What you’ll learn in this article…
- Pediatric dosing errors occur at roughly three times the rate of adult errors.
- Hybrid simulation models measurably improve student competency over clinical hours alone.
- Structured pre-clinical preparation seven to ten days out cuts first-shift safety errors.
A nursing student preparing to assess a 4-year-old in respiratory distress and one preparing to assess a 70-year-old in the same situation are not doing the same job. Developmental stage, weight-based dosing, family dynamics, and a patient who cannot reliably report their own symptoms create a clinical environment that requires a fundamentally different skill set and a fundamentally different teaching strategy.
This gap between adult and pediatric practice shows up clearly in online nursing communities. Discussions in spaces like the r/StudentNurse subreddit reveal that peds rotations generate persistent anxiety around medication calculations, communicating with parents, and assessing children who cannot cooperate with standard protocols. That anxiety is a signal: students are not receiving enough structured preparation before they walk onto a pediatric unit.
Pediatric dosing errors occur at roughly three times the rate of adult medication errors, a disparity rooted in weight-based calculations and narrow therapeutic margins. For nurse educators, that statistic is not a caution label. It is a curriculum design problem that evidence-based preparation, active learning strategies in nursing, and deliberate evaluation can solve.
Why Pediatric Clinical Rotations Require a Specialized Approach
Pediatric clinical rotations are the structured, hands-on experiences where nursing students apply their knowledge in real-world child health settings, from inpatient units to school-based clinics. Unlike adult medical-surgical rotations, where a standardized head-to-toe assessment generalizes across most patients, pediatric placements demand a fundamentally different framework. Caring for patients who range from fragile neonates to independent adolescents means that a one-size-fits-all approach simply does not work. This section explores why these rotations require a specialized playbook, grounded in developmental science, national competency standards, and the evolving landscape of pediatric care delivery.
The Developmental Continuum Changes Everything
In adult nursing, baseline physiologic norms and communication strategies remain relatively stable across patients. In pediatrics, the nurse must recalibrate every interaction based on the child's developmental stage. A toddler's pain assessment relies on behavioral scales like FLACC, while an adolescent can use a numeric rating. Vital sign interpretation shifts dramatically: a heart rate of 130 that is normal for an infant becomes a red flag in a school-age child. Even the approach to medication administration requires age-specific calculations, from weight-based dosing to verifying safe ranges that vary with growth. This developmental lens does not just alter clinical tasks; it transforms how students build trust, explain procedures, and involve families. Without deliberate preparation, students default to adult-centric habits that fall short in the pediatric world.
National Competency Standards and Pediatric-Specific Outcomes
National frameworks reinforce that clinical judgment in nursing pediatrics is not an optional add-on but a distinct competency. The AACN's 2021 Essentials explicitly require that prelicensure graduates demonstrate competence across the lifespan, including pediatric populations, within all four spheres of care.1 Rather than prescribing minimum pediatric hours, the Essentials focus on achieving specific outcomes, allowing flexibility in how programs meet them.1 State boards of nursing may set additional requirements,2 and the NLN similarly recognizes that pediatric competencies develop through a blend of direct care and simulation.3 Importantly, while simulation can supplement pediatric learning, it cannot fully replace direct clinical interactions in this age group.3 These standards make it clear that educators must design rotations that ensure every student encounters the unique challenges of child health, from family-centered communication to recognizing subtle deterioration in a non-verbal patient.
Fewer Beds, More Intentional Placements
Compounding the complexity, the national decline in pediatric inpatient beds is shrinking the traditional pipeline of clinical sites. Many hospitals have consolidated pediatric services, leaving fewer beds and shorter stays, and post-pandemic shifts have accelerated this trend. As a result, educators can no longer assume that a block rotation on a general pediatric floor will automatically expose students to the breadth of conditions they need. This scarcity makes intentional rotation design more critical than ever: coordinating with outpatient clinics, schools, and community health partners, and integrating high-fidelity simulation to fill gaps. For clinical coordinators, the message is clear: creativity in site selection and tight alignment with learning objectives are what will produce competent, confident pediatric nurses.
