What you’ll learn in this article…
- The National Nurses United argues that the nurse shortage is actually a crisis of retention and unsafe working conditions.
- Over 1.15 million actively licensed RNs are not practicing, representing a massive untapped workforce for re-entry programs.
- Nursing schools had 1,588 unfilled faculty positions in 2025-26, worsened by a pay gap with clinical nursing.
- Nursing curricula must now embed advocacy skills to prepare nurses to fight for safe staffing and retention.
Why are more than a million actively licensed registered nurses not working as RNs? National Nurses United asserts the ‘shortage’ is actually a retention crisis, pointing to 1.15 million non-practicing RNs in 20251, a workforce larger than many states’ entire nursing pool. For nurse educators, this reframes the mission: producing new graduates is not enough. Curricula must now embed advocacy, resilience, and policy literacy so students can thrive amid chronic understaffing. Workforce data, curriculum shifts, and policy implications converge on a single demand: training nurses who can both deliver care and fight for the conditions that make it sustainable.
The Controversy: Is There Really a Nursing Shortage?
Hospitals frame the issue as a critical shortage of nurses; a major nursing union counters that the real crisis is one of retention, not supply. This debate has profound implications for nurse educators.
Two Contrasting Narratives
On one side, hospital associations and health systems warn of a dangerous gap in the nursing workforce, pointing to vacancy rates and burnout-driven turnover. On the other, National Nurses United (NNU) asserts there is no shortage of nurses, only a shortage of nurses willing to work under current conditions.1 Their stance shifts the focus from recruitment to workplace safety, adequate staffing, and morale.
The Numbers Tell a Different Story
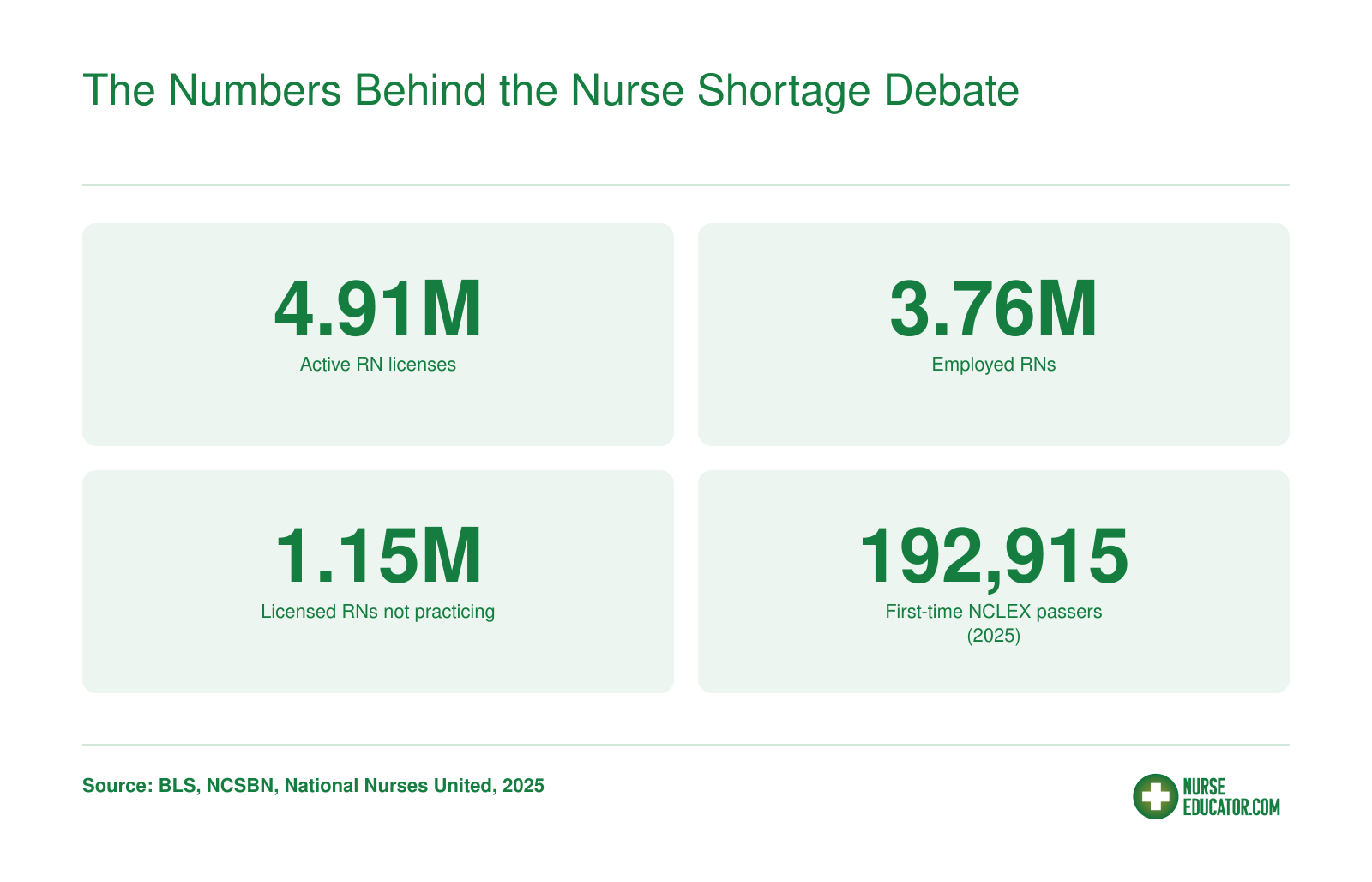
Data from recent years supports the union's perspective. As of May 2025, the U.S. had 4.91 million actively licensed registered nurses, according to the National Council of State Boards of Nursing. Yet only 3.76 million were employed as RNs, leaving 1.15 million license holders not working at the bedside. That is nearly one out of every four licensed nurses choosing to stay away from direct patient care. The Bureau of Labor Statistics confirms these figures, underscoring that the issue is not a lack of qualified professionals, but a refusal to participate in a system many view as broken.
A Strong Pipeline, But an Exodus
Meanwhile, the education pipeline is robust. In 2025, 192,915 first-time U.S.-educated candidates passed the NCLEX-RN exam, a significant rise from 157,206 in 2016. Nursing schools are producing more graduates than ever, yet the workforce continues to hemorrhage talent. This paradox suggests that simply graduating more nurses will not solve the problem; instead, the exodus of licensed nurses from the profession demands new strategies.
