What you’ll learn in this article…
- The 2021 AACN Essentials require nursing programs to embed social determinants of health and population equity competencies across the curriculum.
- Simulation, service learning, and case-based instruction produce measurable shifts in student cultural humility and clinical equity behaviors.
- BLS projects a 16.8 percent growth rate for postsecondary nursing instructors from 2024 to 2034, adding roughly 15,300 positions.
- Validated tools like the IAPCC-R and the PCNA Health Equity Self-Assessment now help faculty evaluate student equity competencies beyond traditional exams.
Black mothers in the United States face maternal mortality rates nearly three times higher than their white peers, a gap that has persisted through decades of workforce diversification efforts and clinical protocols. The fix most often proposed, recruiting more minority nurses or mandating one-hour diversity modules, misses the upstream lever: the 91,600 nursing faculty who shape how every new graduate thinks about causation, accountability, and intervention. Nurse educators determine whether students learn to see health disparities as individual deficits or structural failures requiring systemic response.
Faculty now operate under explicit accreditation language on social determinants and population equity, yet few possess a shared playbook for translating those mandates into classroom practice. Competencies exist on paper; the practical mechanics of embedding them into pharmacology, simulation, or clinical evaluation remain fragmented. This guide walks through the frameworks, teaching methods, assessment tools, and faculty development strategies that can close that gap.
Nursing education positions currently offer median national earnings above $82,000 and projected growth of 16.8% through 2034, making health equity specialization a viable career path for RNs exploring the difference between a nurse and a nurse educator and seeking leverage beyond bedside care.
What Is Health Equity in Nursing Education?
What does health equity actually mean within the context of nursing education, and which standards require programs to teach it?
Health equity in nursing education means preparing graduates to recognize, analyze, and actively work to eliminate the conditions that cause unequal health outcomes across populations. It goes beyond teaching students to treat every patient politely. It asks programs to build the knowledge, skills, and attitudes that let nurses confront systemic barriers, whether those barriers are economic, geographic, racial, or rooted in language and culture.
The Accreditation Foundation
The two major nursing accreditors, CCNE and ACEN, both address health equity through their current standards. CCNE's most recent accreditation standards, publicly posted on the commission's website, require nursing programs to demonstrate that curriculum addresses population health, social determinants of health (SDOH), and diversity as core elements, not electives. ACEN's standards similarly call for evidence that programs incorporate diversity and inclusion across their outcomes and curricula. Because accreditation requirements are updated periodically, going directly to the CCNE and ACEN websites is the most reliable way to confirm current language and expectations for any given accreditation cycle.
The AACN Essentials as a Curriculum Blueprint
The American Association of Colleges of Nursing published its revised Essentials framework in 2021, and two domains in particular shape how baccalaureate and graduate programs approach equity. Domain 7, Population Health, frames SDOH competencies as inseparable from safe, effective nursing practice. It asks graduates to assess community-level health patterns, engage with vulnerable populations, and design interventions that account for upstream causes of illness. Domain 9, Professionalism, reinforces equity by tying professional identity to advocacy, ethical practice, and a commitment to social justice. Together, these two domains signal that equity is not a standalone module but a thread woven through the entire educational experience. Faculty who want to explore what subjects nurse educators teach will find that many of these equity competencies map directly to existing course structures.
Program-Level Application
Accreditation standards and national frameworks describe what programs must accomplish. Individual schools decide how to get there. Visiting a program's official website or requesting its curriculum map often reveals how equity competencies are distributed across courses, clinical hours, and simulation experiences. Mission statements, diversity plans, and program handbooks are equally useful sources.
The National League for Nursing also offers supplementary frameworks and position statements that nursing educators use to build out equity-focused pedagogy. Consulting NLN resources alongside the AACN Essentials gives faculty a broader toolkit for translating accreditation requirements into actual classroom and clinical experiences. Understanding the qualities of a good nurse educator can also help programs identify which faculty strengths best support equity-centered teaching.
