What you’ll learn in this article…
- Structured orientation with an hour-by-hour framework reduces first-day anxiety and cuts early-semester attrition risk.
- Spacing assessments across the first two weeks instead of front-loading quizzes builds student confidence and study habits.
- A clinical dress rehearsal before day one transforms unfamiliar routines into manageable, practiced steps.
- Responding to first-day mistakes with coaching rather than correction establishes psychological safety for the entire cohort.
The first day of a nursing program can unravel a student's confidence before a single clinical skill is taught. A recent post on Reddit's r/StudentNurse forum illustrated the problem sharply: a user enrolled in an accelerated BSN program described feeling overwhelmed after just one fundamentals lab session, with two tests and four quizzes already scheduled for the following week and ATI described as confusing. That level of early pressure is not unusual, and it falls squarely on nurse educators to manage it.
This is a reality that orientation design, assessment pacing, and first-day classroom culture can either worsen or mitigate. When nearly half of nursing students leave before finishing their programs, the stakes of getting the opening week right are not abstract. How educators respond to that first wave of student anxiety often determines who stays and who drops. The pages that follow offer a structured, hour-by-hour framework for orientation, strategies for spacing early assessments, and practical approaches for building the kind of confidence and community that keep students enrolled.
Why the First Day Sets the Tone for Student Success
Nearly half of all nursing students in the United States will not complete their programs, and the highest-risk period is the first semester.1 That figure alone should reframe how nurse educators think about orientation, opening-week schedules, and the earliest signals they send to a new cohort.
The Weight of First Impressions
Research in educational psychology has long established that early experiences in a program shape a student's sense of whether they belong there. In nursing education, that effect is amplified. Students enter already carrying anxiety about clinical competence, academic rigor, and the stakes of patient care. When the first week compounds that anxiety rather than containing it, many students begin quietly rehearsing their exit before the second week arrives.
The Nursing Universal Retention and Success (NURS) model identifies first-semester attrition as a structural problem, not a personal failure.2 It frames retention as something programs must actively engineer, starting from the moment a student walks through the door. Orientation quality, peer mentoring structures, and early signals of institutional support are not peripheral concerns. They are retention mechanisms.
Belongingness Is Not a Soft Metric
The concept of belongingness in nursing education refers to a student's felt sense that they are seen, welcomed, and capable of succeeding in the program. It matters especially for students from underrepresented backgrounds, first-generation college students, and career-changers entering accelerated tracks. Day one communicates belonging or its absence faster than any syllabus or handbook can. When peer mentoring is built into the first day, students report significantly lower feelings of isolation.3 When structured orientation normalizes the stress of nursing school rather than minimizing it, students are better equipped to persist through the difficult weeks ahead.4 Educators who invest in teaching emotional intelligence to nursing students from the start give their cohorts a stronger foundation for managing that early pressure.
A Real-World Signal Worth Heeding
A recent Reddit post in the StudentNurse community illustrates what a destabilizing first day looks like from the inside. The student, enrolled in an accelerated BSN program, came away from the first fundamentals lab session already feeling overwhelmed, facing two tests and four quizzes in the following week and finding ATI confusing with no apparent guidance offered. That is not a story about a struggling student. It is a story about a program that front-loaded pressure without front-loading support.
That pattern, repeated across cohorts, is one reason nursing student academic failure stigma persists and attrition stays high. The antidote begins on day one, and it begins with you.
