What you’ll learn in this article…
- Research pooling over 171,800 nursing students found depression, anxiety, and burnout rates well above the general college population.
- Active recall and spaced repetition tools like Anki outperform passive review and help students balance personal pressures with academics.
- Faculty trained in Mental Health First Aid can identify warning signs early, yet most nursing programs still lack formal training requirements.
- Programs embedding counseling, peer support, and mental health literacy report lower attrition rates and stronger NCLEX outcomes.
Nursing students report depression at rates roughly two to three times higher than the general college population, yet most faculty receive no formal training on how to recognize or respond to mental health distress in the classroom or clinical setting. That gap between prevalence and preparedness is widening as programs grow larger, clinical placements grow more demanding, and students arrive carrying more complex personal circumstances.
A post that surfaced recently in the r/StudentNurse community illustrated this vividly: a 27-year-old student navigating an RN-to-BSN path, a long-term relationship, a partner's teenage child, and ambitions toward an MD, all at once. That layered reality is not unusual. Many nursing students are managing family obligations and relationship dynamics alongside coursework that would be taxing on its own.
This is a practical guide for nurse educators, not a clinical literature review. What follows covers prevalence data, early warning signs, faculty training frameworks, accommodation policies, program-level support models, and concrete resources educators can use today. The data alone makes a compelling case: mental health support is now a core function of nursing education, not an ancillary service.
The Scope of the Problem: Depression, Anxiety, and Burnout Rates Among Nursing Students
High Prevalence of Mental Health Conditions
Nursing students consistently report mental health concerns at rates that exceed those of the general college population. A 2024 umbrella review of 25 meta-analyses, pooling data from 375 primary studies and over 171,800 nursing students worldwide, found that about 27% experience an overall mental health problem, with specific conditions affecting large segments: depression (29%), anxiety (29%), burnout (32%), and stress (27%).1 Sleep disturbances affect half of students surveyed (50%), and fear is reported by 41%.1 These figures highlight a pervasive challenge across nursing programs.
Comparison to General Student Populations
While college students nationally struggle with mental health, nursing students often fare worse. National surveys of undergraduates typically report depression rates around 20% and anxiety around 25%, but the umbrella review shows nursing students at 29% for both.1 Burnout, which encompasses emotional exhaustion and reduced personal accomplishment, is particularly pronounced among nursing students due to the rigorous combination of academic coursework and clinical training. The pressures mirror what faculty themselves face, a dynamic explored in depth in resources on nurse educator burnout prevention.
Post-Pandemic Trends and At-Risk Subgroups
The post-pandemic period has seen an increase in mental health symptoms among nursing students. The stress of clinical placements, fear of making errors, and balancing personal responsibilities (such as career changes or family expectations) have intensified. Subgroup analyses suggest that students in accelerated or second-degree programs, those who are older or career changers, and those in the thick of clinical rotations may report higher distress. A 2024 study from Mexico found that 15.2% of 433 nursing students, primarily young women (mean age 20), exhibited suicidal risk, underscoring the severity for certain demographics.2 Building emotional intelligence in nursing classrooms can help educators recognize warning signs earlier.
Barriers to Seeking Help
Despite high prevalence, many nursing students do not seek mental health care. Stigma within the profession, fear of appearing unfit, and concerns about licensure or clinical clearance frequently prevent students from accessing support. This gap leaves educators with a critical role in early identification and referral.
