, or adjunct faculty for a set period post-graduation. This approach reduces the financial barrier that so often prevents staff nurses from stepping into educator roles. It also shortens the hiring cycle because the clinical partner already knows the candidate's skills, temperament, and cultural fit.
For academic programs, the benefit is twofold. First, they gain faculty who arrive with deep, real-world clinical knowledge that enriches course content and simulation debriefings. Second, the partnership strengthens the relationship between school and clinical site, smoothing the way for expanded clinical placements and joint curriculum planning. When both sides invest in the pipeline, it stops being a one-time favor and becomes a shared strategy for workforce stability.
Return-to-Teach Pathways: A Win-Win Investment
A return-to-teach pathway formalizes the arrangement through a contractual scholarship. The clinical employer pays a portion or all tuition for a nurse to pursue advanced education with an education specialty. In exchange, the nurse agrees to teach a specified number of semesters or years at the partner nursing school, often while maintaining a reduced clinical schedule. If the nurse leaves before fulfilling the commitment, a prorated repayment protects the employer's investment.
These pathways work especially well for ADN programs, where clinical expertise is paramount and instructor shortages are acute. A community college can partner with a regional hospital to build a pool of possible instructors who are already familiar with the hospital's patient populations, documentation systems, and culture. Many health systems are stepping up to fund tuition assistance for aspiring nurse educators, effectively creating a farm system of faculty grown from the bedside.
Real-World Success Stories
Several academic-practice partnerships have already shown that these programs work. For example, some health systems have launched formal nurse educator fellowships: a staff nurse with a BSN applies for a two-year fellowship that funds an MSN in nursing education while the nurse teaches clinical rotations for the partner school. At completion, the nurse emerges as a qualified faculty member with a job waiting. One academic medical center reported that its grow-your-own program produced five new clinical instructors within three years, all of whom remained in teaching roles beyond their initial commitment.
Another model is the post-master's certificate in nursing education that clinical partners sponsor for nurses who already hold an MSN in a clinical specialty. This fast-track route adds the educational theory and practicum experience needed to transition into a teaching role without repeating a full degree. Because the sponsoring hospital can see the immediate payoff in better-prepared nursing students and improved orientation outcomes for new hires, the return on investment becomes clear to administrators.
Bringing Bedside Expertise into the Classroom
Perhaps the most compelling argument for these pipelines is the classroom impact. Nurses who step directly from patient care into teaching bring a currency that no textbook can match. They know the latest safety protocols, the newest EHR workflows, and the real-time challenges of staffing shortages. Students hear not just the ideal but the actual, and they learn to think on their feet from someone who does it every shift. This credibility builds trust and accelerates clinical reasoning.
Moreover, when a hospital invests in growing its own educators, it incidentally strengthens the entire teaching team. Full-time academic faculty gain a reliable partner who can bridge the gap between theory and practice, and the school can offer more clinical sections or reduce student-to-faculty ratios. The end result is a more robust pipeline of practice-ready graduates, a direct antidote to the very nursing shortage that drives the partnership in the first place.
Did you know? In 2024, nursing schools turned away 80,162 qualified applicants, even as faculty vacancy rates hit 7.64%. Each empty educator seat limits the nursing pipeline, underscoring why academic-clinical partnerships and grow-your-own faculty programs are crucial.
Funding and Loan Forgiveness Strategies for Sustainable Partnerships
Financial sustainability often makes or breaks academic-clinical partnerships, but a range of federal and state programs can provide the fuel that keeps them running. By weaving these funding mechanisms directly into your partnership agreement, both the academic institution and the clinical partner can secure long-term viability while building a stronger nurse faculty pipeline.
Federal Support: The Nurse Faculty Loan Program (NFLP)
The Nurse Faculty Loan Program (NFLP) is a federal initiative that empowers schools of nursing to offer low-interest loans to graduate students who commit to teaching after graduation. Accredited schools apply for funds through a competitive grant (the 2026 cycle is HRSA-25-070)1 and then lend up to $35,000 per year to eligible students.1 The real incentive: 85% of the total loan balance is cancelled when the graduate completes four years of full-time faculty service.2 Priority goes to full-time PhD and DNP students, particularly those beyond their first year who lack full funding. For partnership planning, clinical sites can promote NFLP to nurses considering advanced degrees, such as a nurse educator degree, while academic partners can leverage the program to attract aspiring educators from the clinical workforce.