This article is written first for nurse educators and clinical coordinators who build and oversee these experiences. However, students preparing for their first pediatric clinical will also find actionable insights to enter the rotation with greater confidence and awareness of what makes this specialty uniquely demanding and rewarding.
Clinical Site Selection: Matching Settings to Learning Objectives
Choosing the right clinical site is one of the most consequential decisions a nurse educator makes when designing a pediatric rotation. The setting you select shapes everything from the acuity of cases students encounter to the quality of mentorship they receive, so the match between site and learning objective deserves careful, deliberate thought.
Start by mapping your program's competency framework to specific care environments. A general pediatric medical-surgical unit offers breadth: students see a wide range of diagnoses, practice medication calculations for weight-based dosing, and develop comfort communicating with caregivers alongside their young patients. Pediatric emergency departments, by contrast, demand rapid assessment and triage skills, making them better suited for advanced students who have already consolidated foundational clinical judgment. Specialty units such as pediatric oncology or the neonatal intensive care unit provide depth, but the emotional complexity and technical demands can overwhelm students who arrive without adequate preparation.
When evaluating prospective sites, look beyond bed count and reputation. Key criteria include:
- Staff-to-student ratios that allow meaningful supervision without overburdening unit nurses
- Preceptors who hold (or are willing to pursue) formal clinical educator preparation
- Patient volume sufficient to guarantee hands-on experiences rather than observation-only shifts
- Institutional willingness to integrate students into interdisciplinary rounds and family-centered care conferences
- Clear policies on student scope of practice that align with your state board requirements
Relationship-building with site coordinators is ongoing work, not a one-time agreement. Schedule regular check-ins with unit managers and charge nurses to surface logistical friction early. Students who feel welcomed and purposefully placed in a unit perform better and report higher confidence after the rotation.
Finally, consider diversifying placement across at least two different settings within a single pediatric rotation when your curriculum allows. Pairing a community pediatric clinic with an acute-care unit, for instance, exposes students to both preventive and episodic care, reinforcing the full continuum of pediatric health. innovative teaching strategies in nursing education can help you structure those varied experiences into a coherent arc that builds complexity progressively, rather than leaving students to piece together the big picture on their own.
Questions to Ask Yourself
Preparing Students Before the First Shift
Pediatric rotations reward students who show up prepared and rattle those who don't. A structured pre-clinical week, ideally seven to ten days before the first patient contact day, dramatically reduces first-shift anxiety and safety errors. Build the preparation into required coursework rather than leaving it to student initiative.
The Pre-Clinical Knowledge Checklist
Assign a review packet students must complete and self-verify before Day 1. At minimum, it should cover:
- Vital sign ranges by age: Heart rate, respiratory rate, and blood pressure norms for neonates, infants, toddlers, preschoolers, school-age children, and adolescents. Require students to memorize these, not just look them up.
- Growth and development milestones: Erikson's stages paired with age-appropriate communication strategies. A student who knows a three-year-old is in the autonomy stage will offer choices rather than issue commands.
- Pain assessment tools: FLACC for preverbal children, Wong-Baker FACES for ages three and up, and the numeric scale for older school-age and adolescent patients. Students should be able to state which tool fits which age without hesitation.
- Family-centered care principles: The core idea that the child and caregiver are a single unit of care, and that parents are partners rather than visitors.
The Self-Assessment Step
Require a short pre-rotation self-assessment asking students to rate their comfort with children, identify any personal anxiety triggers (crying infants, medical trauma histories, end-of-life pediatric cases), and note prior pediatric exposure. Use the responses to shape assignments. A student rattled by infant procedures may start on a general pediatric floor rather than the NICU or PICU. This is not coddling, it is targeted nursing student stress management that builds confidence before high-stakes encounters.
Orientation and Shadowing
Before the first patient day, schedule students to shadow a child life specialist for two to four hours or attend a formal pediatric unit orientation. Watching a child life specialist prepare a four-year-old for an IV start teaches distraction, developmental communication, and therapeutic play more effectively than any lecture. Nursing students frequently discuss how disorienting how to prepare nursing students for first clinical moments feel when pediatric norms differ sharply from adult units, and building this orientation step directly into your course structure addresses that gap before it becomes a patient safety concern.