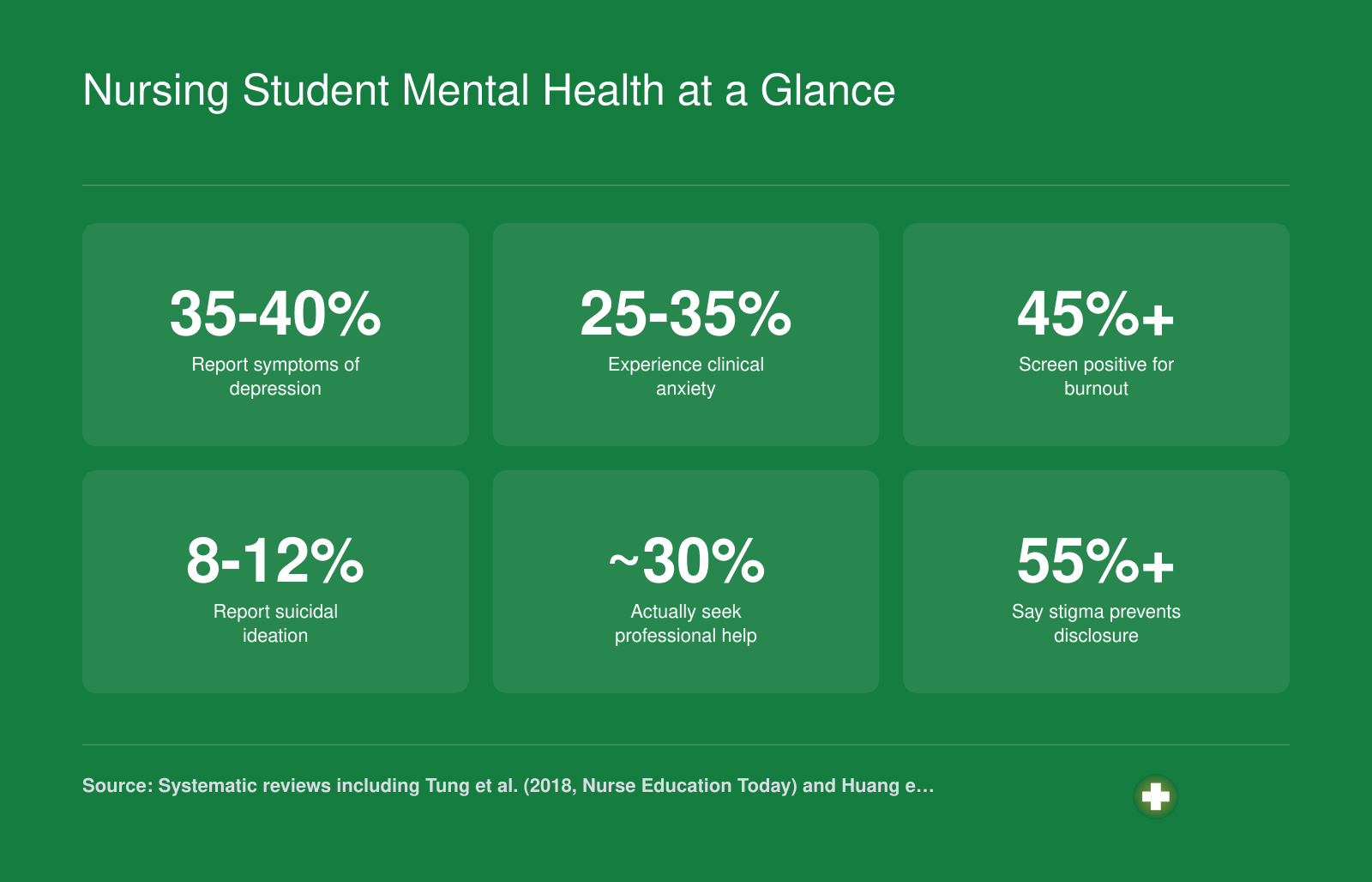
Nursing Student Mental Health at a Glance
Research consistently shows that nursing students experience mental health challenges at rates above the general college population. These figures underscore why faculty training and proactive support systems are not optional extras but program essentials.
Why Nursing Students Face Unique Mental Health Stressors
Nursing students face a constellation of stressors that are fundamentally different from those experienced by students in other fields, stressors that directly threaten mental health and require educator awareness if we are to retain compassionate, capable professionals.
Clinical Placement Trauma: The Weight of the Bedside
Classroom simulations cannot fully prepare a student for the first time a patient dies under their care, or the moment they witness a code blue that ends badly. Clinical placements thrust learners into high-acuity settings where they encounter ethical dilemmas, family conflict, and the raw edges of human suffering while still building clinical judgment in nursing. These are precisely the experiences that contribute to secondary traumatic stress and compassion fatigue, phenomena rarely faced by students in non-healthcare disciplines. Nursing students carry the emotional residue of patients they lose and scenes they cannot forget, often processing this weight in silence because they believe it is part of the professional hardening process. Without structured debriefing or faculty acknowledgment of this emotional load, distress becomes internalized, raising risks for anxiety and depression.