What Nursing Students Experience on Day One: Common Anxieties and Stressors
The Imposter in the Room
Many nursing students walk into their first class convinced someone made a mistake admitting them. This imposter syndrome, feeling like a fraud despite meeting all prerequisites, is especially acute in accelerated programs. A real-world example captures this perfectly: an ABSN student began a summer-term fundamentals lab and immediately felt overwhelmed. Scheduled for 2 tests and 4 quizzes in the second week, they already sensed they didn't belong. For educators, that experience is a mirror. It reflects a systemic pattern: a 2025 meta-analysis of nursing student coping strategies confirms that imposter feelings affect more than half of entering cohorts, spiking during the first week.1
Test Tsunami: When Syllabi Trigger Panic
That same student faced a barrage of assessments, 2 tests and 4 quizzes within week two. For educators, this is a cautionary tale. Early-semester assessment overload activates the amygdala, shifting students from learning mode to survival mode. Productive nervousness can sharpen focus, but a constant flood of high-stakes evaluation pushes students toward debilitating anxiety. The difference matters: one leads to engagement, the other to disengagement and attrition. A 2025 DNP project on reducing anxiety in first nursing skills evaluation demonstrated that spaced assessments and formative feedback cut panic scores significantly.2 Program coordinators should audit their early-week syllabi and ask: are we testing readiness or triggering fear?
Technology Shock: ATI, EHRs, and LMS Overload
Modern nursing programs rely on multiple digital platforms: ATI testing, electronic health record (EHR) simulators, and learning management systems (LMS). For a student already battling nerves, navigating three or four unfamiliar tools on day one can feel paralyzing. The Reddit student specifically described ATI as confusing, a sentiment echoed by many. When technology becomes a barrier rather than a bridge, it compounds anxiety. Research on nursing student stress recommends explicit, hands-on technology walkthroughs before content expectations kick in.3 Schedule a low-stakes "tech sandbox" session during orientation, not after.
The Comparison Trap and Fears of Clinical Incompetence
Day one also introduces peer comparison. Students glance around and assume everyone else has it together. In reality, CDC data shows that nursing student stress peaks precisely around these social comparisons.3 Meanwhile, fear of clinical incompetence looms even before the first patient encounter. Students worry they'll freeze during skills check-offs or harm a real person. The 2025 meta-analysis on coping strategies found that structured peer support and faculty-led debriefing can redirect this fear into productive preparation.1 Educators who practice active learning strategies in nursing and name these fears openly, saying "It's normal to feel this way today," normalize the experience without minimizing the work ahead. Understanding the qualities of a good nurse educator can help faculty model this kind of supportive transparency from the very first class.