Practical Logistics
Send a supply list: stethoscope with a pediatric diaphragm (adult bells miss subtle findings on small chests), a penlight, and small distraction tools such as stickers, bubbles, or a light-up toy. Review the site's dress code (many peds units restrict certain prints or accessories) and clarify infection control expectations, which are typically stricter than adult units given RSV, pertussis, and varicella exposure risks.
Age-Specific Assessment and Pediatric Medication Safety
Pediatric dosing errors occur at roughly three times the rate of adult errors, and weight-based calculations are the single most common failure point students bring into clinical.1 Building age-specific assessment fluency alongside disciplined medication math is the core teaching task of any pediatric rotation.
Assessment Techniques by Developmental Stage
Assessment in pediatrics is not one skill but four, each demanding a different approach. Students need explicit coaching on what changes across the age continuum.
- Infants: Palpate the anterior fontanelle for bulging or sunken contours, count respirations for a full minute before disturbing the baby, and assess tone and reflexes while the infant is calm in a parent's arms.
- Toddlers: Expect resistance. Teach the toe-to-head sequence, save invasive checks (ears, mouth) for last, and use the parent's lap as the exam table. Distraction tools, offering choices, and demonstrating on a stuffed animal all reduce distress.
- School-age children: Most will cooperate with a straightforward, honest explanation. Let them handle the stethoscope. Address them directly, not just the parent.
- Adolescents: Privacy is clinical, not optional. Offer time alone with the nurse, respect gowning preferences, and normalize confidential screening for risk behaviors within legal limits.
Weight-Based Dosing and the Math Students Get Wrong
Every pediatric medication order must include the patient's weight in kilograms, and students should be taught to refuse to proceed without it. Drill the mg/kg calculation as a three-step ritual: verify weight, calculate the ordered dose, then cross-check against a reference safe dose range.3 The predictable student errors are decimal misplacement, unit confusion (grams vs milligrams, pounds vs kilograms), and using the wrong concentration when a drug comes in multiple strengths. Active learning strategies in nursing can sharpen how these failure modes are taught before students ever reach a patient bedside. Simulation scenarios built specifically around weight-based dosing errors, wrong concentration, and decimal errors expose thinking gaps before a real patient is involved.4