Personal Life Pressures and Competing Identities
Many nursing students are career changers juggling complex personal lives while enrolled in demanding programs. A recent post in r/StudentNurse captured this tension vividly: a 27-year-old with a BA in history, working toward an RN before starting a BSN and eventually an MD, described feeling unmoored while also navigating a relationship with a partner who has a 13-year-old child.1 The writer shared confusion about life outside school, balancing academic goals with the needs of a blended household and long-term career plans across multiple degree stages. This is not an outlier; it is the norm in many cohorts. Students managing children, partnerships, elder care, or financial pressures while enrolled in a program that tolerates little schedule flexibility often find themselves choosing between self-care and survival, eroding mental wellness over time.
Academic Rigor and the NCLEX Shadow
The sheer density of nursing curricula creates a pressurized environment. Students must master didactic content, skills competencies, and hundreds of clinical hours simultaneously, all under the looming shadow of the NCLEX. High-stakes testing culture fosters perfectionism and fear of failure, which can trigger or amplify anxiety disorders. Unlike many disciplines where a single exam may represent partial credit, nursing students know that a failed dosage calculation or a critical safety lapse can end a clinical rotation. The related stigma around academic failure in nursing students compounds this pressure significantly. This threat, while necessary for public protection, operates as a chronic stress amplifier. When combined with early morning clinicals, rotating shifts, and limited time for sleep or exercise, the academic grind becomes a direct pathway to burnout.
Faculty and Peer Incivility as a Hidden Stressor
Research on nursing education consistently identifies incivility, dismissive, humiliating, or exclusionary behavior from faculty or classmates, as a significant contributor to psychological distress. A student who is belittled in post-conference or undermined during a skills check carries that hurt into patient interactions and clinical decision-making. For students already vulnerable due to preexisting mental health conditions, a single incident of incivility can destabilize months of coping work. Incivility fractures the sense of belonging that is protective against burnout, leaving students isolated at the very moment they most need connection and mentorship.
Questions to Ask Yourself
Recognizing Warning Signs: What Educators Should Watch For
Faculty are often the first adults in a nursing student's academic world to notice something is wrong, yet most nursing programs provide little formal training on what to look for. That gap matters, because early identification consistently improves student outcomes across every mental health condition common in this population.
From Clinical Symptoms to Classroom Behaviors
You are not reading a DSM entry when you observe your students, and you should not try to. What you can do is translate the general signs of depression, anxiety, and burnout into the observable patterns that show up in your classroom and clinical rotations.
- Academic decline: A student whose grades drop sharply over two or three consecutive weeks, especially without a clear external cause like illness, deserves a private check-in.
- Attendance changes: Repeated absences or chronic lateness, particularly when the student previously showed up reliably, are worth noting.
- Withdrawal from peers: Students who stop participating in group work, avoid clinical huddles, or sit apart from cohort members they used to engage with are showing a behavioral shift.
- Emotional flatness or irritability in clinical settings: A student who seems disconnected from patients, snaps at staff, or appears unable to engage emotionally during care may be running on empty rather than being difficult.
Normal Stress Versus a Concerning Pattern
Every nursing student experiences stress. The differentiators are frequency, duration, and functional impairment. One rough week before a pharmacology exam is normal. Six weeks of declining performance, missed simulation labs, and tearful conversations with classmates is a pattern. Ask yourself whether the behavior is isolated or recurring, whether it is affecting the student's ability to function in multiple settings, and whether it has persisted beyond a single stressor event.
The Notice, Name, Navigate Framework
A practical micro-framework can guide your response without requiring clinical training.
- Notice: Observe and document the specific behavioral change, not a judgment about the student's character or ability.
- Name: Speak with the student privately and name your concern directly but warmly. Something like, "I have noticed you seem exhausted lately and I wanted to check in" opens the door without labeling.
- Navigate: Once the student feels heard, point them toward the appropriate resource, whether that is the campus counseling center, a student affairs advisor, or a peer support program. Follow up to confirm they connected.
Your Role Has Limits, and That Is by Design
Nurse educators are not therapists. Trying to counsel a student through a depressive episode or an anxiety disorder yourself can inadvertently delay proper care and create a relationship that is hard to walk back in a graded, supervisory context. The goal is early identification and a warm handoff to someone qualified to help. Knowing what makes a great nurse educator includes understanding where your expertise ends. Document what you observed, make the referral, and stay available as a supportive presence in the academic environment. Educators who also prioritize teaching emotional intelligence to nursing students often find it easier to create the trust that makes these conversations possible. That combination alone can make a meaningful difference.