What This Means for Nurse Educators
For faculty and program leaders, these facts reframe the mission. If the pipeline is functioning, education must pivot from scaling up enrollments to fostering nurse educator burnout prevention, professional advocacy, and career-sustaining skills. Curricula should equip students to navigate and improve workplace conditions, recognize burnout, and advocate for safe staffing. By doing so, educators can help bridge the gap between the number of licensed nurses and those actually practicing, ultimately strengthening the entire healthcare system.
The Numbers Behind the Nurse Shortage Debate
A closer look at the workforce data reveals a surprising picture: millions of licensed nurses are ready to work but are not at the bedside. These figures suggest a retention crisis, not a supply problem.
From Pipeline to Retention: Rethinking the Educator's Role
For decades, the nursing education community has operated with a pipeline mindset: recruit more students, graduate more nurses, and the shortage will solve itself. The data tells a different story. NCLEX pass rates are strong, and the number of newly licensed RNs has grown from 157,206 in 2016 to 192,915 in 2025. Yet hospitals remain understaffed, and both nurse turnover and the nurse educator shortage remain stubbornly high. The real issue is not supply; it is retention. As an educator, your greatest impact may not come from increasing enrollment, but from reshaping how students think about their careers and their power to change workplace culture.
The Reality of the 'Shortage': It's a Retention Crisis
National turnover among hospital RNs reached 17.6% in fiscal year 20252, but that average masks wide variation; some facilities lose more than 40% of their nursing staff annually2. Among first-year nurses, the rate climbs to 22.7%2, and for Gen Z nurses it sits at 25%4. Specialty areas are hit even harder: behavioral health units report 22.5% turnover2, emergency services 20.7%2, and intensive care units globally see 23%3. These exits are not simply a matter of career changes or retirement. According to National Nurses United's 'There Is No Nurse Shortage' report, only 59% of retired nurses said their departures were planned, and a February 2026 JAMA Network survey of over 4,000 RNs found adequate staffing to be the top factor (65%) that would draw them back. The same analysis highlights a staggering imbalance: 4.91 million RNs hold active licenses, yet only 3.76 million are employed in nursing, leaving 1.15 million qualified professionals on the sidelines.