High-alert medications, including opioids, insulin, anticoagulants, and chemotherapy agents, demand an independent double-check by a second qualified nurse, plus barcode verification and smart pump confirmation before administration.3 Teach students that the double-check is independent: the second nurse recalculates from the order, not from the first nurse's math. Medication reconciliation before the first dose, except in emergencies, is another non-negotiable step students must internalize.5
Competency Before Clinical
Embed a standardized dosage calculation quiz into pre-clinical requirements with a firm minimum passing score, commonly 90 percent, before a student may pass any pediatric medication in the clinical setting.4 Pair the quiz with OSCEs and scenario-based written exams, and require reflection on any near-miss the student witnesses or contributes to.4 Frame near-miss reporting as non-punitive learning, mirroring the safety culture students will need to build in practice.3 When educators encounter persistent gaps, Plan-Do-Study-Act (PDSA) cycles offer a structured method for refining how medication safety competencies are taught and assessed over time.4
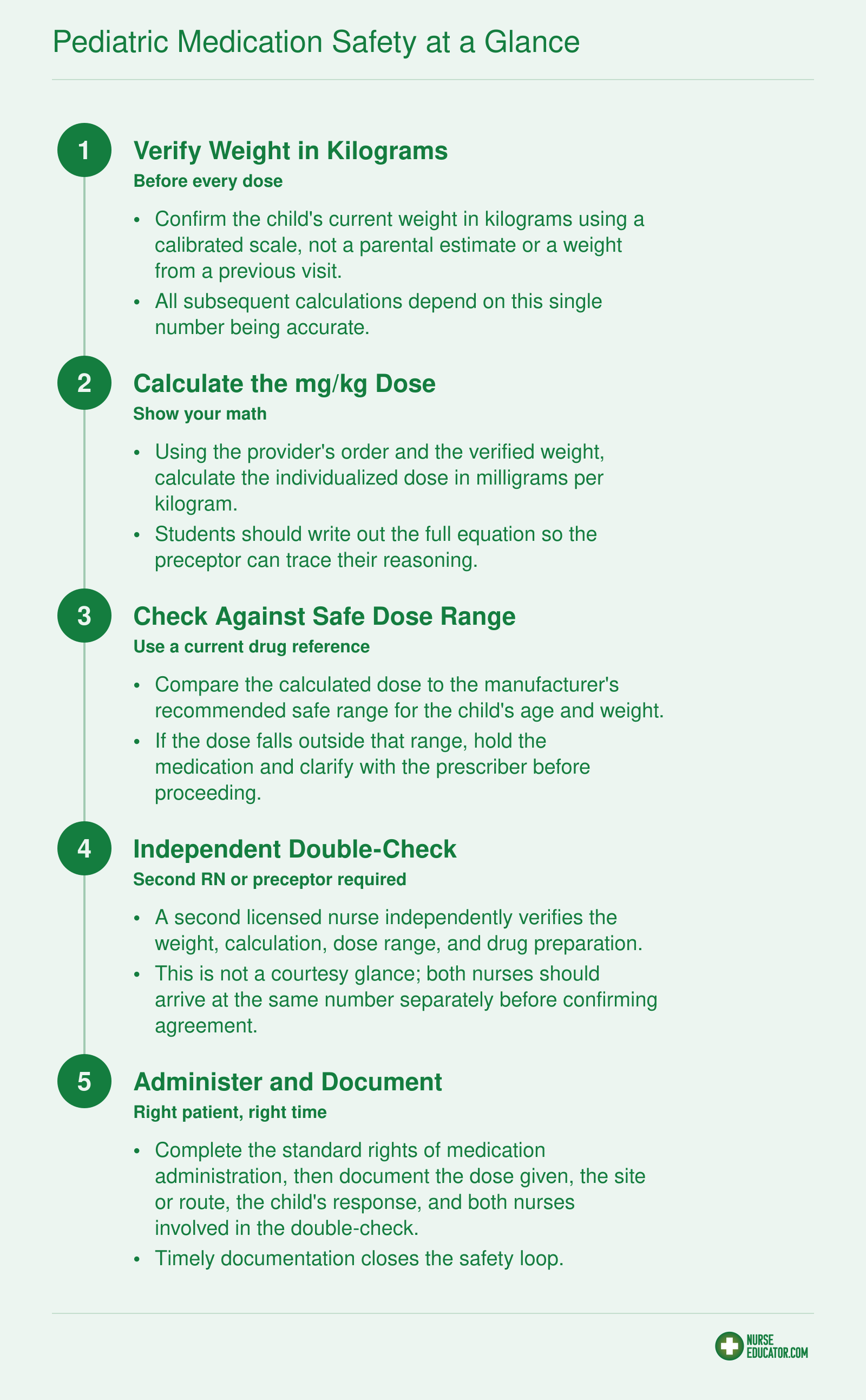
Pediatric Medication Safety at a Glance
Every pediatric medication pass carries higher risk than its adult counterpart because of weight-based dosing, smaller margin for error, and patients who cannot always self-advocate. Before your students touch a syringe in a pediatric setting, make sure they have internalized this five-step workflow. Post it in your simulation lab, review it during pre-clinical huddles, and expect students to verbalize each step during competency check-offs.
Communicating With Families: Teaching Family-Centered Care
Family-centered care has moved from an aspirational philosophy to a measurable competency in pediatric nursing education, yet many programs still treat effective family communication as something students either "have or don't." That assumption shortchanges learners. Communication with parents, guardians, and extended family members is a teachable, practicable skill, and nurse educators who approach it with the same rigor they apply to clinical procedures will see better outcomes on the unit and in student confidence.
Concrete Strategies That Build Competence
Four teaching approaches work especially well when preparing students for the realities of pediatric family interactions.
- Role-play with standardized family members: Recruit trained actors or fellow faculty to portray specific parent personas (anxious first-time parent, a medically savvy guardian questioning the care plan, a non-English-speaking grandparent) so students practice adapting their approach before they face the real thing.