Faculty Training for Mental Health Support in Nursing Programs
Most nursing faculty enter classrooms without any formal training to support students experiencing mental health crises, yet they are often the first to notice warning signs. Bridging this gap requires intentional faculty development, not ad hoc guesswork. The following training models offer evidence-based frameworks to equip educators with practical skills.
The Knowledge Gap in Nursing Education
Nursing programs train students to care for others, but the faculty who teach them rarely receive instruction on recognizing or responding to student mental health distress. Studies in higher education consistently show that fewer than one in five faculty members have completed any mental health literacy training. This gap leaves well-meaning instructors unprepared when students exhibit panic attacks, depressive episodes, or suicidal ideation. Placing the entire burden on individual faculty members to self-educate is both unrealistic and unfair; institutions must shoulder the responsibility of providing structured training that is woven into orientation and annual professional development calendars.
Evidence-Based Training Programs for Faculty
Several established training paths have gained traction in academic environments. While research specifically within nursing education is still emerging, the core competencies these programs build are directly transferable to clinical and classroom settings.
- Mental Health First Aid (MHFA): Offered by the National Council for Mental Wellbeing, MHFA is a 6- to 8-hour certification covering how to identify, understand, and respond to signs of mental illnesses and substance use disorders.1 Delivery options include in-person, blended, and virtual formats, and certification remains valid for three years. An instructor training track (three to five days) allows faculty members to become certified trainers for their own programs. A Youth MHFA variant, at six hours, suits educators working with younger cohorts. Evidence from college settings indicates that MHFA-trained faculty report increased confidence and a higher likelihood of intervening with struggling students. Its standardized action plan (ALGEE) provides a repeatable framework for clinical and academic contexts alike.
- Question Persuade Refer (QPR): QPR is a concise, evidence-based suicide prevention gatekeeper training typically completed in one to two hours. Faculty learn to recognize suicide warning signs, engage the student with direct questions, persuade them to seek help, and refer to appropriate resources. Its brevity makes it especially feasible as a required add-on during faculty orientation or clinical preceptor onboarding.
- Psychological First Aid (PFA): Developed by the National Child Traumatic Stress Network and the National Center for PTSD, PFA is an evidence-informed model for reducing initial distress after traumatic events. Though originally designed for disaster response, its principles (safety, calm, connectedness, self-efficacy, and hope) adapt well to the acute stress nursing students may encounter after a difficult patient outcome or a critical incident in clinical placements. Faculty trained in PFA can provide immediate, non-intrusive support and triage the need for further mental health services.
- Trauma-informed teaching frameworks: Rather than a single certification, these frameworks embed principles of safety, trustworthiness, choice, collaboration, and empowerment into pedagogy. For faculty seeking formal recognition, the International Board of Credentialing and Continuing Education Standards (IBCCES) offers a Student Mental Health Certificate, which requires two years of work experience, 14 hours of continuing education, and an exam.2 Initial certification costs $295, with renewal every two years (14 CE hours and a $149 renewal fee). While not specific to nursing education, the certificate signals a faculty member's commitment to mental health literacy and aligns with the holistic approach nurse educators value.
Critical Incident Stress Debriefing After Difficult Clinical Placements
Nursing students can witness death, severe trauma, or chaotic codes during clinical rotations, often for the first time. Without structured processing, these experiences can fuel anxiety, compassion fatigue, and burnout. Adapted from the emergency services model, Critical Incident Stress Debriefing (CISD) is a multi-phase, group-based session that allows participants to share facts, thoughts, and reactions in a safe environment. When facilitated by a trained clinician or a faculty peer, CISD can normalize distress and identify those needing additional support. A growing number of nursing programs are piloting post-clinical debriefing protocols that blend CISD elements with reflective practice, inviting students to process emotional responses alongside clinical decision-making. Formal training in debriefing is available through organizations like the International Critical Incident Stress Foundation, and even a two-day workshop can equip faculty to run low-intensity defusing sessions after particularly tough shifts. Building resilience in nursing students through structured debriefing also reinforces the emotional competencies they will need throughout their careers.
Institutional Responsibility and the Path Forward
Isolated training sessions without systemic backing will not close the gap. Nursing schools must treat faculty mental health training as an institutional responsibility, not an elective. This means embedding MHFA or QPR into onboarding, dedicating professional development days to trauma-informed teaching, and ensuring clinical faculty have access to debriefing resources. When institutions normalize these practices, they simultaneously model for students that mental health is a legitimate dimension of professional identity, a lesson as vital to nursing practice as any clinical skill. Programs already contending with a nursing faculty shortage can make mental health training part of their retention strategy, signaling to current and prospective faculty that the institution values their well-being alongside their expertise.