Why Nurse Educators Are Central to Reducing Healthcare Disparities
Why are nurse educators important in healthcare? The answer lies in their position as upstream change agents whose influence multiplies with every graduating cohort. While bedside nurses provide essential direct care, nurse educators shape the foundational competencies of entire generations of practitioners. This distinction makes educators uniquely powerful in the fight against healthcare disparities. If you are weighing a move from practice to the classroom, understanding this multiplier effect may confirm that becoming a nurse educator aligns with your goals.
The Scale Argument: Multiplying Impact Through Education
Consider the numbers: roughly 200,000 or more new registered nurses graduate annually in the United States. If equity-focused pedagogy reaches even half of these students, the downstream effect on patient outcomes far exceeds what individual provider interventions can achieve. One nurse educator teaching health equity concepts to 30 students per semester can influence hundreds of practitioners over a career, each of whom may provide care to thousands of patients.
This multiplier effect explains why the National Academies of Sciences, Engineering, and Medicine emphasized strengthening nursing education for health equity in The Future of Nursing 2020, 2030 report.1 The report specifically called for research examining how nursing interventions address social determinants of health and advance equity, recognizing that educational transformation must precede practice transformation.1
Beyond Remedial Training: Embedding Equity From the Start
Many healthcare organizations approach equity training as a corrective measure, offering workshops or modules to practicing nurses who may have received little foundational preparation. This approach, while valuable, treats symptoms rather than causes. Without educators embedding equity into foundational training, practice-level initiatives remain remedial, attempting to retrofit concepts that should have been integral to professional formation.
Early evidence supports this educational-first approach. Studies of social determinants of health screening programs integrated into nursing education show measurable improvements in care delivery.2 One program examining patient navigation found that referral completion rates increased from approximately 20 percent before implementation to 40 percent after students received structured SDOH training, a jump of 10 to 20 percentage points.2 Though these studies typically involve modest sample sizes (up to 300 patients in screening programs), they suggest that curricular interventions translate to practice changes.1
Diversifying the Pipeline as Structural Intervention
Nurse educators also address disparities through their role in diversifying the nursing workforce itself. Meeting the demand for faculty who can lead this work requires confronting the ongoing nursing faculty shortage. Key activities include:
- Recruitment: Actively engaging underrepresented communities and creating pathways into nursing programs
- Mentorship: Providing sustained support that helps underrepresented students navigate academic and professional challenges
- Inclusive classrooms: Designing learning environments where students from all backgrounds can thrive and contribute their perspectives
The Equity-Centered Nursing Leadership Framework introduced in 2023 positions these activities as structural interventions rather than supplementary diversity efforts.3 When nursing graduates better reflect the communities they serve, they bring cultural knowledge and lived experience that enhances care for marginalized populations.
Faculty development programs, such as the Justice, Equity, and Inclusion initiative described in nursing education literature, demonstrate growing institutional commitment to preparing educators for this work.4 These programs recognize that educators themselves need preparation to teach equity effectively, whether through anti-racism curricula (typically studied in cohorts of 40 to 200 students) or comprehensive SDOH integration.1
The evidence base for these educational interventions continues to develop, with most current studies using quasi-experimental or pre-post designs rather than randomized trials.1 Still, the logic is compelling: nurses cannot practice what they were never taught, and educators control what enters the curriculum.
Questions to Ask Yourself
Core Competencies Nurse Educators Need for Health Equity
Accreditation standards now embed health equity language, yet most nursing faculty lack a shared vocabulary for what those mandates mean in practice. The 2021 AACN Essentials introduced explicit competencies around social determinants of health and population equity, while the National League for Nursing has long emphasized recognizing diverse learner needs.12 Synthesizing frameworks from NLN, AACN, and Quality and Safety Education for Nurses (QSEN) reveals five core competency domains nurse educators must develop to prepare students for equitable care.
Cultural Humility and Self-Awareness
Cultural humility requires educators to continuously examine their own biases and recognize the limits of their knowledge about communities different from their own. In practice, this means an educator can facilitate a debriefing on implicit bias without centering their own experience or defensiveness. The NLN's 2020 Novice Nurse Educator Competencies calls for recognizing individual learning and professional socialization needs of diverse learner populations, embedding this expectation into accreditation requirements.1 A concrete indicator: the educator models acknowledging mistakes about cultural assumptions in front of students and uses those moments as teaching opportunities. This kind of reflective practice is one of the essential qualities of a teacher in nursing education.