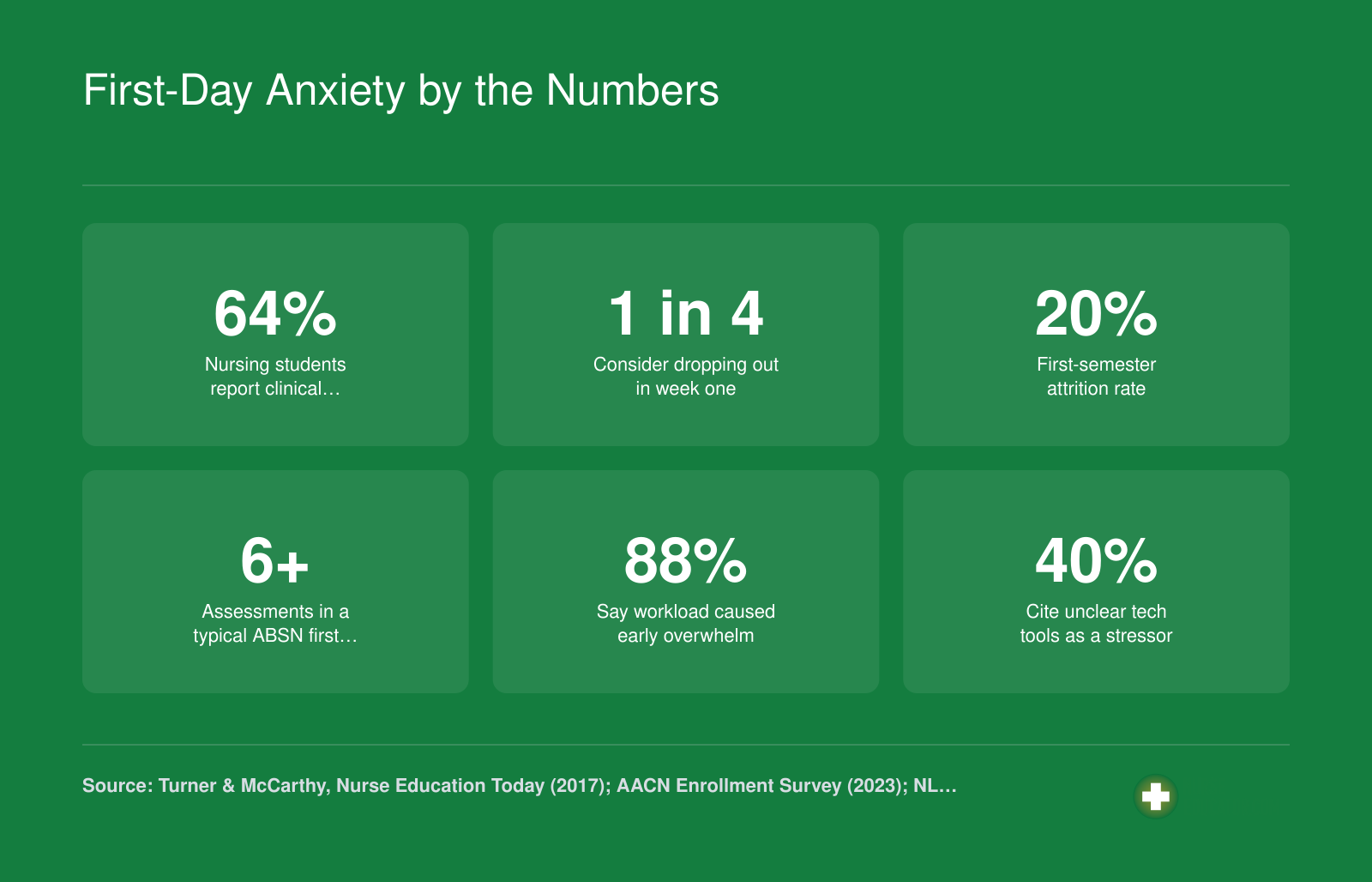
First-Day Anxiety by the Numbers
Nursing students arrive on day one carrying more stress than many educators realize. The data below paints a picture of just how intense the early days can be, especially in accelerated programs. These are the challenges you have the power to address through thoughtful orientation design and assessment planning.
Designing an Effective Nursing School Orientation: An Hour-By-Hour Framework
What should a nursing school orientation actually look like, hour by hour, to set students up for success rather than overwhelm them?
That question matters more than ever as accelerated BSN programs continue to compress months of content into tight timelines. A well-designed orientation is not a formality. It is a functional intervention that shapes how students process everything that follows. When orientation is rushed or treats students as passive recipients of policies, the first clinical rotation or first batch of assessments can feel like a wall with no footholds.
Start with Emotional Grounding, Not Logistics
The opening hour of orientation is the most squandered real estate in nursing education. Programs often fill it with syllabi review and parking passes. A more effective approach begins by acknowledging what students are actually feeling: excitement layered over genuine fear. A short, structured activity that invites students to name their biggest concern removes the pretense that everyone is fine. This normalizes anxiety rather than burying it, and it gives faculty a real-time read on where the cohort is emotionally before any content is introduced.
From there, a brief overview of the semester arc, framed in terms of student experience rather than course objectives, helps students build a mental map. They need to know not just what is coming but roughly when the hardest stretches tend to fall.
Technology Onboarding Deserves Its Own Block
One of the most consistent sources of first-week distress is arriving at a required digital platform without any real preparation. Learning management systems, testing software, and clinical documentation tools all carry their own logic. Treating technology onboarding as something students will figure out on their own is a gamble that costs time and confidence.
Building a dedicated block of at least 30 to 45 minutes specifically for guided, hands-on navigation of required platforms pays dividends quickly. This works best when faculty or student mentors walk through actual tasks, not just screenshots, and when students leave with a short reference sheet they created themselves during the session.