- SBAR handoff practice that includes family concerns: Modify your SBAR template so students must explicitly document and relay the family's stated worries or preferences during handoff. This trains them to treat family input as clinical data rather than background noise.
- Reflective journaling after difficult interactions: Ask students to write a structured journal entry following any encounter that felt emotionally charged. Prompts such as "What did the parent need that I initially missed?" and "How would I approach this conversation differently?" turn a single experience into a durable lesson.
- Guided debriefing in post-clinical conference: Dedicate time each week for the group to discuss a family communication challenge one student faced. Peer feedback normalizes the difficulty and surfaces strategies students might not discover on their own.
Preparing for the Full Spectrum of Family Dynamics
Students will encounter families across a wide emotional and cultural range. Some parents are processing a first-ever hospitalization and need frequent reassurance. Others arrive with extensive medical knowledge and will push back on proposed interventions. Families in acute crisis, whether from a new diagnosis or a trauma admission, may express fear as anger or withdrawal. Non-English-speaking families require students to coordinate interpreter services and rely more heavily on nonverbal cues. Reviewing clinical communication strategies for ESL nursing students before clinical orientation gives students a practical framework for those encounters.
Educators should map these scenarios explicitly in pre-clinical orientation rather than waiting for students to stumble through them. Even a brief lecture that names and normalizes these dynamics reduces the freeze response many students experience the first time a parent challenges their assessment.
Balancing Partnership with Professional Boundaries
Teaching students to view parents as partners in care does not mean encouraging them to share every detail of clinical reasoning or defer to family wishes that conflict with evidence-based practice. The goal is transparent, respectful communication within the student's scope. Encourage students to use phrases like "I want to make sure your concerns are part of our plan" while also modeling how to say "Let me bring that question to the supervising nurse so we can give you the most accurate answer."
This balance is where educator modeling and the qualities of a good nurse educator matter most. When you round with students, demonstrate how you acknowledge a parent's expertise about their own child while still guiding clinical decisions. Then debrief what you did and why. Students internalize boundaries far more effectively when they watch a skilled educator navigate them in real time than when they read about them in a textbook.
In pediatric care, the parent or caregiver is your second patient. Students who learn to assess parental anxiety alongside the child's vitals consistently perform better in clinical evaluations and build stronger therapeutic rapport. Teach your students to read the room, not just the chart.
Integrating Simulation Into Pediatric Clinical Education
Clinical-only models versus simulation-enhanced models: for decades, nursing programs relied almost entirely on hospital placements to build pediatric competency. Today, the evidence points clearly toward a hybrid approach that combines real clinical hours with structured simulation experiences, and the outcomes for students are measurably better.
High-Fidelity Scenarios That Build Real Competency
Not every simulation scenario translates equally well into pediatric nursing education. The ones that consistently produce strong learning outcomes tend to mirror the high-stakes, time-sensitive situations students will actually encounter on a pediatric unit. Four scenarios stand out as particularly effective:
- Acute asthma exacerbation: Students practice rapid assessment, bronchodilator administration, and escalation decisions while managing a child who is visibly distressed and a frightened parent asking questions.
- Febrile seizure management: This scenario builds skill in recognizing seizure activity, maintaining airway safety, administering rescue medications, and communicating calmly with caregivers during and after the event.
- Dehydration assessment in an infant: Students learn to integrate subtle clinical signs, including skin turgor, fontanelle status, mucous membrane moisture, and urine output history, into a coherent clinical picture before recommending intervention.
- Medication error recognition: A scenario in which an order contains a weight-based dosing error forces students to pause, verify, and speak up, directly reinforcing the safety habits that pediatric medication administration demands.
These scenario types align with categories identified in recent simulation literature, including acute emergencies, medical-surgical situations, neonatal presentations, and family-centered discharge planning.1
What the Research Says
A 2024 review of high-fidelity simulation in pre-licensure nursing programs found consistent improvements in student self-efficacy, reductions in clinical anxiety, and gains in active learning strategies nursing when simulation was integrated alongside traditional placements.2 Separately, a 2024 interprofessional pediatric simulation training study reported that 95 percent of participants rated the experience as excellent or good, and 99 percent said they would recommend it to colleagues.3 While these findings come from varied contexts and should be interpreted with appropriate caution rather than as universal guarantees, the direction of the evidence is encouraging.
