What you’ll learn in this article…
- Nurse educators typically need an MSN or doctoral degree, while registered nurses can begin practice with an associate degree.
- The BLS reports a national median salary of $80,780 for RNs versus $82,040 for postsecondary nursing instructors as of May 2024.
- Earning the CNE credential from the NLN strengthens job prospects and is required or preferred by many academic employers.
- Transitioning from clinical nursing to education often starts with precepting students or mentoring new hires on the unit.
Registered nurses work at the bedside or in outpatient settings, delivering direct patient care. Nurse educators work in classrooms, simulation labs, and clinical training sites, preparing students and staff to do that work. The shift from one role to the other is common, but it requires additional education, a different credential set, and a fundamental change in how you spend your day.
Many nurses reach a point where the appeal of teaching outweighs the demands of shift work, but the decision is rarely simple. Burnout, scheduling control, and long-term earning potential all factor in, alongside questions about whether you want to stay close to patients or step back into a mentoring and curriculum-design role. Understanding why nurses choose to transition into a career as a nurse educator can help you weigh those motivations against your own. The choice also intersects with another common fork: whether to pursue a nurse practitioner degree instead, which keeps you in direct care but in an advanced capacity.
Nurse educator salaries lag behind NP wages in most states, but the role offers predictable hours, academic calendars, and influence over how the next generation practices.
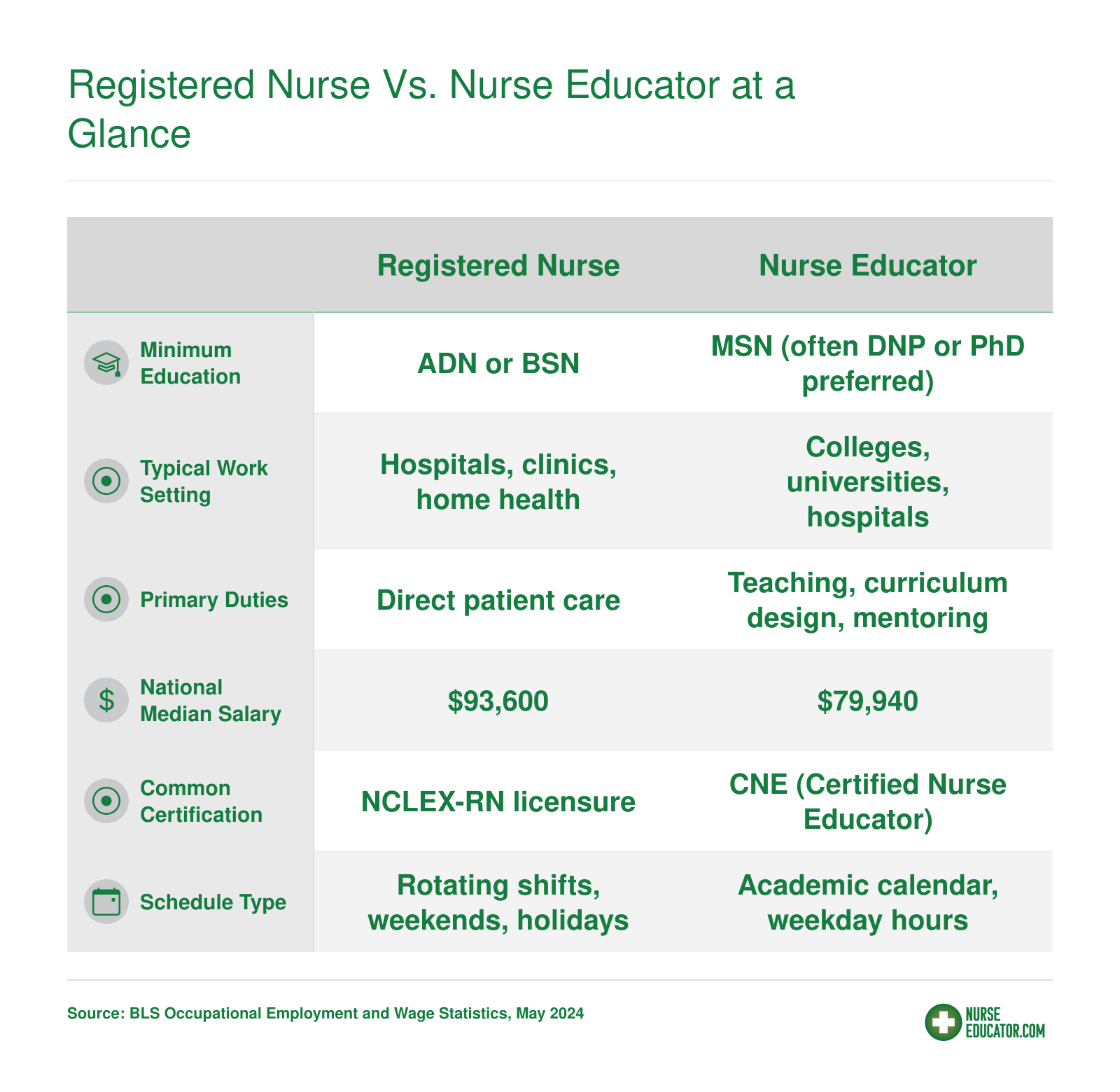
Registered Nurse Vs. Nurse Educator at a Glance
Before diving into the details, here is a quick-reference snapshot comparing the two career paths across key attributes. Use this as your starting point, then read on for the full breakdown.
What Does a Registered Nurse Do?
Registered nurses deliver hands-on patient care in a wide variety of clinical settings, coordinating treatment plans, monitoring health status, and serving as the connective tissue between patients, families, and the broader care team. The work is grounded in concrete, repeatable tasks that fill every shift: taking vital signs, starting IVs, administering medications, updating care plans, teaching patients about post-discharge instructions, and documenting every intervention in the electronic health record. The scope is clinical, the tempo is fast, and the work demands physical stamina and emotional resilience.