The underlying drivers are well documented. Emotional stress is now the top reason nurses cite for leaving their jobs4, followed closely by insufficient staffing and the “reality shock” that new graduates experience when they hit the floor4. A 2022 survey of acute-care nurses found that 60% reported burnout5 and 75% reported high stress5, and more than half (52%) expressed intent to leave their current position5. This churn comes with a steep patient safety cost: on understaffed units, patient mortality risk increases by 6%5. The narrative of a “nurse shortage” can obscure this retention emergency, and educators have a critical role in correcting the story.
Shaping the Nurse of Tomorrow: Advocacy and Resilience
Nursing curricula have traditionally focused on clinical judgment, pathophysiology, and technical skills, with little formal attention to the workplace dynamics that drive nurses out. To change that, educators can embed advocacy skills and the principles of teaching emotional intelligence and resilience to nursing students into their programs. This does not mean a single lecture on self-care; it means teaching students to:
- Recognize early signs of burnout in themselves and colleagues, distinguishing normal stress from moral injury caused by systemic constraints.
- Advocate for safe staffing using evidence and collegial communication strategies, so they enter practice ready to speak up during huddles or unit governance meetings.
- Build professional resilience through structured reflection, peer support networks, and an understanding of organizational resources before they ever experience a crisis.
Role-playing difficult conversations and debriefing clinical experiences through the lens of workplace conditions are concrete strategies. When students learn that burnout is not an individual failing but a predictable result of under-resourcing, they are more likely to seek institutional solutions rather than silently leaving the bedside.
Tapping the Untapped: Re‑Engaging Inactive Nurses
With 1.15 million licensed RNs not currently employed in nursing, even modest improvements in working conditions could draw many back. Many of them left due to the same conditions that drive current turnover. Educators can contribute to this re-engagement by designing re‑entry refresher courses that address contemporary practice challenges and by equipping new graduates with the skills to become workplace change agents. When today’s students enter practice ready to constructively push for safe staffing and supportive cultures, they help build the kind of workplaces that could draw skilled nurses back into the profession, making a genuine dent in the staffing crisis without relying solely on new graduate production.
Related Articles
Questions to Ask Yourself
Building Resilience and Advocacy Into Nursing Curricula
Nurse educators today must do more than impart clinical knowledge; they must equip students with the tools to sustain a career and change broken systems. The AACN Essentials Domain 10 emphasizes personal, professional, and leadership development, providing a framework for integrating well-being and advocacy into every nursing program.
Recognizing Burnout and Building Personal Resilience
Burnout begins before the first job. Many programs now introduce resilience training during orientation. For example, one nursing school described in My American Nurse (2024)1 implemented a commercial resilience program at orientation to reduce early burnout. The AACN's Developing Nursing Well-Being and Leadership Tool Kit offers faculty ready-made resources for teaching self-care, mindfulness, and stress management.2 Simple modules on sleep hygiene, reflective journaling, and peer support groups can be woven into existing courses without adding credit hours.
But resilience cannot stop at the individual. Students must learn that burnout often stems from unsafe workloads, not personal weakness.
Empowering Students to Advocate for Safe Staffing
Negotiation and communication skills are rarely taught, yet they are essential. Educators can design role-play scenarios based on real workplace conflicts: for instance, a nurse requesting additional staff for a unit that has exceeded safe limits. These exercises build confidence to speak up. The AONL's 2026 advocacy priorities include the Save Healthcare Workers Act3, highlighting legislative efforts students should understand. When students role-play contacting legislators or testifying at hearings, they see advocacy as a professional obligation.
Curriculum Models in Action
The AACN's Well-Being and Resilience Initiative recommends routine mental health screenings and nursing student mental health support, normalizing help-seeking.2 Columbia Nursing's Climate Crisis Session teaches policy dissemination and storytelling, skills easily adapted to staffing advocacy.4 Students learn to craft a compelling narrative about a staffing failure and its impact on patient safety. A 2024 review of climate resilience in nursing education (PMC13275279)5 underscores the importance of embedding systems-level thinking; the same approach works for workplace safety.