On the structural side, a 2024 review noted that some state boards and accrediting bodies now permit simulation to replace up to 50 percent of required clinical hours, provided programs meet established quality benchmarks.2 The National League for Nursing supports this model, and INACSL Standards of Best Practice serve as the primary benchmark for programs seeking to meet accreditation expectations.1
Debriefing: Where the Learning Actually Happens
Simulation without structured debriefing is a missed opportunity. Two frameworks work especially well in pediatric contexts. Debriefing for Meaningful Learning (DML) uses a Socratic questioning style that asks students to reflect on their clinical reasoning rather than just their actions. The PEARLS framework (Promoting Excellence and Reflective Learning in Simulation) blends self-assessment with facilitated discussion and direct instruction, making it flexible enough to use with both novice and more advanced students.
Faculty facilitating pediatric simulation should complete formal simulation educator training before leading high-fidelity scenarios. Programs that lack the budget for full manikin-based setups have practical alternatives: tabletop simulations using case cards and physical props can replicate decision-making pressure at a fraction of the cost, and nursing simulation software features now include pediatric-specific modules that students can access independently outside of lab hours.
The goal, regardless of the platform or fidelity level, is to give students a chance to make decisions, experience consequences in a safe environment, and reflect deliberately before they encounter the same situations at the bedside.
Evaluation Methods and Clinical Performance Criteria
How do you fairly and consistently evaluate nursing students in pediatric clinical rotations when the competencies, patient populations, and care settings differ so much from adult practice?
Selecting the right evaluation instruments and building criteria around pediatric-specific skills are two of the most impactful decisions a nurse educator can make. A poorly matched rubric leaves students confused about expectations and gives faculty little actionable data. Here is how to approach clinical placement evaluation for nursing students with both rigor and clarity.
Choose Validated Instruments That Fit Pediatric Practice
Several well-established tools can be adapted for pediatric rotations.
- Lasater Clinical Judgment Rubric: Originally designed for simulation debriefing, this rubric has been applied successfully to virtual pediatric scenarios and supports student self-evaluation, making it useful for both formative feedback and reflective practice.1
- Creighton Competency Evaluation Instrument (C-CEI): Built around clinical judgment dimensions, the C-CEI translates well to pediatric settings when faculty map its behavioral anchors to child-specific care activities.
- QSEN-Based Pediatric Nursing Clinical Evaluation Instrument: Developed at The College of New Jersey, this 40-item tool is grounded in QSEN competencies and boasts strong content validity (scale-level content validity index of 0.985 using the averaging method).2 It was purpose-built for pediatric rotations, so the alignment with age-specific care is already built in.
- AACN/QSEN Clinical Evaluation Tools: Scored on a 0-to-4 numeric scale across QSEN knowledge, skills, and attitudes, these tools total 100 points and map directly to AACN BSN Essentials.3
Other frameworks organize evaluation by clinical domains. The Miami Dade College pediatric evaluation tool, for instance, clusters criteria into Assessment, Managing Care, Clinical Decision Making, and Caring Interventions,4 while a Springer Publishing tool uses a six-point frequency scale (from "always" to "never") across domains including collaboration, differential diagnosis, and interpersonal skills.5
Build Criteria Around Pediatric-Specific Competencies
Whichever instrument you select, make sure your criteria capture what makes pediatric nursing distinct:
- Age-appropriate communication (talking to a toddler is not the same as interviewing an adolescent)
- Application of growth-and-development principles to assessment and care planning
- Family-centered care delivery, including the ability to partner with parents and caregivers
- Safe medication administration with accurate weight-based dosage calculations
When students can see these competencies spelled out on their evaluation form before the rotation begins, they know exactly where to focus their energy.