Build in Time for Questions You Did Not Anticipate
Published orientation frameworks from nursing education organizations consistently emphasize the importance of unscripted dialogue. Scheduling a genuine open-floor segment, one where no topic is deflected, signals that faculty are approachable partners rather than gatekeepers. Students who ask questions early are more likely to seek help when the semester intensifies. That kind of approachability is one of the essential qualities of a good nurse educator worth modeling from day one.
A practical hour-by-hour structure might move from emotional check-in to program overview, then to technology onboarding, followed by a campus or clinical site walkthrough, and close with that open Q&A. The sequence matters. Logistical details land better once students feel seen and oriented, not the other way around.
Where to Find Published Frameworks
If you want to benchmark your orientation against current best practices, the National League for Nursing and the American Association of Colleges of Nursing both maintain education resources sections on their websites. Peer-reviewed journals such as the Journal of Nursing Education and Nurse Educator regularly publish research on first-week design, technology integration, and orientation outcomes. Databases like PubMed and CINAHL are the most reliable access points for that literature. For program-specific models, reviewing orientation handbooks posted under the admissions or current-students sections of accelerated BSN program websites can offer concrete examples of how other faculty have structured their first days. If you are looking to understand how orientation fits into the broader scope of what subjects nurse educators teach, that context can help you prioritize the topics your first day needs to cover.
Related Articles
Questions to Ask Yourself
Preparing Students for Their First Clinical Day: Dress Rehearsals, Packing Lists, and Pre-Conference Prep
A clinical dress rehearsal is a structured practice session where nursing students simulate every step of their first clinical day before it actually happens. This preparation strategy transforms an intimidating unknown into a manageable sequence of familiar actions, dramatically reducing first-day anxiety while building procedural confidence.
The Clinical Dress Rehearsal Concept
Schedule a dedicated session one to two weeks before the first clinical rotation where students practice the complete arrival sequence. Have them don their scrubs, lab coats, and required PPE in real time. Walk through badge placement, hair requirements, and jewelry restrictions. If possible, arrange a brief site visit so students can locate parking, entrances, restrooms, break rooms, and the nursing station before they arrive under pressure.
During the rehearsal, have each student practice introducing themselves to a "nurse" (played by a peer or teaching assistant) and a "patient" (a simulation mannequin or volunteer). This low-stakes practice normalizes what can feel like an awkward exchange when students are nervous.
First Clinical Day Packing List
Provide students with a concrete list of what to bring. Guesswork breeds anxiety, and forgotten items undermine confidence. Recommend the following essentials:
- Stethoscope: A quality student model with their name engraved or tagged.
- Penlight: For pupil checks and oral assessments.
- Watch with second hand: Digital or analog, but it must show seconds for pulse and respiratory counts.
- Clipboard or small notebook: For jotting patient notes between charting sessions.
- Drug reference: A pocket guide or approved smartphone app for quick medication lookups.
- Snacks and water: Clinical days are long, and low blood sugar affects critical thinking.
- ID badge and clinical paperwork: Immunization records, facility orientation forms, and any required signatures.
Scaffolding the First Pre-Conference
Pre-conference can terrify new students who have never presented patient information aloud. Reduce intimidation by providing a simple template: diagnosis, relevant history, current medications, morning vitals, and one nursing priority for the shift. During the first session, model the presentation yourself before asking students to share. Accept incomplete answers gracefully and fill gaps without criticism. Understanding nurse educator patient care responsibilities can help you frame this modeling in a way that feels natural rather than performative.
A 30-Second Peer-Introduction Script
Give students a memorizable template they can adapt when meeting unit staff or patients:
"Good morning. My name is [first name], and I'm a nursing student from [school name]. I'll be working with [patient name or unit] today under the supervision of [clinical instructor's name]. Is there anything I can help you with or anything I should know before I begin?"
Practicing this script during the dress rehearsal ensures students can deliver it smoothly even when nervous, helping them appear composed and professional from the moment they arrive. For a broader look at clinical and classroom responsibilities, explore our overview of nurse educator roles and responsibilities.