A Typical Day on the Floor
Most hospital-based RNs work 12-hour shifts, often starting at 7 a.m. or 7 p.m., and the rhythm is set by patient acuity and unit protocols. A medical-surgical nurse might juggle four to six patients, starting each shift with bedside assessments, reviewing overnight labs, reconciling medication orders, and coordinating with physicians, physical therapists, and case managers. Between scheduled medication passes and charting windows, the nurse responds to call lights, manages pain, troubleshoots IV pumps, educates families, and watches for subtle changes in condition that signal deterioration. The documentation burden is significant: every assessment, every intervention, and every patient conversation must be logged in real time to meet regulatory and legal standards. For a useful contrast, consider what a typical nurse educator day looks like.
Settings and How Daily Life Varies
RNs practice across a spectrum of environments, and the job changes shape accordingly. Hospital nurses work rotating shifts, often including nights, weekends, and holidays, in high-acuity units where patient turnover is constant. Outpatient clinic nurses see scheduled appointments during business hours, manage chronic disease follow-up, administer infusions, and triage phone calls. Home health RNs drive to patients' houses, conducting assessments and teaching caregivers in living rooms and kitchens, with greater autonomy and less immediate backup. School nurses balance first aid, medication administration, health screenings, and crisis intervention for hundreds of students, often as the sole healthcare provider on campus.
Physical and Emotional Demands
The work is physically taxing: RNs spend most of their shifts on their feet, lifting and repositioning patients, pushing equipment down long hallways, and responding to codes that demand bursts of adrenaline-fueled activity. The emotional load is equally real. Nurses absorb patients' fear and families' grief, navigate end-of-life conversations, and carry the weight of clinical decisions made under time pressure and incomplete information. Burnout rates are high, particularly in understaffed units, and the combination of shift work, moral distress, and compassion fatigue influences long-term career satisfaction and attrition. These pressures are a key reason behind the ongoing nursing faculty shortage, as fewer experienced clinicians transition into teaching roles.
