What you’ll learn in this article…
- Psychiatric NP certification volume surged more than 800 percent in nine years, making it the fastest growing nursing credential.
- Both the ANCC and AANPCB offer PMHNP board exams, and educators must understand how each exam's structure shapes student preparation.
- Strengthening undergraduate psychiatric content is the single most important pipeline investment for sustaining the PMHNP workforce.
- Nurse educators can use median salaries exceeding $130,000 alongside mission driven messaging to recruit students into PMHNP tracks.
Psychiatric nurse practitioner certification has surged more than 800 percent over the past nine years, making it the fastest-growing advanced nursing credential in the country. For nurse educators, this acceleration carries immediate implications: program design, curriculum sequencing, student advising, and faculty hiring all need to keep pace with a specialty that has moved from niche to mainstream in less than a decade.
The growth is not hypothetical. It shows up in exam volume, credentialing databases, and workforce projections, and it challenges schools to expand PMHNP track capacity while maintaining clinical placement quality and board pass rates. Understanding what the certification data reveals, how the two certifying boards compare, and where compensation intersects with demand is now baseline knowledge for any educator counseling students through specialty selection or proposing new program tracks to academic leadership.
PMHNP Certification Growth: The Data Behind the Surge
The psychiatric-mental health nurse practitioner credential has grown faster than any other advanced nursing certification over the past decade, and the numbers leave little room for interpretation. Psychiatric NP certification volume surged more than 800% between 2015 and 2024, transforming what was once a niche specialty into one of the most sought-after pathways in advanced practice nursing.1 For nurse educators, this acceleration signals both opportunity and pressure: more students are entering PMHNP pipelines, and the infrastructure to support them has not kept pace.
Understanding the Scale of Growth
As of 2025, approximately 52,176 PMHNPs are practicing nationwide, with the broader psychiatric-mental health APRN workforce reaching 55,520. When you include registered nurses working in psychiatric-mental health roles, the total credentialed psychiatric nursing workforce stands at over 104,000 professionals. Yet even with this growth, supply lags far behind demand. An estimated 123 million people in the United States live in mental health professional shortage areas, underscoring the scale of unmet need and the urgency driving students toward this specialty.3
Historical workforce data shows PMHNP full-time equivalent employment was just 11,025 FTEs in 2018, a figure that has since more than quadrupled in active certificants.4 This exponential increase reflects not just more graduates entering the field, but also a structural shift in how mental health care is delivered and reimbursed.
What Is Driving the Surge?
Three forces converge to fuel PMHNP certification growth:
- Mental health workforce shortages: Decades of inadequate provider supply, compounded by rising rates of depression, anxiety, and substance use disorders, have created sustained demand.
- Mental health parity legislation: Federal and state laws requiring insurers to cover mental health services at parity with medical and surgical care have expanded access and reimbursement.
- Telehealth expansion: The COVID-19 pandemic accelerated adoption of telepsychiatry, enabling PMHNPs to serve patients across state lines and in underserved areas.
Implications for Nurse Educators
This surge means nursing programs are facing unprecedented demand for PMHNP seats. Schools must expand faculty ranks, secure additional clinical placements in psychiatric settings, and often compete for the same preceptors. Clinical placement capacity is the most common bottleneck: psychiatric sites willing to host students are limited, and the ratio of students to qualified preceptors has tightened as cohort sizes grow. Programs that cannot scale their clinical infrastructure risk wait lists, delayed graduations, and frustrated students.
The nursing faculty shortage compounds the challenge. Qualified PMHNP faculty are in high demand, and many choose lucrative clinical practice over academic roles. Given that nurse educator demand continues to climb across specialties, educators tasked with building or expanding PMHNP tracks must navigate these constraints while maintaining quality and preparing students for national certification exams.
Psychiatric NP Certification at a Glance
Whether you are pitching a new PMHNP track to your dean or benchmarking your program against national trends, these figures tell the story. Keep this snapshot handy for accreditation self-studies, advisory board presentations, and curriculum committee discussions.

Two Boards, One Specialty: How ANCC and AANPCB PMHNP Exams Compare
When guiding students toward psychiatric-mental health NP certification, one of the first decisions they'll face is which exam to sit for: the ANCC PMHNP-BC or the AANPCB PMHNP. Both lead to board certification, but they differ in structure, content emphasis, and recognition across states. Understanding these differences helps educators steer students toward the exam that aligns with their practice location and career aspirations. If you already help students navigate choosing between CNE and CNEcl certification, this decision-framing approach will feel familiar.