First-Day Clinical Packing Checklist
Hand this checklist to students before their first clinical or lab day so nothing gets left behind. Sharing the 'Why It Matters' reasoning helps new nursing students understand professional expectations rather than just memorizing a list. The checklist is divided into items needed for classroom or lab settings and items specific to the clinical environment.
| Category | Item | Why It Matters |
|---|---|---|
| Clinical Essentials | Stethoscope (with name tag or label) | You will use it every shift, and labeling prevents mix-ups in shared spaces. |
| Clinical Essentials | Penlight | Required for pupil checks, throat assessments, and other focused exams. |
| Clinical Essentials | Bandage scissors | Needed for dressing changes and tape removal; keeps you from borrowing a preceptor's pair. |
| Clinical Essentials | Watch with a second hand (or digital seconds display) | Accurate pulse and respiratory rate counts require timing to the second. |
| Clinical Essentials | Hemostats or Kelly clamp | Useful for clamping tubing and managing drains safely during patient care. |
| Documentation and Tech | Black ink pens (at least two) | Most facilities require black ink for legibility in paper charting; a backup saves time. |
| Documentation and Tech | Small pocket notebook or clinical worksheet | Lets you jot patient data, lab values, and questions for post-conference review. |
| Documentation and Tech | Laptop or tablet (classroom and lab days) | Needed for accessing the learning management system, ATI modules, and lecture slides. |
| Documentation and Tech | Drug reference app or pocket guide | Quick medication lookups build safe practice habits from the start. |
| Personal Care | Extra hair ties or bobby pins | Keeps hair secured and within infection-control standards during patient care. |
| Personal Care | Snacks and a water bottle | Clinical days run long; staying fueled helps maintain focus and prevents lightheadedness. |
| Personal Care | Comfortable, regulation-compliant shoes | You will be on your feet for hours; proper footwear prevents blisters and back pain. |
| Personal Care | Hand lotion (unscented) | Frequent handwashing dries skin quickly; unscented formulas respect patient sensitivities. |
| Paperwork | Student ID and clinical site badge | Facilities require visible identification for security and HIPAA compliance. |
| Paperwork | Copies of immunization records and CPR card | Many clinical sites verify these on the first day; having copies avoids being turned away. |
| Paperwork | Signed clinical agreements or health forms | Incomplete paperwork can delay or prevent your participation in patient care. |
| Paperwork | Course syllabus or clinical rotation schedule | Confirms room assignments, instructor contacts, and objectives for the day. |
Strategies for Reducing Early-Semester Assessment Overload
A recent post on Reddit's StudentNurse forum offered a sobering snapshot of early-semester reality: an accelerated BSN student reported facing two tests and four quizzes in just the second week of a summer-term fundamentals course. The student described feeling overwhelmed before the program had truly begun. For nurse educators, this example illustrates how front-loaded assessment schedules can undermine the very confidence and engagement we hope to build in new students.
What the Research Says About Assessment Spacing
Cognitive load theory, widely applied in nursing education, supports the use of chunking and scaffolding to help students process new information without becoming overwhelmed.1 Spaced learning, which distributes practice and assessment over time rather than concentrating it in the first weeks, improves both retention and confidence. According to current evidence, first-semester nursing courses benefit from weekly or twice-weekly low-stakes quizzes, with each quiz weighted at just one to three percent of the final grade.1 Brief activities lasting five to fifteen minutes help students build retrieval practice habits without the anxiety that accompanies high-stakes exams.
Nationally, undergraduate nursing programs have historically relied heavily on summative exams, but 2025 data show a clear shift toward diversified and formative assessment strategies.2 The AACN Essentials also emphasize aligning assessments with competency development, which calls for longitudinal, scaffolded evaluation rather than early gatekeeping exams.3 These approaches pair well with innovative teaching strategies in nursing education that prioritize student engagement over rote memorization.
Practical Alternatives for the First Weeks
Consider replacing early high-stakes quizzes with ungraded or low-stakes formative assessments. These allow students to practice retrieving information and receive feedback without the pressure of grade consequences. Scheduling the first graded exam no earlier than week three gives students time to acclimate to your course structure, their peers, and the learning management system.