Specialization Within a Clinical Scope
RNs can specialize in dozens of areas (critical care, operating room, oncology, pediatrics, emergency medicine), but the core scope remains bedside and clinical. An ICU nurse manages ventilators, vasoactive drips, and continuous hemodynamic monitoring for one or two critically ill patients. An OR nurse circulates during surgery, maintaining sterile technique and anticipating the surgeon's needs. An oncology nurse administers chemotherapy, monitors for infusion reactions, and provides psychosocial support through grueling treatment cycles. Regardless of specialty, the registered nurse's primary role is direct patient care, not teaching, policy development, or curriculum design.
What Does a Nurse Educator Do?
Two distinct career paths carry the nurse educator title, and understanding how they differ is the first step in deciding which direction fits you.
Academic Nurse Educator: The Faculty Role
Academic nurse educators work in colleges and universities, preparing the next generation of nurses through classroom instruction, simulation lab facilitation, and clinical rotations. The role of nurse educator in this setting is broader than many expect. A typical week runs 45 to 55 hours and spans several kinds of work:1
- Direct teaching: Lecturing, leading seminars, and running simulation scenarios account for roughly 25 to 35 percent of weekly time.
- Clinical supervision: Overseeing students in hospital and community placements takes another 20 to 30 percent.
- Preparation and grading: Curriculum design, lesson planning, and evaluating student work fill 15 to 25 percent of the schedule.
- Advising and mentoring: One-on-one student support and academic advising make up 5 to 10 percent.
- Administrative and service work: Faculty committees, accreditation tasks, and departmental meetings consume 10 to 20 percent.
- Scholarship and research: Depending on the institution type, scholarly work ranges from essentially none to about 15 percent of the workload.
Direct hands-on patient care drops to 0 to 10 percent, compared to the 80 to 90 percent a bedside RN spends in direct patient contact.1 That shift is the defining structural difference. For a deeper comparison of these two tracks, see our guide on academic vs clinical nurse educator roles.
Clinical Nurse Educator: The Staff Development Role
Clinical nurse educators, sometimes called nurse professional development specialists, are hospital and health system employees. Their nurse educator responsibilities center on onboarding new staff, delivering in-service training, ensuring regulatory compliance, and rolling out policy changes. The schedule is closer to a standard 40-hour work week without the evening or weekend shifts common in bedside nursing. About 10 to 30 percent of their time still involves direct patient care situations, primarily during competency validation or when demonstrating procedures at the bedside.1
Program development and quality improvement work take up 15 to 25 percent of their time, while administrative duties and meetings account for another 10 to 20 percent.
The Thread That Connects Both Paths
What neither role strips away is clinical expertise. Academic faculty draw on years of practice every time they explain a clinical scenario to a student. Clinical educators use that same knowledge to coach a new graduate nurse through a procedure for the first time. If you recognize yourself in that mentoring instinct, you may already be showing signs you should become a nurse educator. The nurse educator is not leaving nursing. The job is making sure nursing knowledge travels from one generation to the next, through teaching, mentoring, and deliberate practice rather than direct bedside care.
Questions to Ask Yourself
Education and Certification Requirements Compared
The educational paths for bedside nursing and nursing education share a common starting point, but they diverge sharply once you decide to step into a teaching role.
The RN Path
Becoming a registered nurse requires either an Associate Degree in Nursing (ADN) or a Bachelor of Science in Nursing (BSN), followed by passing the NCLEX-RN licensure exam. Many nurses also complete an RN-to-BSN program after working in clinical practice for a few years. That foundation is excellent for patient care, but it is not enough on its own to land most academic teaching positions.
Moving Into Nurse Education: What Degree Do You Need?