Exam Structure and Content Focus
The ANCC exam, administered by the American Nurses Credentialing Center, includes 175 questions and allows 3.5 hours.1 Its content scope is broader, covering assessment, diagnosis, treatment, and health promotion across the lifespan, with a strong emphasis on integration of physical and mental health. The AANPCB exam, offered by the American Association of Nurse Practitioners Certification Board, features 150 questions over 3 hours and is described as more clinically focused, drilling deeply into practice-based scenarios and direct patient care.2 Both exams are computer-based and designed to reflect national standards for the PMHNP role.
Recognition and State Board Requirements
State board recognition varies, and educators should encourage students to verify which exam is accepted in their intended state of practice. Historically, the ANCC certification is more widely required by state boards of nursing, but the AANPCB credential has gained ground in recent years and is now accepted in many jurisdictions. Neither exam is uniformly "better"; the choice often hinges on where a graduate plans to practice. Students targeting federal or military positions may also find one credential preferred over the other, so checking specific employer requirements is essential.
Renewal and Continuing Education
Both certifications require periodic renewal through continuing education (CE) and clinical practice hours. While exact renewal fees and CE hour requirements shift over time, the general pattern includes a five-year cycle with a set number of pharmacology and specialty-specific credits. Educators should direct students to each board's website for the most current renewal criteria. Emphasizing lifelong learning from the start prepares students for the maintenance of certification that lies ahead.
Guiding Students Toward the Right Choice
When advising students, frame the decision around three practical questions: Which exam does my state board of nursing recognize? Does my future employer have a preference? Do I feel more confident with a broader content exam or a clinically intense one? Many programs prepare students for both exams, and some students choose to sit for both to maximize flexibility. Because exam fees and pass rates are not static, recommend that students visit the ANCC and AANPCB websites directly for up-to-date cost breakdowns and performance statistics.3 Ultimately, both pathways lead to the same goal: a qualified, board-certified psychiatric-mental health nurse practitioner ready to meet the nation's growing mental health needs.
What Exam Pass Rates and Credentialing Data Reveal
What do PMHNP exam pass rates actually tell us about program quality, and how should educators interpret the rapid jump in test-takers? The honest answer: pass rates are a useful signal, but only when read alongside volume trends and curriculum design.
Reading the Pass Rate Numbers
Both the ANCC and AANPCB publish annual pass rate summaries for their psychiatric-mental health nurse practitioner exams. Historically, first-time pass rates for the ANCC PMHNP exam have hovered in the low-to-mid 80% range, with AANPCB reporting similar performance for its psychiatric-mental health certification. These are aggregate numbers across all programs, so a national average masks wide variation between schools. For context on how pass rate data is analyzed across nursing certifications, the same benchmarking principles that apply to the CNE exam pass rate are relevant here.
For program directors, the question is not whether your graduates are passing, but how your first-attempt rate compares to the national benchmark and how it trends over three to five years. A single dip can reflect cohort variation. A sustained gap of five points or more below the national average usually points to a structural issue.
What Exam Volume Trends Suggest
The number of candidates sitting for PMHNP exams has climbed sharply alongside the 800% surge in certifications over the past decade. That growth is fueled by new MSN and DNP tracks, accelerated pathways, and online program expansion. The concern is whether clinical placement quality and didactic rigor have scaled at the same pace. When exam volume rises faster than the supply of experienced preceptors and psychiatric clinical sites, preparation quality is the variable most likely to slip.
Legacy Credentials and Consolidation
The ANCC's withdrawal of the psychiatric-mental health clinical nurse specialist certification reflects a broader consolidation toward the PMHNP credential as the dominant advanced practice pathway in psychiatric nursing. Educators still teaching legacy CNS content should audit whether that material maps cleanly to current PMHNP scope and exam blueprints. Faculty reviewing nursing education curriculum should ensure psychiatric content aligns with updated credentialing pathways rather than retired CNS frameworks.
A Framework for Diagnosing Pass Rate Gaps
If your program is trailing the national average, work through these areas in order:
- Clinical hour quality: Are students getting genuine psychiatric diagnostic and prescribing experience, or shadow-heavy placements?
- Psychopharmacology depth: Is the curriculum covering full medication classes, dosing logic, and side effect management, not just overviews?