Balance Formative and Summative Strategies
Relying solely on an end-of-rotation competency sign-off is a missed opportunity. A structured midpoint check-in gives students time to course-correct while stakes are still low. During that formative conversation, use specific behavioral examples: "During your assessment of the 4-year-old with croup, you used distraction techniques effectively but did not verbally confirm the weight-based dose with the RN before administration." That level of detail is far more useful than a generic "needs improvement."
Summative evaluation at the end of the rotation should then confirm whether the student meets competency thresholds across all pediatric-specific domains. Tools such as reflective journaling, SOAPIE documentation review, and clinical tracking logs can supplement direct observation and round out the picture.6
Tackle Inter-Rater Reliability Head-On
When multiple preceptors evaluate the same student across different clinical sites, scoring inconsistencies are almost inevitable. A few practical steps can minimize the problem:
- Hold a calibration session before the rotation starts where all evaluators score the same recorded student scenario and compare results.
- Use rubrics with clearly defined behavioral anchors rather than vague descriptors like "satisfactory" or "competent."
- Designate a lead faculty member to review all evaluations and flag outlier scores for follow-up discussion.
- Incorporate tools designed for direct observation, such as Mini Clinical Evaluation Exercises or Direct Observation of Procedural Skills, which standardize what the evaluator watches for in real time.7
Consistent, transparent evaluation protects students from subjective bias and gives nurse educators defensible data when making progression decisions. The time invested in selecting the right tools and training evaluators pays dividends in student trust and program credibility.
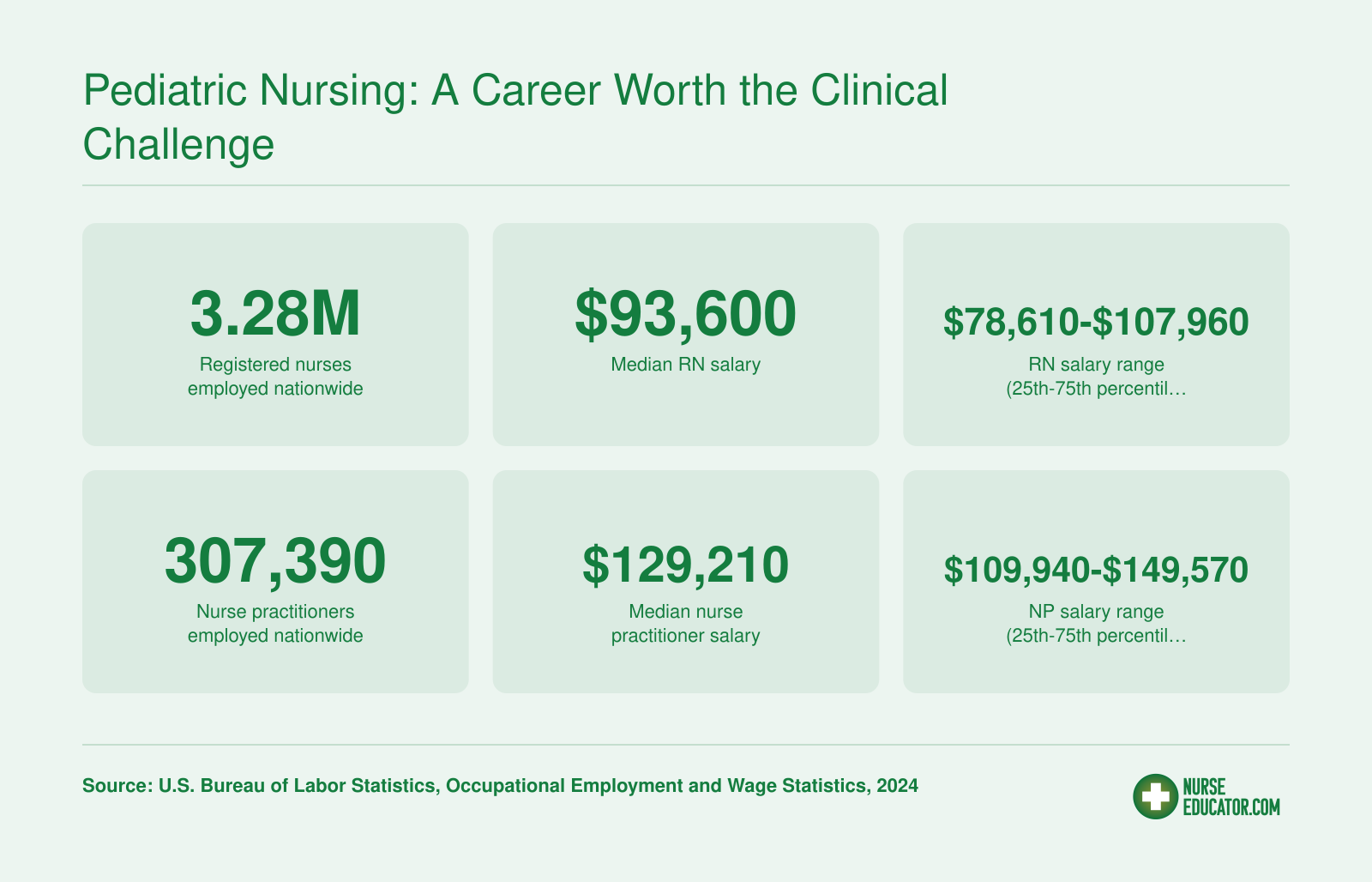
Pediatric Nursing: A Career Worth the Clinical Challenge
Strong pediatric clinical training positions graduates for success in a profession that continues to grow in both demand and earning potential. Whether your students pursue bedside RN roles or advance to nurse practitioner practice, the labor market rewards clinicians who enter the workforce well prepared. These national figures underscore why investing in rigorous pediatric rotations pays off for educators and students alike.
Common Challenges and How Educators Can Address Them
Pediatric clinical rotations consistently present unique challenges that require proactive faculty intervention and creative solutions. Understanding these obstacles and implementing evidence-based strategies ensures students gain the competencies they need despite real-world constraints.
Declining Pediatric Inpatient Census