Anti-Bias Pedagogy Skills
Equity-centered educators design learning experiences that actively disrupt rather than reinforce health disparities. This includes choosing case studies that represent diverse patient populations, using inclusive language in lectures and exams, and interrupting stereotyping during clinical debriefs. While the AACN Essentials 2021 mandate assessment of social determinants of health, the pedagogical methods for teaching that content remain largely best practice rather than accreditation requirement.2 Practical indicator: the educator reviews all course materials annually to identify and remove examples that pathologize marginalized communities.
Social Determinants of Health Content Literacy
Educators must possess deep understanding of how housing, transportation, food security, and systemic racism shape health outcomes, then weave that knowledge throughout the curriculum. The AACN Essentials 2021 Population Health domain explicitly requires students to assess social determinants of health, which means educators need both the content expertise and the curricular mapping skills to integrate SDOH concepts across theory, lab, and clinical courses.2 Both academic vs clinical nurse educators must be fluent in this content, because SDOH concepts appear in classroom instruction and practice settings alike. Indicator: the educator can articulate where SDOH content appears in every course they teach and identify gaps in the sequence.
Policy and Advocacy Knowledge
Understanding the policy landscape that perpetuates or mitigates disparities allows educators to prepare students for systems-level change. This competency is emerging as best practice but not yet universally mandated. Educators should be able to explain how reimbursement structures, scope-of-practice regulations, and public health policies affect access to care for underserved populations. Practical indicator: the educator assigns at least one learning activity per semester that asks students to analyze a health policy through an equity lens.
Inclusive Assessment Design
Equity requires evaluating student competence in ways that do not disadvantage learners from non-dominant cultures or educational backgrounds. This means designing rubrics that assess equity skills explicitly, offering multiple ways to demonstrate mastery, and avoiding exam questions that assume cultural knowledge irrelevant to clinical judgment. Indicator: the educator uses structured rubrics for equity-related objectives and can explain how each assessment method reduces bias.
Related Articles
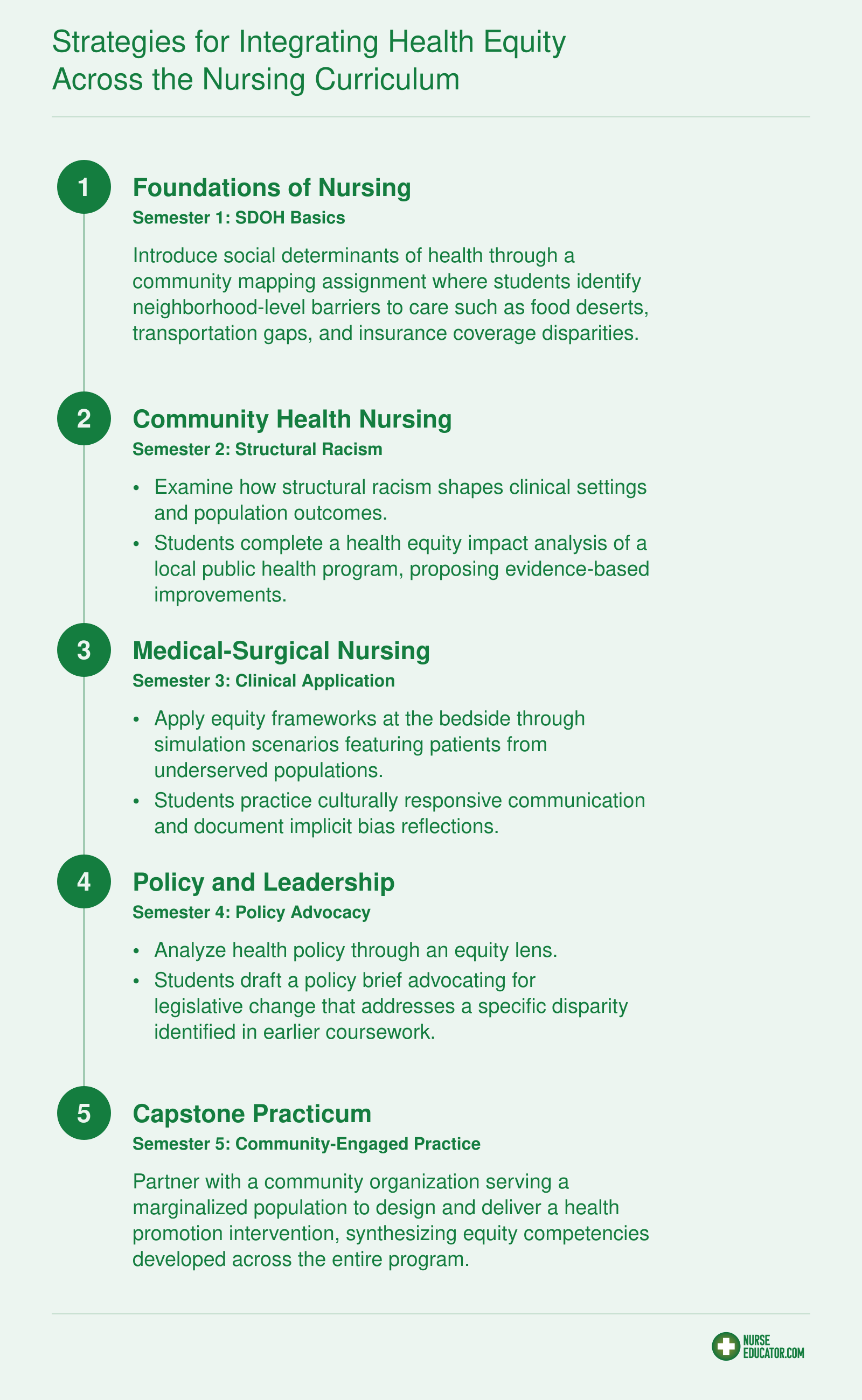
Strategies for Integrating Health Equity Across the Nursing Curriculum