A common question nurses ask is whether a BSN is sufficient to work as a nurse educator. The short answer: it depends on the role. Some clinical educator positions within hospital systems, and occasional adjunct or skills lab roles at community colleges, will hire a BSN-prepared nurse who brings substantial hands-on experience. However, most full-time academic positions require an MSN at minimum, and that bar keeps rising. Tenure-track faculty roles at four-year universities increasingly expect a DNP or a PhD in nursing, particularly as accreditation bodies push programs to elevate their faculty credentials.
If academic education is your goal, planning for an MSN with a nursing education concentration is the practical floor. You can explore affordable online nurse educator MSN programs to compare costs and timelines. That typically adds two to three years of study beyond your BSN, which is worth factoring into your timeline and budget before comparing salaries. The return on that investment gets covered later in this article.
CNE Certification from the NLN
The National League for Nursing offers the Certified Nurse Educator (CNE) credential, the recognized specialty certification in this field.1 To sit for the CNE exam, candidates must hold a master's or doctoral degree in nursing. There is no pathway for BSN-only applicants to earn this credential.2
Eligibility falls into two options:
- Option A: A graduate degree in nursing plus at least 9 credit hours of graduate-level nursing education coursework (note that research or statistics courses do not count toward this requirement).2
- Option B: A graduate degree in nursing plus two years of teaching experience within the past five years, with no specific coursework requirement.2
The CNE is a voluntary specialty certification. Most universities and hospital systems list it as preferred rather than required when hiring, but holding it signals a serious commitment to the educator role and can strengthen your candidacy meaningfully.1 For nurses weighing the CNE against the newer clinical certification, our CNE vs. CNEcl certification comparison breaks down the differences.
For nurses working in practical or vocational nursing education specifically, the NLN introduced the CNEpv credential in 2026.3 That pathway accepts a baccalaureate degree or higher in nursing, combined with three years of nursing experience and two years of teaching experience within the past five years, making it accessible to educators in LPN/LVN programs who do not hold a graduate degree.3
Salary and Job Outlook: RN Vs. Nurse Educator
The table below compares national salary benchmarks and employment figures for Registered Nurses, Nursing Instructors and Teachers (Postsecondary), and Nurse Practitioners. Nurse Practitioner data is included because many nurses weighing an educator path also consider the NP route, and a side-by-side comparison helps clarify the financial trade-offs. All figures are drawn from the most recent BLS Occupational Employment and Wage Statistics (May 2024 data year) and should be treated as approximate. Projected growth rates cover the 2024 to 2034 decade. Notably, postsecondary nursing instructors are projected to grow at roughly 17%, well above the average for all occupations, reflecting ongoing demand for qualified faculty to train the next generation of nurses. Registered Nurses, meanwhile, are expected to add about 166,100 new positions over the same period at a 5% growth rate, and Nurse Practitioners continue to be one of the fastest-growing occupations in healthcare.
| Occupation | National Median Salary | 25th Percentile | 75th Percentile | Total Employment (2024) | Projected Job Growth (2024 to 2034) |
|---|---|---|---|---|---|
| Registered Nurses | $93,600 | $78,610 | $107,960 | 3,282,010 | 5% (about 166,100 new jobs) |
| Nursing Instructors and Teachers, Postsecondary | $79,940 | $62,210 | $102,020 | 74,250 | 17% |
| Nurse Practitioners | $129,210 | $109,940 | $149,570 | 307,390 | N/A |
Highest-Paying States for Nursing Instructors
Geography matters when it comes to nurse educator pay. The table below ranks the top 10 states by median annual salary for Nursing Instructors and Teachers, Postsecondary, and places each alongside the median RN salary in the same state so you can see the real earning trade-off. In several high-paying states, nurse educators actually out-earn bedside RNs, while in others the gap favors clinical practice. Employment totals also reveal where demand is strongest. All figures are from the most recent BLS Occupational Employment and Wage Statistics.