- Lifespan coverage: PMHNP exams test across pediatric, adult, and geriatric populations. Gaps in any one cohort show up in scores.
- Exam blueprint alignment: Has faculty reviewed the current ANCC and AANPCB content outlines within the last 18 months?
- Preceptor calibration: Are clinical preceptors trained on program competencies, or operating independently of your learning objectives?
Questions to Ask Yourself
Implications for MSN and DNP Program Design
Keeping pace with certification growth is one challenge. Designing programs that prepare graduates to actually pass their boards and thrive in practice is another, and the gap between those two goals is where curriculum decisions become consequential.
Aligning Curriculum with Certification Blueprints
Both ANCC and AANPCB publish detailed blueprints for their PMHNP certification exams, and these documents are publicly available on each board's website. Reviewing them is not optional for program directors. The blueprints outline the competency domains that exam candidates are expected to master, and any meaningful shift in those domains, such as the growing clinical relevance of telehealth delivery in psychiatric care, should prompt a corresponding look at whether your curriculum covers that ground adequately.
As of 2024 through 2026, telehealth competencies have become an increasingly visible part of psychiatric NP practice. Whether current exam blueprints formally assess tele-psychiatry skills as a distinct domain is worth verifying directly through each board's published materials, since these documents are updated on a rolling basis. Program faculty who rely on older versions risk missing refinements that affect what graduates need to know.
Using Professional Standards as a Curriculum Compass
Beyond the exam boards, two documents deserve a place in every PMHNP program director's reference library: AACN's Essentials and NONPF's NP Core Competencies. Both have been updated in recent years to reflect a more integrated view of advanced practice, including telehealth as a mode of clinical delivery rather than an add-on.
For masters in nursing education programs, the practical question is whether telehealth-related content appears somewhere in the required coursework, not just as a brief module but as a thread woven through clinical reasoning, ethics, and supervised practice hours. DNP programs face an additional layer of expectation, since doctoral-level graduates are often positioned as leaders who will shape how their institutions adopt new care delivery models. If your DNP curriculum does not address the policy, regulatory, and competency dimensions of tele-psychiatry, that is a gap worth closing. Faculty exploring affordable nurse educator DNP programs should evaluate whether these newer competency expectations are reflected in program design before committing resources.
Finding Models in Existing Programs
Looking at the publicly available curricula of accredited PMHNP programs is a practical shortcut for program development. Many programs now list telehealth-specific courses or describe clinical placement requirements that include virtual care settings. Reviewing these structures does not mean copying them, but it does offer a grounded sense of what peers in the field are building.
The American Psychiatric Nurses Association (APNA) and individual state boards of nursing are also worth contacting directly. APNA periodically issues guidance on training standards, and state boards can clarify whether any specific telehealth supervision or clinical hour requirements apply within their jurisdiction. Program accreditation decisions increasingly reflect these expectations, making early outreach more efficient than reactive revision.
Making the Curriculum Responsive, Not Reactive
The broader lesson for MSN and DNP program designers is that PMHNP education cannot be a static structure. The surge in certification demand means more students are entering these programs with varied clinical backgrounds, and the care settings they will work in after graduation, including community mental health centers, correctional facilities, and remote-access telehealth platforms, require preparation that generic NP curricula may not fully provide. Building regular blueprint reviews, professional organization consultations, and peer program comparisons into your program's quality cycle is what separates a curriculum that adapts from one that gradually falls behind.