Loan Repayment Incentives: Nurse Corps and State Programs
The Nurse Corps Loan Repayment Program repays up to 85% of outstanding nursing education debt in exchange for service in high-need areas, including faculty roles at eligible schools. Clinical partners can actively encourage staff to explore this route for transitioning into teaching. At the state level, loan repayment programs often fill in gaps. Georgia, for example, runs an APRN Loan Repayment Program that provides $10,000 per year (up to $40,000 over four years) for nurses providing direct care in underserved rural areas, and a Nurse Faculty Loan Repayment Program that awards up to $25,000 for a two-year commitment to teach at a Georgia institution.3 Many other states offer similar programs; partnership agreements should include regular scans of available state funding and a plan to promote them to potential faculty candidates.
State Tax Credits and Institutional Incentives
Beyond loan repayment, several states offer tax credits or direct grants to healthcare organizations that share employee educators or fund joint appointments. While specifics differ by state, these incentives can offset the cost of clinical release time, adjunct faculty salaries, or partnership infrastructure. Partners should consult their state's workforce development office to identify applicable credits. For instance, some programs reimburse a portion of salary costs when a hospital employee devotes a set number of hours to clinical instruction. Embedding a shared-funding model into the agreement ensures both parties capture these financial benefits and maintain commitment through changing budget cycles.
Baking Incentives into the Partnership Agreement
To transform temporary grants into lasting support, build these programs directly into the partnership contract. Spell out responsibilities: which entity applies for NFLP or state funds, how loan forgiveness service years are documented, and how tax credits are divided. Create a joint oversight committee to monitor grant cycles, renewals, and reporting deadlines. Formalizing these details turns ad hoc funding into a predictable resource stream, aligns clinical and academic objectives, and demonstrates to stakeholders that the partnership is financially robust enough to endure long-term.
Related Articles
Real-World Partnerships That Are Moving the Needle
The most promising academic-clinical partnerships today are no longer just about sharing resources: they are reshaping how nursing education is delivered and funded.
McLeod Health and Florence-Darlington Technical College: Investing in Community-Based ADN Programs
In June 2026, McLeod Health made a $75,000 contribution to Florence-Darlington Technical College (FDTC) to sustain its Associate Degree in Nursing program. The five-semester ADN program prepares students for RN licensure and represents a critical pipeline for local healthcare. Tony Derrick, Chief Nursing Officer for McLeod Regional Medical Center, tied the investment directly to demographic pressures: "The need for healthcare services is increasing due to the national shortage of nurses and the growing number of aging baby boomers." Dr. Debbie Cheek, FDTC’s Interim President, called the funding "a strong commitment to developing the next generation of healthcare professionals." This partnership keeps the program operational, ensuring a steady flow of new nurses into a system strained by retirements.