| State | Nursing Instructor Median Salary | Nursing Instructor Employment | RN Median Salary (Same State) | Instructor vs. RN Difference |
|---|---|---|---|---|
| California | $99,010 | 6,120 | N/A | N/A |
| Texas | $97,610 | 5,940 | $90,010 | +$7,600 |
| New York | $93,640 | 5,380 | N/A | N/A |
| Alaska | $92,050 | 190 | N/A | N/A |
| Nevada | $84,660 | 920 | N/A | N/A |
| Montana | $84,550 | 230 | N/A | N/A |
| Florida | $83,940 | 4,990 | N/A | N/A |
| Delaware | $83,420 | 250 | $92,610 | −$9,190 |
| North Dakota | $83,130 | 120 | N/A | N/A |
| Connecticut | $81,490 | 1,160 | N/A | N/A |
Should I Be a Nurse or a Teacher? Choosing the Right Path
The tension most people feel here is not really between nursing and teaching as separate careers. It is between two versions of the same impulse: wanting to care for people and wanting to shape how others learn to do that. Nurse education is where those two drives converge, and understanding the practical tradeoffs helps you decide whether the timing is right for you.
Lifestyle and Schedule
Bedside nursing is physically demanding work built around 12-hour rotating shifts, weekend rotations, and holiday coverage. Nurse educators, whether in academic or clinical nurse educator roles, generally work closer to a standard weekday schedule, with academic faculty often experiencing lighter loads during summer and intersession periods. The physical wear of years on your feet, lifting patients, and managing high-acuity emergencies is real, and it accumulates. A move into education does not eliminate stress, but it changes the texture of it considerably.
Emotional labor is present in both roles. Educators carry the weight of students struggling with licensure, skill gaps, and career uncertainty. Clinical nurses absorb patient suffering, family grief, and the moral distress that comes with understaffed units. Neither path is emotionally easy, but the nature of the weight differs.
Burnout: What the Numbers Actually Show
Burnout in nursing has reached crisis levels. Recent data puts the national burnout rate for nurses at 76 percent as of 2025.1 Roughly 60 percent of acute care nurses report burnout and 75 percent report high stress.2 Nearly 40 percent of registered nurses say they intend to leave their current position, and among those, more than 41 percent cite burnout as the reason.3
Nurse educators are not immune. A systematic review found that about 85 percent of nursing faculty reported moderate to high burnout, with a mean overall burnout score of 59.28.4 However, the same data shows a meaningful personal accomplishment score of 32.16, which reflects a sense of meaning and contribution that many clinical nurses struggling with understaffing and moral injury report losing. The profile of educator burnout tilts more toward workload and role overload than toward the emotional exhaustion and depersonalization that dominate bedside burnout.
The ROI of Making the Transition
Pursuing an MSN to move into education takes time and money, typically two to three years of study alongside clinical work. That investment is real. But many academic institutions offer tuition remission as a faculty benefit, which can offset a significant portion of the cost if you pursue a doctoral degree afterward. If cost is a concern, exploring affordable nurse educator DNP programs can help you map out realistic options. The physical longevity factor matters too: careers in education simply place less wear on the body, which has compounding value over a 15- to 20-year horizon.
The question is not whether bedside nursing or nurse education is harder. It is which kind of challenge fits the life you want to build, and whether you are ready to invest in the credential that opens the door.
Related Articles
Nurse Educator Vs. Nurse Practitioner: How They Differ
One pathway shapes the next generation of nurses; the other expands the reach of direct patient care. Both roles begin with a Master of Science in Nursing (MSN), yet they lead to fundamentally different professional identities. Choosing between them means deciding whether your passion lies in the classroom and curriculum or the exam room and treatment plan.