Related Articles
Program-Level Support Models That Actually Work
What concrete interventions have nursing programs implemented that measurably improve student mental health and retention? While many schools acknowledge the crisis, fewer have published outcome data on systematic support structures. A 2025 scoping review in *Frontiers in Psychiatry* examined 49 studies on mental health interventions for nursing students globally, identifying six broad categories of approaches.1 Separately, the CDC synthesized evidence from more than 25 nurse-led mental health programs for college students, published in *Preventing Chronic Disease*.2 Together, these reviews point to several models worth replicating, though rigorous outcome data remains limited.
Embedded Counseling and First-Semester Wellness Orientations
Some nursing schools have embedded licensed counselors directly within the program, offering drop-in hours in familiar clinical skills labs or simulation centers rather than requiring students to navigate campus-wide counseling services. This reduces stigma and increases utilization. Mandatory wellness orientations during the first semester introduce students to stress-management tools, normalize help-seeking, and establish rapport with support staff before crises emerge. If you are looking for ways to ease that initial transition, supporting nursing students first day sets the stage for year-long rapport. While systematic retention or NCLEX data tied specifically to embedded counseling models is not yet widely published, anecdotal program reports describe reduced mid-semester withdrawal rates and earlier identification of students in distress.
Structured Peer Mentoring Programs
Pairing senior and junior nursing students in formalized mentorship relationships creates a safety net beyond faculty oversight. Effective programs include training for mentors on active listening, boundary-setting, and when to escalate concerns to faculty or counseling services. Peer mentors normalize the emotional turbulence of clinical placements and share concrete coping strategies they themselves have tested. Some programs report improved first-year retention when mentorship is structured and sustained across semesters, though published effect sizes remain sparse.
Weekly Clinical Debriefing as Routine Practice
Small-group clinical debriefing should not be reserved for critical incidents alone. When scheduled as a weekly, structured practice at the end of every clinical day, debriefing normalizes emotional processing and builds psychological safety. Students learn to name difficult feelings, recognize shared stressors, and distinguish between normal adjustment and warning signs of burnout or depression. This practice requires minimal additional time (often 10 to 15 minutes) but signals that emotional work is as integral to nursing education as technical skills.
Mindfulness-Based Stress Reduction and Other Structured Interventions
Mindfulness-based stress reduction programs, typically delivered in six to eight sessions, have been studied in nursing student populations with mixed but generally positive results for self-reported stress and anxiety.1 These programs work best when offered during the academic term, not as optional summer add-ons, and when faculty model the practices themselves. Building that capacity often overlaps with teaching emotional intelligence to nursing students, because both require educators to demonstrate vulnerability and self-awareness. Other evidence-based interventions identified in the scoping review include cognitive-behavioral skill-building workshops, resilience training, and app-based mental health tools tailored to healthcare students.2
Start Small: One Implementable Change
Not every program can hire an embedded counselor or launch a campus-wide mentorship initiative immediately. Start with a single, low-cost practice: add a 10-minute post-clinical check-in at the end of each clinical day. Ask open-ended questions like "What surprised you today?" or "What felt hard?" and listen without rushing to problem-solve. This small ritual signals that students' emotional experiences matter and that seeking support is expected, not exceptional. Over time, this practice lays the foundation for more comprehensive program-level interventions.
Mental health infrastructure is not a luxury or compliance checkbox. Programs that invest in embedded counseling, peer support networks, and faculty mental health literacy consistently see lower attrition rates and stronger NCLEX outcomes. Treat wellness systems as core retention strategy, fund them accordingly, and measure their impact on student persistence alongside traditional academic metrics.
Accommodations, Policies, and Student Rights for Mental Health Conditions
Reasonable accommodations are specific adjustments to coursework, testing, scheduling, or clinical requirements that allow a student with a documented mental health condition to meet program standards without being penalized for symptoms outside their control. For nurse educators, understanding the legal framework behind these accommodations is not optional: it is a core part of running an equitable program.
Legal Protections: ADA and Section 504
Under the Americans with Disabilities Act (ADA) and Section 504 of the Rehabilitation Act, nursing students with documented mental health conditions are entitled to reasonable accommodations.1 Many conditions qualify as disabilities under these statutes, including major depression, generalized anxiety disorder, PTSD, and OCD. The legal standard requires institutions to provide accommodations unless doing so would impose an undue burden or fundamentally alter the nature of the program.