Threading health equity concepts across multiple semesters, rather than confining them to a single diversity elective, gives students repeated exposure that deepens understanding and builds lasting competence. Research on spiral curriculum design shows that revisiting concepts in progressively complex contexts improves retention and clinical application. The blueprint below maps equity content across four core courses so students graduate with equity skills woven into every dimension of their practice.
Effective Teaching Methods: Simulation, Service Learning, and Case Studies
Three evidence-based methods stand out for building equity competencies in nursing students: high-fidelity simulation, service learning, and case-based instruction. Each, when grounded in real disparity data and reflective debriefing, shifts student attitudes and clinical behaviors in measurable ways. These approaches fill a notable gap: top-ranked resources rarely provide specific, named teaching interventions with documented outcomes.
High-Fidelity Simulation to Confront Implicit Bias
At the University of Michigan School of Nursing, a quasi-experimental pre-post study with 80 to 100 students used high-fidelity simulation scenarios featuring an uninsured, non-English-speaking patient.1 The post-simulation debriefing incorporated structured questions that explicitly surfaced assumptions and implicit bias. Students demonstrated measurable improvement in cultural awareness and clinical decision-making. A report from the National Academies reinforces that such immersive, facilitated reflection is critical for developing culturally responsive care.1 To replicate this, design debriefing sessions around questions like, "What assumptions guided your actions?" and "How might language barriers have affected the care you provided?" Pair facilitators from diverse backgrounds and use standardized patients when possible to amplify realism.
Community-Engaged Service Learning That Avoids Extraction
A mixed-methods pre-post study at the University of North Carolina at Chapel Hill School of Nursing involved 50 to 70 students in community health projects with underserved populations.1 Outcomes included statistically significant gains in understanding social determinants of health and a stronger commitment to advocacy. The program's success hinged on a reciprocal partnership model: community stakeholders co-designed the learning objectives and defined project deliverables that benefited their organizations directly. Avoid extractive dynamics by requiring students to complete a community asset map before engaging, and by structuring ongoing feedback loops where partners evaluate student contributions.