Scope of Practice and Daily Responsibilities
The starkest contrast emerges in what each professional does hour by hour. Nurse educators design courses, deliver lectures, run simulation labs, mentor students, and assess competency.1 They shape curricula and ensure that the nursing workforce enters practice ready to provide safe, effective care. In contrast, nurse practitioners (NPs) function as advanced practice registered nurses, conducting physical exams, diagnosing conditions, prescribing medications, ordering and interpreting tests, and managing whole episodes of care.2 NPs often serve as primary care providers, especially in underserved areas.
Both roles draw on deep clinical knowledge, but the nurse educator translates that knowledge into formative experiences. The NP applies it directly to patient outcomes. If you thrive on one-on-one patient interaction and clinical decision-making, the NP route aligns with that drive. If you're energized by watching a student grasp a difficult concept or master a skill, education may be the better fit.
Typical Employers and Settings
Nurse educators work predominantly in academic institutions: university nursing schools, community colleges, hospital-based diploma programs, and online education platforms. Many also maintain a clinical nurse educator role, supervising students in hospitals or clinics, which provides a bridge to patient care without being the primary provider. NPs are found in a much broader array of clinical settings, including private physician practices, retail health clinics, hospitals, community health centers, specialty clinics, and increasingly telemedicine.2 The employment footprint reflects the fundamental difference: one serves the learners, the other the patients.
Education and Certification Requirements Compared
- Entry-level degree: Both roles require an MSN at minimum, though a growing number of educators and NPs pursue a Doctor of Nursing Practice (DNP) or a PhD.
- Licensure and certification: Nurse educators typically hold an RN license plus specialty certification such as the Certified Nurse Educator (CNE) credential. They may also need state-specific teaching authorization. NPs must hold an RN license, earn national certification in a population focus (e.g., family, adult-gerontology), and obtain advanced practice licensure from their state board. NPs must also meet continuing education and recertification requirements to maintain prescriptive authority.
The educational path for a nurse educator often includes coursework in curriculum design, assessment, and teaching strategies, while the NP curriculum emphasizes advanced pathophysiology, pharmacology, health assessment, and clinical hours in a chosen specialty.1
Salary and Career Trajectory
National compensation data highlights a significant earnings gap. As of 2024, the median annual wage for nurse practitioners was $132,050, reflecting the high demand for advanced clinical providers.2 Nurse educators earned a median of $67,983 nationally.3 You can explore a deeper breakdown of nurse educator salary trends to see how experience, setting, and degree level affect pay. The wage difference mirrors the clinical specialization and billing capacity of NPs, whereas educator salaries are tied to academic pay scales and grant funding.
Job growth projections tell a similar story of opportunity, but for different reasons. NP employment is projected to surge 35% from 2024 to 2034, fueled by an aging population and emphasis on primary care access.2 Nurse educator roles were projected to grow 6% from 2018 to 2028, with demand driven by faculty retirements and the need to expand nursing school enrollment.3 Both paths offer stability, but the NP role currently has far more openings and faster projected expansion.
Making the Choice: Educator or Clinician?
The decision often comes down to your core motivation. Nurse educators measure success in graduation rates, NCLEX pass percentages, and the clinical readiness of new nurses. NPs measure it in improved patient outcomes, chronic disease management, and community health metrics. If you leave a shift energized by teaching moments and curriculum innovation, education is calling. If you're fulfilled by complex clinical reasoning and long-term patient relationships, the NP path may be your best fit. Both build the nursing profession, just from very different angles.