For online or hybrid courses, weekly modules paired with short quizzes help students build routines gradually.4 Cumulative items on later quizzes reinforce earlier material and encourage ongoing review, rather than cramming.1
Introducing ATI Without Adding Overwhelm
ATI platforms are a common source of confusion for new nursing students, as the Reddit post illustrated. Rather than expecting students to self-navigate ATI alongside other new systems, dedicate a thirty- to forty-minute orientation session with a guided walkthrough during the first week.1 Frame early ATI use as formative and exploratory, not punitive.5 This approach reduces anxiety and helps students see ATI as a learning tool rather than another high-stakes hurdle.
Limit the number of new platforms introduced in week one.4 When students must simultaneously learn your LMS, ATI, clinical documentation systems, and course materials, cognitive overload is nearly inevitable. Prioritize what is essential for immediate success and phase in additional tools over the first month.
Building a Better First Week
There is no single optimal test frequency for first-semester nursing courses, but the evidence is clear: spacing assessments, lowering early stakes, and scaffolding platform introductions all support student confidence and long-term retention.1 By designing your assessment calendar with cognitive load in mind, you set students up for success rather than survival.
The first week should assess readiness, not content mastery. Replace graded quizzes with self-check activities, guided tutorials for platforms like ATI, and low-stakes group exercises that let students calibrate their study habits without penalty. When learners feel safe to make early mistakes, they build the confidence needed to tackle high-stakes assessments later in the term.
Building Confidence and Community From Day One
Nursing education is finally catching up to what students have always known: academic performance is inseparable from emotional safety and belonging.
Icebreakers That Actually Build Connection
Many nursing cohorts bond over shared anxiety, but structured activities accelerate trust. Instead of generic introductions, try these discipline-specific approaches:
- Two Truths and a Lie (Clinical Edition): Each student shares two true clinical-related experiences (e.g., shadowing a nurse, caring for a family member) and one false. This surfaces existing healthcare exposure and sparks authentic conversation.
- Paired Interviews with a Twist: Pair students and ask them to uncover their partner's "why nursing?" story, then introduce each other to the group. This shifts focus from self-promotion to active listening.
- Clinical Scenario Gallery Walk: Post short case vignettes on the walls and have small groups rotate, discussing initial reactions. It normalizes uncertainty and demonstrates that everyone brings unique strengths.
Peer Mentorship: A Buddy System That Works
A short-term buddy model pairs each incoming student with a second-semester volunteer for the first two weeks. The mentor's role is simple: answer logistical questions, share survival tips, and model how to navigate early stressors. Critically, mentors are not tutors or therapists. They are navigators who normalize the adjustment process. Provide mentors with a one-page guide covering common first-week concerns (ATI logins, lab etiquette, time management) and set clear boundaries to prevent overextension.
Modeling Approachability from the Podium
Educators set the emotional temperature of the room. In your first lecture, share a brief, relatable story of your own early misstep, whether it was forgetting a skill or feeling overwhelmed in clinical, to demonstrate that expertise grows from imperfection. This kind of vulnerability is one of the essential qualities of a good nurse educator. Explicitly state, "I expect you to ask questions. Silence is not a sign of competence here." Then, establish open office hours within the first three days and invite students to drop by, even if just to say hello. Physical presence signals genuine availability.
Normalizing the Struggle and Mapping Resources
From day one, reframe help-seeking as a professional habit, not a weakness. Say aloud, "Struggling is part of this process, and how you respond to it matters more than avoiding it." This mindset also helps reduce academic failure stigma among nursing students before it takes root. Distribute a one-page resource map listing the tutoring center, mental health counseling, writing support, and financial aid office, with names, locations, and hours. When students see that the institution has planned for their challenges, they feel less isolated and more equipped to persist.
First-Day Mistakes: How Nurse Educators Should Respond
A first-day mistake is any error, misstep, or moment of confusion that occurs during the initial 24 to 48 hours of a nursing program, whether in the classroom, skills lab, or clinical setting. These mistakes are universal, predictable, and entirely normal. Yet the way you respond as an educator in that moment will determine whether your student internalizes the error as a catastrophic failure or a natural part of learning.