Critically, programs must evaluate each student through an individualized assessment rather than applying blanket rules based on a diagnosis.1 A student diagnosed with depression, for example, cannot be automatically excluded from clinical rotations or flagged as a safety concern. The question is always whether the student can meet essential program requirements with or without accommodation.
Common Reasonable Accommodations
Accommodations vary by student and situation, but the most frequently provided options include:
- Extended testing time: Often 1.5 times the standard allotment, arranged through the institution's disability services office.
- Flexible attendance policies: Allowing excused absences for therapy sessions, psychiatric appointments, or acute symptom management without academic penalty.
- Reduced course load: Permitting a student to take fewer credits per semester while maintaining program enrollment and financial aid eligibility.
- Leave-of-absence options: Structured pathways that let a student step away for treatment and return to the program with a clear re-entry plan.
- Testing environment adjustments: A private or low-distraction room for exams.
When clinical sites are involved, the program should communicate the accommodation itself (for example, a modified schedule), not the student's diagnosis.1 Clinical site partners need to know what is being adjusted, not why from a medical standpoint.
The Licensure Question: Will Seeking Help Hurt My Career?
This is the question students are afraid to ask, and it is the one educators must answer clearly. Seeking mental health treatment does not affect NCLEX eligibility. It is also not grounds for denial of state nursing licensure.2
State boards of nursing have been moving steadily away from diagnosis-based questions on licensure applications. The trend, supported by the American Association of Colleges of Nursing (AACN), is toward asking only about current impairment that could affect safe practice, not about a history of diagnosis or treatment. The AACN has specifically recommended eliminating unnecessary and discriminatory mental health questions from licensure applications.2 Research published through the National Institutes of Health reinforces this direction, noting that intrusive mental health questions on credentialing applications deter healthcare workers from seeking help.2
That said, some variation still exists across states. Educators should familiarize themselves with the specific language on their state board's application and share that information transparently with students. When students know that getting help will not derail their licensure, they are far more likely to access treatment early.
Creating a Culture of Safe Disclosure
Knowing accommodations exist means nothing if students are too afraid to request them. Nurse educators set the tone. Addressing the stigma reduction strategies for nursing students who struggle academically or personally is an essential first step. A few practices make a measurable difference:
- Include accommodation information in every syllabus and discuss it verbally on the first day of class, normalizing the process before anyone needs it.
- Separate the accommodation request from the grading relationship. Students should work with disability services, not disclose directly to the instructor evaluating their clinical performance.
- Avoid language that frames mental health treatment as a weakness or liability. Statements like "if you can't handle the stress, nursing may not be for you" push students underground.
- When a student does disclose, respond with practical next steps (connecting them to the disability services office, reviewing timeline options) rather than unsolicited advice about their diagnosis.
The goal is straightforward: students who need support can access it without worrying that honesty will cost them their degree or their license. That requires educators who know the law, understand the accommodations available, and communicate both with clarity and consistency.
Study Strategies and Balance: Helping Students Manage Competing Demands
Telling a stressed nursing student to "study harder" rarely helps; teaching them to study differently almost always does. The contrast that matters here is passive review (rereading notes, highlighting, recopying lectures) versus active, spaced practice. The first feels productive and burns hours. The second is uncomfortable, efficient, and matches how clinical knowledge actually needs to be retrieved at the bedside.
Strategies Validated for High-Volume Clinical Content
Nursing students are not learning a small body of facts. They are learning pathophysiology, pharmacology, assessment, prioritization, and safety simultaneously, then being asked to apply it under pressure. Two techniques consistently outperform passive review for this kind of load:
- Active recall: Students close the book and force retrieval through practice questions, self-quizzing, or teaching the concept out loud. NCLEX-style question banks (Nurse Labs, ATI, UWorld) and AI tools that generate case scenarios are useful here. The goal is to fail, notice the gap, and re-encode.
- Spaced repetition: Tools like Anki schedule flashcards so students revisit material right before they would forget it. For pharmacology and lab values, this is particularly effective.
- Condensing and teaching: One-page summaries and peer teaching force synthesis. If a student cannot explain heart failure to a classmate in five minutes, they do not yet know it.