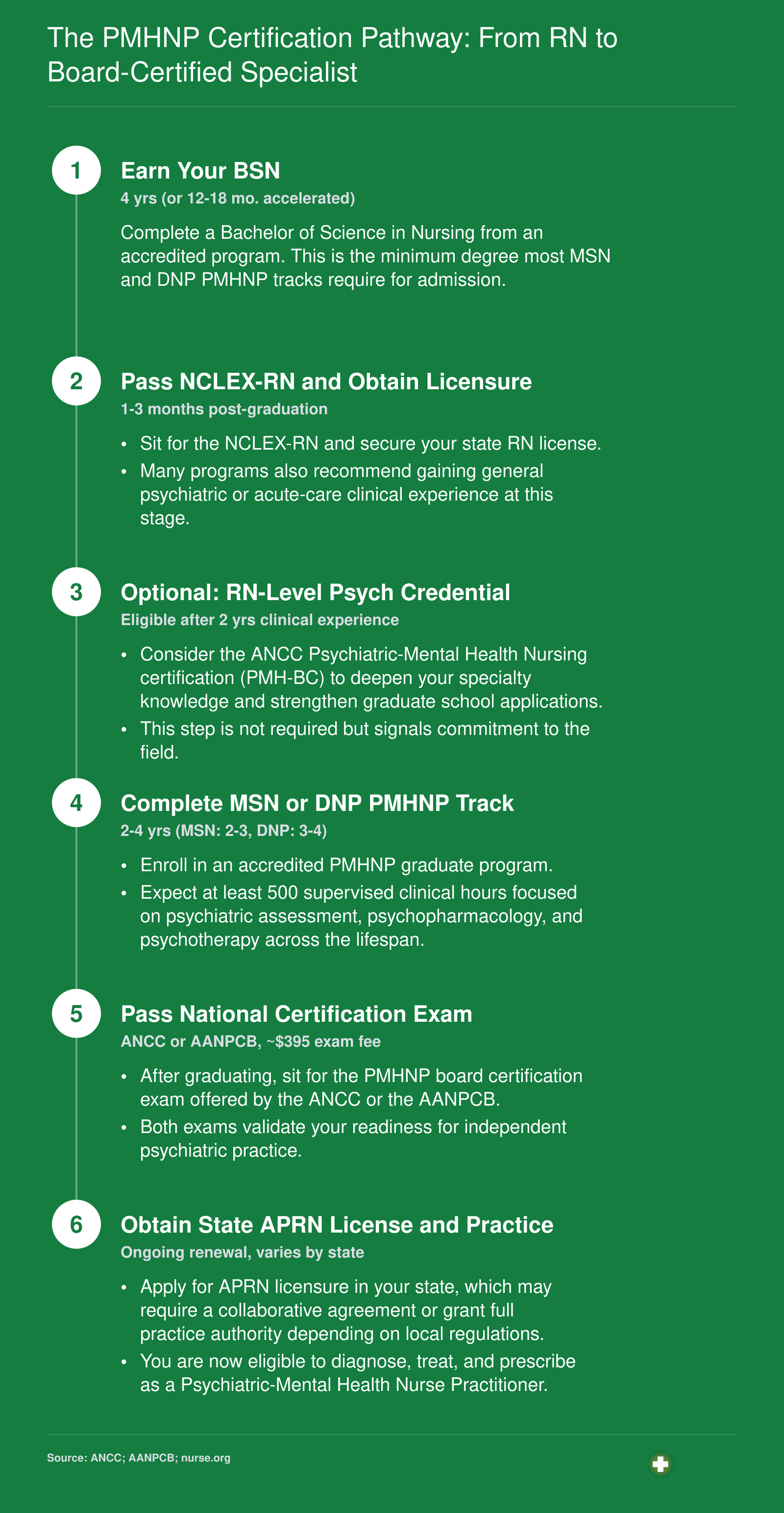
The PMHNP Certification Pathway: From RN to Board-Certified Specialist
The road from bedside nurse to board-certified Psychiatric-Mental Health Nurse Practitioner follows a clear credentialing ladder. Each stage builds on the last, and understanding the timeline helps educators advise students realistically. Note that earning an RN-level psychiatric credential (such as the ANCC PMH-BC) is an optional early step that strengthens clinical readiness before entering a graduate program.
Building the RN-Level Foundation for Psychiatric Mental Health
Strong undergraduate psychiatric-mental health content is the single most important pipeline investment nurse educators can make to sustain the PMHNP workforce. Every board-certified psychiatric nurse practitioner starts as a registered nurse, and the depth of mental health knowledge built during prelicensure education shapes whether graduates pursue the specialty later. If your BSN or ADN program treats psychiatric nursing as a single-rotation afterthought, you are inadvertently narrowing the future applicant pool for MSN and DNP PMHNP tracks.
Strengthening Prelicensure Psych-MH Content
Nurse educators should look beyond the minimum and weave psychiatric-mental health concepts across the curriculum, not just into a standalone clinical rotation. Integrating topics like trauma-informed care, motivational interviewing, and suicide risk assessment into medical-surgical, community health, and pediatric courses normalizes mental health as a core competency rather than a niche interest. Simulation scenarios involving patients with co-occurring psychiatric and medical conditions can reinforce this integration without requiring additional clinical hours.