From Simulation to System Change
Simulation labs and clinical debriefs are perfect arenas to reinforce resilience and advocacy. After a high-fidelity simulation, facilitators can ask, "What system issues contributed to this situation? How would you advocate for a different outcome?" Debriefs shift focus from individual error to team and environmental factors. Pair this with faculty mentorship that models advocacy, and students graduate ready to not just survive but transform their workplaces.
The Pay Gap That Drives the Faculty Shortage
Nursing educators earn less than clinical RNs despite requiring advanced degrees. This pay gap deters nurses from entering academia, fueling the faculty shortage.
Re-Engaging the 1.15 Million Non-Practicing RNs
The most overlooked resource in the nurse shortage debate is a staggering 1.15 million registered nurses who hold active licenses but are not practicing. These are experienced clinicians who stepped away for family, burnout, career changes, or other reasons. Rather than solely focusing on producing new graduates, nurse educators have an opportunity to design re-entry pathways that recapture this latent workforce. Targeted programs can update skills, restore confidence, and address the working conditions that pushed nurses out in the first place.
Models That Work: What the Data Show
Nationwide, well-structured nurse re-entry programs demonstrate consistent success, with 70 to 75 percent of participants returning to practice.1 Most programs combine 10 to 15 weeks of didactic coursework with 120 to 160 hours of supervised clinical experience, often completed over three to six months.1 For example, the University of Delaware's RN Refresher runs a 15-week online didactic component over a six-month period. In North Carolina, the AHEC RN Refresher Program has graduated more than 400 nurses in three years, achieving a 75 percent job placement rate.1 A Rutgers University study found a 70.2 percent return-to-practice rate among participants.1 A hospital-partnered refresher model priced at $2,399, with scholarships available, completes in just 10 weeks, proving that compressed, affordable options are feasible.1
Designing Re-Entry Programs as an Educator
Nurse educators are uniquely positioned to lead these initiatives. They understand the curriculum gaps that returning nurses face, particularly in electronic health records, telehealth, and evidence-based practice. Beyond clinical knowledge, re-entry programs must address emotional readiness. Many non-practicing nurses left due to moral distress or burnout; a supportive mentorship component, built into the clinical hours, can rebuild professional identity. Temporary licenses, valid for six months in many states like Georgia4, and through reentry programs such as the Foothills AHEC RN Reentry Program, provide a legal bridge while skills are refreshed.
Collaboration with healthcare facilities is essential. Educators can partner with hospitals to design clinical rotations that mirror current practice, ensuring returning nurses are not simply placed in overburdened units but are gradually reintegrated with preceptor support. This also lets educators influence workplace culture by embedding safe staffing principles into the re-entry curriculum.
A Win-Win for Staffing and the Profession
Re-entry programs serve a dual purpose: they ease the staffing crisis while honoring the investment already made in seasoned professionals. For healthcare organizations, re-engaging existing licensees is faster and more cost-effective than recruiting new graduates. For nurses, it offers a structured, dignified path back to a career they may have thought was lost. Educators who champion these programs position themselves as architects of workforce solutions, not just classroom instructors. The 1.15 million inactive RNs represent not a failure of the education pipeline, but a reservoir of talent waiting for the right opportunity to return.
Why There's a Shortage of Nurse Educators: Faculty Vacancy Crisis by State
The nursing faculty shortage left 1,588 budgeted but unfilled faculty positions in the 2025-2026 academic year1. That translates to a national vacancy rate of 7.2% out of 21,993 total budgeted positions, but the challenge is sharper in some regions: 8.3% in the West, 8.2% in the South, compared to 4.9% in the Midwest. State-level data reveals even steeper shortages in certain program types. In Texas, graduate nursing programs reported a 15.4% vacancy rate, with vocational nursing programs experiencing a staggering 28.5% turnover rate among faculty.2
The Salary Gap That Keeps Expertise at the Bedside
A primary driver of the faculty shortage is the stark salary disparity between academic and clinical roles. Nurse faculty earned a median annual wage of $87,000 in 2024, while advanced practice registered nurses (APRNs) in clinical practice brought in $120,000, creating a gap of $30,000 to $35,000.3 For experienced clinicians considering a transition to teaching, this pay cut is often prohibitive. Combined with heavy teaching loads, advising responsibilities, and the pressure to publish, the academic pathway simply cannot compete financially with hospital or private practice settings. Additionally, the requirement for a doctoral degree in many tenure-track positions creates another barrier, as nurses must invest years of additional education while already working.