Many clinical sites have experienced reduced pediatric inpatient volumes over the past decade, creating competition for limited placement slots. Shorter hospital stays and the shift toward ambulatory care mean fewer patients are available for traditional bedside experiences. Educators can address this by diversifying clinical partnership models for nursing education to include pediatric specialty clinics, school health offices, home health agencies, and community health centers. Negotiating agreements with multiple sites allows rotation of smaller student groups and expands the variety of pediatric conditions students encounter. Professional organizations such as the National League for Nursing and the American Association of Colleges of Nursing regularly publish guidance on navigating placement shortages and developing alternative clinical models that maintain educational rigor while adapting to healthcare delivery trends.
Student Anxiety and Confidence Building
Working with children often triggers heightened anxiety in nursing students, particularly around medication administration, assessment of nonverbal patients, and family interactions. Faculty can mitigate this by scheduling high-fidelity simulation sessions before the first clinical day, using pediatric mannequins that replicate age-specific vital signs and responses. Pre-rotation workshops on developmental milestones, communication techniques, and medication dosage calculations build foundational confidence. During clinical days, pairing students with experienced pediatric nurses for the initial shifts provides role modeling and real-time coaching. Debriefing sessions after each clinical day allow students to process emotional responses and reframe challenging encounters as learning opportunities. Educators who also attend to nursing student mental health support during high-stress rotations report stronger student engagement and lower attrition.
Limited Hands-On Participation
Some pediatric units restrict student involvement due to patient acuity, family preferences, or institutional policies. When direct care opportunities are scarce, faculty should emphasize observation with structured reflection assignments. Students can shadow multidisciplinary rounds, observe procedures through simulation or video, and complete case studies based on patients they observe rather than directly care for. State boards of nursing and nursing education discussion forums offer documented strategies for ensuring clinical competency even when participation is constrained. Alternative experiences such as pediatric simulation labs, virtual reality scenarios, and standardized patient encounters can supplement limited bedside hours, ensuring students meet program outcomes and regulatory requirements for pediatric nursing competencies.
Frequently Asked Questions About Pediatric Clinical Rotations
Pediatric clinical rotations raise practical questions for both new nurse educators and the students they mentor. Below are answers to the most common questions, grounded in the frameworks and strategies covered throughout this guide.