Students who encounter psychiatric-mental health concepts repeatedly, in varied contexts, are more likely to develop both competence and confidence. That foundation makes the leap to a graduate PMHNP program feel achievable rather than intimidating.
Aligning With National Competency Standards
The American Association of Colleges of Nursing (AACN) publishes competency frameworks, including its Essentials documents, that outline expected outcomes for nursing graduates at every level. Educators designing or revising psychiatric-mental health content should consult these documents directly on the AACN website to ensure alignment with current expectations. Faculty role statements from AACN also clarify qualifications for those teaching in the specialty, which is especially relevant as programs recruit new instructors.
Verifying Faculty Qualifications
If you are hiring or mentoring faculty for psychiatric-mental health courses, start by reviewing what peer institutions expect. Many schools of nursing list minimum credentials in their faculty job postings, and requirements commonly include a PMHNP-BC certification, the Certified Nurse Educator (CNE) credential from the National League for Nursing, or a doctoral degree. Understanding how to become a nurse educator provides a practical benchmark for the qualifications you should seek. Checking individual school faculty pages and current job listings adds further context.
Beyond institutional norms, state boards of nursing sometimes impose requirements for educators in specific clinical specialties that go further than national standards. Consulting your state board's rules ensures you do not overlook a mandate that could affect hiring or course approval.
Useful External Resources for Curriculum Planning
A few key sources can keep your program grounded in current workforce realities:
- AACN Essentials: Review the latest competency documents and faculty qualification guidance at the AACN website.
- ANCC: Check the American Nurses Credentialing Center site for up-to-date details on PMHNP-BC and CNE certification eligibility, exam content, and renewal requirements.
- State board of nursing: Each state's board maintains its own rules for nursing educator qualifications. Some require active clinical certification in the specialty taught.
For educators exploring broader careers in nurse education, positioning the RN-level experience as the deliberate first stage of the PMHNP pipeline, rather than a generic prerequisite, helps programs feed directly into the specialty's explosive growth.
Compensation and Demand: What the Workforce Data Shows
Demand for psychiatric-mental health nurse practitioners is outpacing the supply of credentialed providers, and that gap shows no signs of closing on its own.
For nurse educators, this matters in a very practical way: students choosing the PMHNP pathway are entering a specialty where competitive compensation and strong job security are both well documented. Understanding where to find that data, and how to present it meaningfully, helps you guide students toward informed decisions.
Where to Find Reliable Workforce Data
Several authoritative sources track NP employment trends, and the PMHNP specialty is increasingly visible in each of them.
- BLS Occupational Outlook Handbook: The Bureau of Labor Statistics publishes employment projections for nurse practitioners as an occupational group. The Handbook includes projected job growth rates, median wages, and state-level employment data. Use the site's search tool to locate the nurse practitioner profile and filter for mental health context where available.
- HRSA Behavioral Health Workforce Reports: The Health Resources and Services Administration publishes projections specifically for behavioral health providers, including psychiatric NPs. Their reports often highlight state-level shortage designations and the demand drivers behind them, such as aging populations, increased mental health awareness, and primary care integration.
- Professional Association Surveys: The American Association of Nurse Practitioners (AANP) and the American Psychiatric Nurses Association (APNA) both publish workforce surveys and policy briefs that address PMHNP-specific practice settings, compensation ranges, and employment trends. These are particularly useful for specialty-level context that broad BLS data may not capture.
What University Program Pages Reveal
Beyond federal sources, many PMHNP programs publish regional market data drawn directly from their clinical partners and employer networks. Program pages sometimes include placement rates, demand signals from affiliated health systems, and shortage statistics for the surrounding region. Reviewing several of these pages gives you a layered picture of how national trends translate at the local level. You can also compare offerings across best nurse educator programs to see how different institutions frame workforce outcomes for prospective students.
Why This Matters for Educators
When you teach to a specialty in high demand, salary and employment data become more than background information. They are legitimate recruitment and retention tools, especially as the nursing faculty shortage continues to constrain program capacity. Students who understand the workforce landscape are more likely to pursue the credential with purpose, complete programs, and enter practice prepared. Pointing them toward credible, current sources, rather than anecdotal estimates, builds the kind of critical information literacy that serves them throughout their careers.