A Faculty Workforce Approaching Retirement
The aging profile of nurse educators adds urgency. The average age of doctorally prepared faculty is 61.2 years, and for master's prepared faculty it is 55 years.4 A third of all nurse faculty were projected to retire by 20253, meaning that even as schools scramble to hire replacements, a wave of departures is already underway. This demographic cliff threatens to deepen the vacancy crisis unless succession planning and expedited pathways into academia are prioritized. Without deliberate mentorship programs, newer faculty who do enter the field often face heavy course loads and isolation, which drives turnover.
The Ripple Effect of the Clinical Retention Crisis
The broader retention crisis in nursing amplifies the faculty shortage. If bedside nurses are exiting the profession early due to unsafe staffing and burnout, as recent workforce data suggests, the pool of experienced clinicians who might eventually pivot to teaching is shrinking. The same working conditions that push nurses out of hospitals also make the idea of staying in healthcare, even in education, less appealing. Addressing the educator shortage, then, isn't just about training more PhDs; it requires systemic improvements in clinical environments so that seasoned nurses want to stay in the profession long enough to pass on their expertise. By connecting the dots between clinical retention and faculty recruitment, we see that solutions must tackle the root causes of dissatisfaction on both fronts: compensation, workload, and respect.
We don't have a nurse shortage; we have a shortage of safe working conditions that drives experienced nurses out of the profession. That is the real crisis.
Policy Implications: Safe Staffing and Working Conditions
Nurse educators hold a unique lever for systemic change: by instilling policy literacy in every student, they transform the nursing workforce from within.
Why Retention Depends on Safe Staffing
A growing consensus among researchers reframes the so-called nursing shortage as a retention crisis driven by poor working conditions. Data from more than 4,000 nurses in 10 states, reported in a February 2026 JAMA Network analysis, confirms: nurses are not leaving because they lack skills or calling; they are leaving because they cannot practice safely.
For nurse educators, this reframes the central challenge. Instead of simply producing more graduates to fill vacancies, education programs must equip students to advocate for the conditions that make staying in nursing viable. When students grasp the evidence linking staffing ratios to patient outcomes and career longevity, they enter practice as agents of change, not passive participants.
From Classroom to Capitol: Teaching Policy Literacy
Policy advocacy cannot be an afterthought in nursing curricula. Students need concrete skills: how to track legislation, contact elected officials, join professional organizations, and speak at public hearings. Several states, including California and Massachusetts, have passed safe staffing laws in response to sustained nurse-led campaigns. These victories illustrate that change is possible when nurses organize around data and share their frontline experiences.
Educators can weave policy content into existing courses. A clinical debrief, for example, might discuss how staffing levels affected patient care that day; a leadership assignment can ask students to draft a letter to a legislator. Using active learning strategies, educators can normalize advocacy as a core nursing competency, as essential as medication administration or infection control.
Preparing Nurses for a Career-Long Advocacy Journey
Systemic retention demands a workforce that continually pushes for accountability; it is not a one-time fix. Nurse educators are uniquely positioned to plant that seed. By teaching students to interpret workforce data, recognize the signs of moral distress tied to understaffing, and engage in collective action, faculty help build a profession that can sustain itself. The 1.15 million licensed RNs not currently practicing represent a latent force. Policy-literate nurses can help design re-entry programs and lobby for the conditions that would bring them back.
Ultimately, the debate over whether a shortage exists misses the point. What matters is that educators prepare nurses to create workplaces where people want to work. That starts with policy literacy, taught early and reinforced throughout the curriculum.
Frequently Asked Questions About the Nurse Shortage
Nurse educators often field questions about the shortage. Below are common questions with guidance on where to find reliable, up-to-date information.
The so-called nursing shortage is a retention crisis: 1.15 million inactive RNs prove that nurses are leaving because of working conditions, not a lack of qualified graduates. The way forward starts in the classroom. Nurse educators must embed advocacy, resilience, and re-entry pathways into curricula, preparing students to fight for safe staffing and sustainable careers. Systemic change demands that academia, hospitals, and policymakers unite around retention, not just recruitment. By shaping nurses who are equipped to stay and to lead, educators can build a profession that no one wants to leave.