Alabama Academic-Practice Partnership: A Data-Driven Model with Measurable Gains
A multi-year partnership in Alabama between a university and health system produced outcomes that quantify the impact of joint appointments. The arrangement placed 140 nurses into academic roles, expanding faculty capacity by 30-50% and addressing the nurse educator demand. Nurse retention climbed from 68% pre-partnership to 84% afterward, while hospital-acquired pressure injuries dropped by 95% between 2018 and 2024. These gains show how integrating clinical nurses into teaching, an innovative teaching strategies approach, not only fills faculty gaps but also sharpens bedside care.3 BSN and RN-to-BSN graduates from the partner school saw employment rates of 50% and 62%, respectively, with many staying in the system. Nationally, similar joint appointment models have boosted enrollment capacity by 50-60% and raised first-time NCLEX pass rates from 84-86% to 90-94%, proving that strategic alignment between service and education delivers hard returns.12
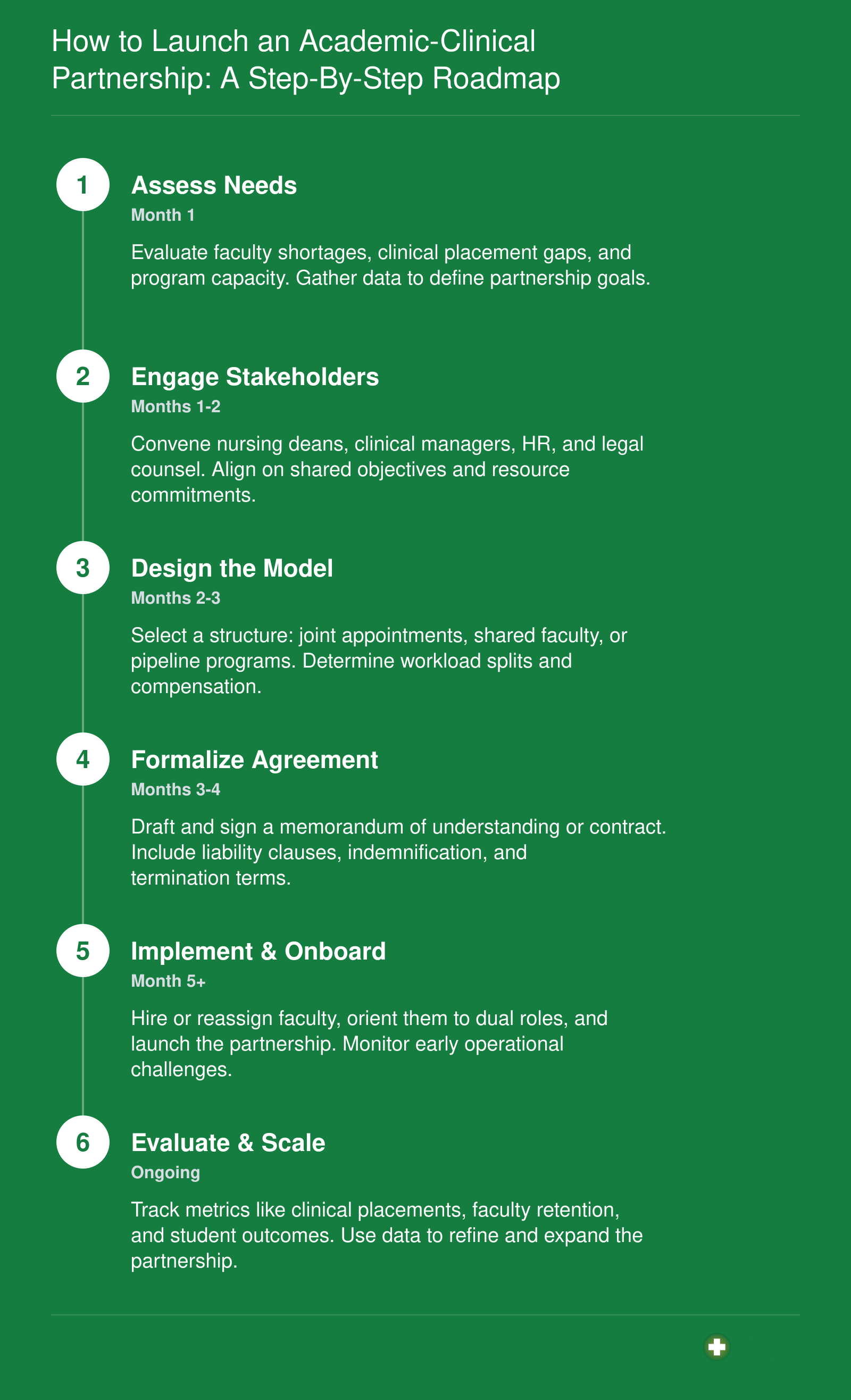
How to Launch an Academic-Clinical Partnership: A Step-By-Step Roadmap
Launching a successful academic-clinical partnership requires thoughtful planning and collaboration. Follow this roadmap to build a sustainable model that addresses the nursing faculty shortage.
Measuring Success: Outcome Metrics for Partnership ROI
Tracking the return on investment for academic-clinical partnerships helps institutions justify funding and expand programs. The metrics below represent typical outcomes for pipeline and shared faculty models.