NP Salary by State: Where Demand Meets Compensation
The table below draws from the most recent Occupational Employment and Wage Statistics published by the U.S. Bureau of Labor Statistics (2024 data) for nurse practitioners across all specialties. States that combine large employment totals with above-average median pay represent especially strong markets for PMHNP graduates. Keep in mind that state-level variation reflects differences in cost of living, scope-of-practice laws, and the prevalence of rural mental health shortage designations.
| State | Total NP Employment | Median Annual Salary | 25th Percentile | 75th Percentile | Mean Annual Salary |
|---|---|---|---|---|---|
| California | 20,980 | $166,610 | $140,260 | $205,400 | $173,190 |
| Texas | 21,690 | $129,880 | $110,570 | $143,860 | $130,930 |
| Florida | 24,690 | $129,010 | $109,670 | $143,670 | $128,340 |
| New York | 20,430 | $145,390 | $128,190 | $164,670 | $148,410 |
| New Jersey | 9,590 | $149,620 | $126,030 | $162,250 | $140,470 |
| Illinois | 9,560 | $128,620 | $111,450 | $138,420 | $128,880 |
| Massachusetts | 8,920 | $138,890 | $125,590 | $160,310 | $145,140 |
| Minnesota | 8,690 | $128,570 | $103,250 | $139,590 | $128,120 |
| Arizona | 7,540 | $133,790 | $115,290 | $151,650 | $132,920 |
| Indiana | 7,470 | $128,280 | $111,210 | $134,840 | $126,520 |
| Wisconsin | 4,950 | $128,580 | $117,630 | $137,150 | $130,490 |
| Washington | 4,790 | $140,220 | $125,890 | $161,730 | $143,620 |
| Colorado | 4,130 | $129,750 | $110,300 | $139,440 | $127,610 |
| Connecticut | 3,680 | $138,960 | $125,910 | $159,680 | $141,140 |
| Iowa | 2,810 | $129,420 | $115,950 | $137,900 | $133,020 |
| Oregon | 2,430 | $144,600 | $129,840 | $163,240 | $148,030 |
| New Mexico | 1,870 | $138,440 | $113,240 | $156,000 | $136,620 |
| New Hampshire | 1,790 | $132,440 | $120,270 | $143,010 | $133,660 |
| Idaho | 1,570 | $128,940 | $119,290 | $140,920 | $131,380 |
| Rhode Island | 1,200 | $130,710 | $126,200 | $160,030 | $139,600 |
| Montana | 1,050 | $133,640 | $112,180 | $141,050 | $131,560 |
| District of Columbia | 790 | $131,380 | $119,240 | $143,960 | $137,600 |
| Vermont | 680 | $129,740 | $115,650 | $139,930 | $130,580 |
| Alaska | 570 | $145,450 | $104,000 | $165,510 | $142,340 |
| Hawaii | 470 | $130,940 | $121,410 | $158,100 | $135,020 |
When recruiting students to psychiatric NP tracks, lead with the numbers: median salaries exceeding $130,000 in many states provide a powerful counterpoint to concerns about mental health specialty complexity. Pairing compensation data with mission-driven messaging creates a complete value proposition that attracts both purpose-driven and career-focused candidates.
Guiding Students Toward the PMHNP Pathway
How long does it take to become a board-certified psychiatric-mental health nurse practitioner starting from a BSN degree? The honest answer depends on program model, enrollment intensity, and degree level, but most students complete the journey in two to four years. Full-time MSN-PMHNP programs typically require 18 to 24 months, while part-time tracks stretch to 30 or 36 months. DNP-PMHNP pathways demand three to four years for full-time students and up to five years for working nurses studying part-time. Educators should present these timelines early in advising conversations so students can plan finances, childcare, and work commitments realistically.
Eligibility Requirements for Certification
Both the American Nurses Credentialing Center and the American Association of Nurse Practitioners Certification Board require candidates to hold an active, unencumbered RN license at the time of application and examination. Applicants must graduate from an accredited PMHNP program (CCNE or ACEN recognized) that confers a master's or doctoral degree in nursing. Clinical hour requirements vary slightly: ANCC mandates a minimum of 500 supervised clinical hours focused on psychiatric-mental health populations across the lifespan, while AANPCB requires the same 500-hour threshold but emphasizes documentation of direct patient care in psychiatric settings. Programs that exceed 600 hours give students broader exposure and stronger exam readiness. Educators should verify that every student's clinical log meets or exceeds board minimums before endorsing certification applications.