Case-Based Learning Anchored in Real Disparity Data
The University of Minnesota School of Nursing implemented case-based modules for MS and PhD students in 2022, using local public health data on diabetes prevalence and housing instability.2 A pre-post evaluation with 25 students found increased confidence in addressing health disparities and applying equity frameworks to clinical cases. As outlined in a Healio review on preparing nurse educators, case-based learning that integrates social determinants data is a core competency for fostering equity-driven practice. For practical implementation, embed raw disparity tables and maps from city or county health departments directly into the cases. Ask students to identify the social and structural determinants driving the numbers, then propose system-level interventions.
Programs that weave all three methods across a curriculum, alongside innovative teaching strategies in nursing education, give students repeated opportunities to practice equity-centered care, normalizing it as a clinical habit. Together, they answer the gap in top-ranked search results that rarely name specific, tested interventions with outcomes.
Assessing Student Equity Competencies: Rubrics, OSCEs, and Evaluation Tools
In 2025, validated instruments like the IAPCC-R cultural competence survey and the PCNA Health Equity Self-Assessment Tool are used across nursing programs to evaluate student learning in health equity.14 Traditional knowledge exams cannot reliably measure growth in cultural humility, an understanding of social determinants of health, or the ability to address bias, all core equity competencies. Instead, nurse educators are turning to formative, multi-modal assessments that capture attitudinal shifts and practice readiness.
Why Standardized Exams Often Miss the Mark
Multiple-choice tests measure recall but rarely probe the nuanced decision-making required to deliver equitable care. They do not reveal whether a student can navigate a cross-cultural encounter with humility or identify structural barriers affecting a patient's health. Because health equity competencies blend knowledge, attitudes, and skills, assessment must go beyond right-answer testing. Formative approaches, where feedback loops guide growth over time, are better suited to this task.
Validated Instruments for Equity-Focused Assessment
Several published tools help faculty quantify equity-related learning. Below are instruments backed by recent research, along with what they measure and when they fit best in the curriculum.
- Method: Inventory for Assessing the Process of Cultural Competence, Revised (IAPCC-R)
- What It Measures: Cultural competence across five constructs: awareness, knowledge, skill, encounters, and desire.1
- Format: Likert-scale self-report survey.
- Best Placement: Pre- and post-curricular evaluation in BSN, MSN, or DNP programs.
- Method: IAPCC Student Version (IAPCC-SV)
- What It Measures: Cultural competence specifically designed for student nurses.1
- Format: Likert-scale questionnaire.
- Best Placement: Undergraduate BSN courses, especially capstone, community health, or global health experiences.
- Method: PCNA Health Equity Self-Assessment Tool
- What It Measures: Clinician knowledge and practice related to health equity.4
- Format: 23 multiple-choice questions plus one open-response item.
- Best Placement: Baseline and outcome measure for health equity content in DNP or MSN programs.
- Method: Student Health Equity Survey (SHES)
- What It Measures: Knowledge, attitudes, and experiences related to health equity and health disparities.2
- Format: Questionnaire.
- Best Placement: Curriculum evaluation for health equity courses; adaptable across nursing levels.
- Method: Evaluating Nursing Curriculum for Cultural Competence (ENCCC)
- What It Measures: Extent to which the curriculum prepares graduates for culturally congruent care.3
- Format: Faculty-completed audit instrument.
- Best Placement: Program-level evaluation for accreditation or curriculum revision.
Complementary strategies such as reflective portfolio rubrics, equity-themed clinical journals, and OSCEs with standardized patients from diverse backgrounds can capture richer, performance-based evidence. Faculty in clinical nurse educator roles often embed these methods within courses to prompt ongoing self-reflection rather than summative grading alone.
Using Formative Feedback to Deepen Equity Competency
Equity competencies develop incrementally. Formative assessment, where students receive timely, constructive feedback on their clinical reasoning, self-awareness, and advocacy efforts, fosters deeper integration than a single high-stakes exam. For example, an implicit bias pre-test given early in a course can be revisited after simulation exercises to help students recognize their own growth. Approaches that build emotional intelligence in nursing complement these tools by helping learners sit with discomfort and respond with empathy during cross-cultural encounters. Faculty who combine validated instruments with reflective dialogue help learners internalize health equity as a practice standard, not just a tested concept.