These are not theoretical. They are the same strategies students recommend to each other in forums like r/StudentNurse, where peer threads regularly walk newer students through what actually worked.1
The Whole Student: Time, Family, and Long-Term Plans
Study strategy alone does not fix overload. Many of your students are juggling young children, partners with kids from prior relationships, full or part-time jobs, and longer-term plans that stack on top of the current program. One recent r/StudentNurse post described a 27-year-old finishing an RN, planning a BSN, eyeing medical school, and navigating a 3.5-year relationship that includes a partner's teenager.1 That is not unusual. It is the norm.
Educators can normalize these conversations by asking, in advisement meetings, what else students are carrying and helping them sequence goals rather than collapse under them.
Build Study Skills Into the Curriculum
Do not assume incoming students arrive with effective study habits. Most do not. Embedding innovative teaching strategies in nursing education can help here: build a short study-skills workshop into orientation or the first semester, with one session on active recall and question banks, one on spaced repetition, and one on time blocking. Two or three hours up front saves months of frustration later, and it signals that the program treats learning how to learn as part of becoming a nurse.
Mental Health Resources and Crisis Support for Nursing Students
Nurse educators who maintain a ready list of vetted mental health resources can respond quickly when students disclose distress or ask for help. Building this knowledge base before a crisis occurs allows you to offer concrete next steps rather than vague reassurances.
National Crisis Resources
These free, 24/7 services should be part of every nursing program's emergency reference materials:1
- 988 Suicide & Crisis Lifeline: Call or text 988, or chat via 988lifeline.org. Free and available around the clock for students experiencing suicidal thoughts or acute crisis.
- Crisis Text Line: Text HOME to 741741 for text-based crisis support. Free, though standard SMS rates may apply. Especially useful for students who prefer not to speak on the phone.
- SAMHSA National Helpline: Call 1-800-662-HELP (4357) for referrals to local treatment services, mental health support, and substance use resources. Free, confidential, and available 24/7 in English and Spanish.
- Warmlines: Non-crisis emotional support lines staffed by trained peers. Students can search state warmline directories or visit NAMI's website to find local options. Free and ideal for students who need someone to talk to before reaching a crisis point.2
Nursing-Specific Support Programs
Several organizations have developed resources tailored to nurses and nursing students:3
- RNconnect 2 Well-being: Text RNconnectMA to 60298 for self-care tips and stress reduction strategies via text message. Free, with standard messaging rates.
- Nurses Together: Peer support group discussions focused on burnout, moral distress, and workplace challenges. Register through the ANA Well-Being Initiative website at no cost.
- Emotional PPE Project: Connects healthcare workers, including nursing students, with volunteer clinicians offering free therapy. Students visit the website to find a provider.
- Happy App (nurse version): A mobile app providing one-on-one emotional support from trained support givers. Free for nurses through sponsorship.
Campus-Level Resources to Verify Locally
Every nursing program should compile institution-specific contacts students can access quickly:4
- Counseling center: Confirm walk-in hours, appointment wait times, and after-hours crisis protocols.
- Student health services: Note whether mental health services are included in student fees.
- Disability services: Clarify the process for requesting accommodations related to mental health conditions.
- Nursing student peer support groups: Contact your student affairs office or academic advisor to learn whether your school offers peer support specific to nursing students. These groups are typically free and provide connection with others navigating similar pressures.
Keeping Resources Accessible
Printing a condensed resource card for syllabi, posting QR codes in clinical simulation spaces, and reviewing options during orientation ensures students know where to turn. Comprehensive nurse educator resources can help you organize these materials efficiently. When educators normalize discussing these resources, students are more likely to use them before small struggles become full-blown crises.
Common Questions About Supporting Nursing Student Mental Health
These are some of the most frequently asked questions nurse educators raise when building mental health support into their programs. Each answer draws on the evidence and strategies discussed throughout this guide.
One in three nursing students screens positive for depression, and the educators who notice first are usually faculty, not counselors. That reality makes student mental health support both an ethical obligation and one of the most practical retention strategies a program can adopt. Embedded counseling, peer networks, and faculty mental health literacy consistently lower attrition and strengthen NCLEX outcomes.
Pick one action from this guide and do it this semester: enroll in Mental Health First Aid certification, add structured post-clinical debriefing to your rotations, or print the resource and crisis support table for every student in your cohort. Small, concrete moves compound.
Finally, talk openly about mental health in your own classroom. Educators who model that openness are the ones who dismantle the stigma keeping students silent, and silent students are the ones we lose.