Below are five common first-day scenarios, each paired with an ineffective response and a constructive alternative that builds trust and normalizes the learning process.
Scenario 1: Showing Up Without Required Supplies
The Mistake: A student arrives at the first skills lab without a stethoscope, pen light, or watch with a second hand.
Wrong Response: "Did you not read the syllabus? Everyone else managed to bring what they needed. You can't participate today."
Constructive Response: Pull the student aside briefly. "I see you're missing a few items today. Let me lend you a stethoscope for this session, and here's the supply list again. If cost is a concern, our program has a small loan closet, just ask me after class."
Scenario 2: Freezing During a Patient Introduction
The Mistake: During the first clinical shift, a student goes blank while introducing themselves to a patient, stumbles over their title, and rushes out of the room.
Wrong Response: "You need to get it together. Patients notice hesitation. Let's debrief this in front of the group so everyone learns."
Constructive Response: Find a private moment during post-conference. "I noticed you seemed uncertain introducing yourself this morning. That happens to almost everyone on day one. Let's practice it together right now, and you'll do it again tomorrow with more confidence."
Scenario 3: Misunderstanding the Dress Code
The Mistake: A student arrives in navy scrubs instead of the required white, or wears open-toed shoes.
Wrong Response: "Send them home. They should have read the handbook."
Constructive Response: "I can see there was some confusion about the dress code. For today, let's get you a pair of closed-toe shoes from the simulation center, and I'll email you the uniform policy tonight so we're aligned for next week."
Scenario 4: Submitting the Wrong Form
The Mistake: A student uploads their immunization record to the wrong portal, misses a deadline, or submits an outdated form.
Wrong Response: "This is going to delay your clinical placement. You need to be more organized."
Constructive Response: "I see the immunization form went to the wrong place. Let me walk you through the portal right now so you know exactly where things go. I'll note that you submitted on time, just to the wrong spot."
Scenario 5: Breaking Sterile Technique in Lab
The Mistake: During a catheterization simulation, a student touches the catheter tip with an ungloved hand.
Wrong Response: "That's contaminated. In a real patient, you just caused a UTI. Everyone, watch what happens when you don't pay attention."
Constructive Response: "Stop, pause. You've just contaminated the field. That's actually really common the first time. Let's reset, and I'll walk you through the hand positioning again. You'll get it."
The Principle That Governs Every Response
Correct in private, praise in public. This is not a platitude. In nursing education, it is a clinical safety principle. The student who is shamed in front of peers on day one will hide medication errors, near-misses, and knowledge gaps for the rest of the program. The student who experiences a mistake as a correctable moment will self-report, ask questions, and grow into a reflective practitioner. Understanding the clinical nurse educator role helps you see that this kind of responsive mentorship is central to the job, not a sidebar. Your tone in the first 48 hours sets the disclosure culture for the entire cohort.
Common Questions About Supporting Nursing Students on Their First Day
Nurse educators frequently ask how to make those critical opening hours count. Below are answers to the most common questions about supporting nursing students on their first day, drawn from classroom best practices and real student experiences, including insights from accelerated BSN students who have shared their early struggles online.
What if a structured, supportive first day could have shifted that overwhelmed accelerated BSN student from panic to purpose?
The Reddit post that opened this guide captured a defining moment: two tests, four quizzes, and a confusing ATI platform all hitting in week one of fundamentals. That trajectory was preventable. Your first eight hours are not ceremonial. They are an intervention point that shapes retention, confidence, and clinical readiness. A clinical dress rehearsal replaces guessing with competence. Spacing assessments builds trust instead of triggering flight. Hour-by-hour orientation, ATI walkthroughs, and icebreakers that create community are not luxuries. They are retention infrastructure.
Audit your current first-day plan against the strategies in this article. Identify one change you can implement next semester. That single shift might be the difference between a student who stays and one who walks away.