Certification Costs Students Will Face
Budget transparency matters during the advising process. As of 2026, the ANCC PMHNP examination fee is $395 for members of the American Nurses Association and $525 for non-members. AANPCB charges $450 regardless of membership status. Application fees for most state boards of nursing range from $100 to $300. Study materials add another $200 to $600, depending on whether students purchase review courses, practice question banks, or textbook bundles. Initial certification is valid for five years; renewal costs approximately $300 to $400 plus continuing education credits, typically 75 contact hours for ANCC and similar for AANPCB. Sharing these figures during orientation helps students plan for expenses beyond tuition. Faculty who also hold or are pursuing nurse educator certification can model the value of credentialing across specialties.
Integrating Certification Prep Into Curriculum
Programs that embed exam preparation into coursework report higher first-time pass rates and lower student anxiety. Assign practice exams aligned with ANCC or AANPCB content blueprints during the final semester, scheduling one full-length simulation under timed conditions. Dedicate class sessions to high-weight domains: psychopharmacology, evidence-based psychotherapy modalities, and differential diagnosis of psychiatric disorders. Use mock clinical scenarios that mirror exam case studies, requiring students to synthesize assessment findings, formulate diagnoses, and justify treatment plans within standardized patient encounters. Faculty who review item analysis reports from practice exams can target remediation to weak content areas before students sit for the actual certification exam. Educators looking to strengthen their own teaching credentials may also explore online nursing education degrees to build pedagogical expertise alongside clinical knowledge.
Action Steps for Nurse Educators
Knowing the data is one thing; translating it into semester-level changes that actually move the needle is another. The gap between awareness and action is where too many programs stall, and with PMHNP certification growth showing no signs of plateauing, delay carries a real cost. Here are five concrete steps you can implement starting this academic year.
Audit Your Curriculum Against Current Certification Blueprints
Both the ANCC and AANPCB update their PMHNP exam content outlines periodically, and even small shifts in weighted domains can leave students underprepared. Set a recurring calendar item each summer to pull the latest blueprints, compare them line by line with your course objectives, and adjust lecture hours, case studies, and assessment items accordingly. This process resembles how faculty approach curriculum mapping for NGN, where blueprint alignment drives instructional design. Assign one faculty member to own this workflow so it does not slip through the cracks during busy semesters.
Integrate Telehealth Simulation and Tele-Psychiatry Clinical Exposure
Tele-psychiatry has become a standard delivery model across community mental health and private practice settings. Your simulation lab should reflect that reality. Build at least two standardized patient encounters per semester that use a video platform, and negotiate clinical placement agreements that guarantee students log supervised tele-psychiatry hours. Programs that graduate students without this exposure are sending them into practice with a gap employers will notice immediately.
Expand Clinical Placement Networks Strategically
Clinical site availability remains one of the biggest bottlenecks for PMHNP programs nationwide. Proactively build relationships with community mental health centers, federally qualified health centers, and Veterans Affairs medical systems. These organizations serve high-acuity psychiatric populations and often welcome preceptorship partnerships when approached with a clear, structured proposal. Dedicate time each semester to outreach rather than scrambling when a placement falls through.
Track and Benchmark Certification Pass Rates
Your program's first-time certification pass rate is one of the most visible markers of educational quality. Collect this data systematically from graduates, compare it against published national averages, and share results with faculty during annual curriculum review. If your pass rate dips below the national benchmark, treat it as a signal that specific content domains need reinforcement, not as a footnote to file away.
Model Credentialing Expectations as Faculty
Faculty who hold active PMHNP-BC certification demonstrate to students that board certification is not merely a graduation requirement but a career-long professional commitment. The qualities of a good nurse educator include modeling the professional behaviors you expect from your students. If you teach in a PMHNP track, pursue or maintain your own certification, keep your continuing education current, and share your recertification process openly with students. This normalizes credentialing as an ongoing practice rather than a one-time hurdle.
Why Speed Matters
The over 800 percent surge in psychiatric NP certification reflects sustained workforce demand, not a passing trend. Programs that move quickly on these five steps will attract the most motivated applicants, secure the strongest clinical partnerships, and graduate practitioners who are genuinely ready for the complexity of psychiatric-mental health care. Waiting another cycle is a choice, and it is one your competitors are not making.
Frequently Asked Questions About PMHNP Certification
Below are answers to the questions nurse educators and their students ask most often about psychiatric-mental health nurse practitioner certification. Each response is written to be concise and actionable, so you can reference them during advising sessions or embed them in program materials.