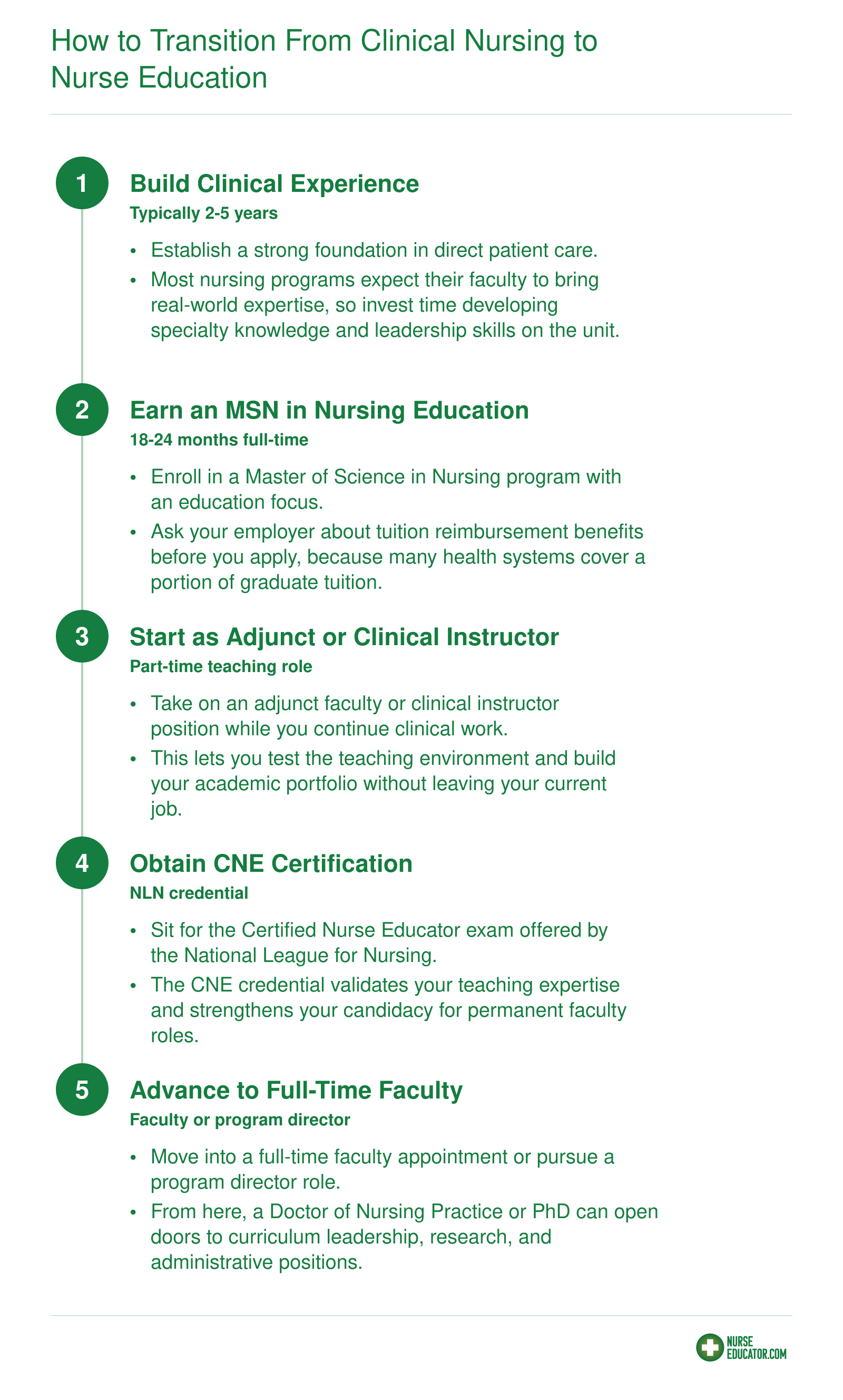
How to Transition From Clinical Nursing to Nurse Education
Many nurses get their first taste of teaching by precepting nursing students or mentoring new hires on the unit. That informal experience is a strong signal that the educator path may be right for you. When you are ready to make it official, the transition follows a fairly predictable sequence, and some hospitals even offer tuition reimbursement for MSN programs, which can significantly lower the financial barrier to entry.
Frequently Asked Questions
These are the questions nurses most often ask when weighing a move into education. Each answer draws on the salary data, scope comparisons, and credentialing details covered earlier in this article.