In 2022, the American Association of Colleges of Nursing found that a significant portion of nursing programs have formally integrated social determinants of health and health equity content throughout their entire curriculum rather than confining it to a single course. This shift reflects a growing recognition that equity competencies must be woven into clinical rotations, simulations, and core coursework to prepare graduates for real-world practice.
Faculty Development and Overcoming Implementation Barriers
Equity-centered nursing education cannot take root unless the faculty teaching it are genuinely prepared to lead it.
Most articles on health disparities in nursing stop at curriculum redesign and say nothing about the people responsible for delivering that curriculum. That gap matters. Even the most thoughtfully constructed syllabus will fall flat if faculty feel underprepared, skeptical, or stretched too thin to engage with equity content meaningfully. Closing the preparation gap requires deliberate, structured faculty development, not a single workshop or a DEI module tucked into an annual retreat.
Named Programs Worth Knowing
Two initiatives offer concrete models for schools looking to build faculty capacity.
A quality improvement program published in the Journal of Nursing Education (2023) by a school of nursing affiliated with the Munn Center at Massachusetts General Hospital delivered a five-workshop series across two semesters, guided by a DEI consultant and structured around the Institute for Healthcare Improvement Model for Improvement.1 Faculty who completed the series made formal commitments to creating inclusive classroom environments, intervening when microaggressions occurred, and making concrete curricular changes. The school-level scope meant the effort built shared language and accountability across an entire department rather than leaving individual faculty to figure it out alone.
At the national level, the AACN Foundation for Academic Nursing launched its Faculty Scholars Grant Program focused on DEI, awarding up to $25,000 per scholar for one to two years of scholarship in this area.3 Two awards were granted in 2023. Programs like this signal that upskilling for equity is a legitimate, fundable scholarly activity, not a volunteer burden.
Other models worth exploring include equity-focused faculty learning communities, which bring small groups of instructors together across a semester to read, discuss, and apply equity frameworks to their specific courses. Train-the-trainer structures, where a few faculty develop deep expertise and then coach colleagues, can stretch limited resources further.
The Barriers That Actually Stall Progress
Faculty resistance is real, but it usually takes the form of discomfort rather than outright opposition. Instructors who have spent decades teaching pathophysiology or pharmacology may feel genuinely uncertain about facilitating conversations on structural racism or implicit bias. That uncertainty, if unaddressed, quietly pushes equity content to the margins.
Workload is the second barrier that consistently comes up. Nursing faculty are already managing clinical practice, scholarly expectations, and heavy advising loads. The ongoing nursing faculty shortage solutions conversation highlights how thinly stretched educators already are, and asking them to overhaul courses from scratch adds friction that most will resist.
Change Management Strategies That Work
Start with faculty champions rather than mandates. Identify two or three instructors who are already interested in equity content and give them protected time and resources to go deeper. Their enthusiasm becomes the gravitational pull that draws in skeptical colleagues over time.
Embed equity into existing course review cycles rather than proposing new standalone courses. When a course comes up for its regular accreditation review or catalog update, that is the moment to integrate social determinants of health, health disparities data, and culturally responsive case studies. The work gets done without triggering the political resistance that a new course proposal often generates.
Speak the language of accreditation. ACEN and CCNE both require evidence that programs address health equity and population health outcomes. Framing faculty development as accreditation preparation, rather than ideological advocacy, shifts the conversation toward institutional self-interest. Most deans and program directors respond to that framing quickly.
Nurse Educator Salary and Career Outlook
The Bureau of Labor Statistics (BLS) reports approximately 91,600 nursing instructors and teachers employed at the postsecondary level nationally as of 2024. Demand is strong: the occupation is projected to grow 16.8% from 2024 to 2034 (roughly 15,300 new positions), ranking 19th out of 832 occupations for growth rate. That pace is more than double the 7% average projected for all postsecondary teachers. Keep in mind that BLS figures are approximate and reflect base salary only. Nurse educators who develop specialized expertise in health equity pedagogy may find additional opportunities in grant-funded research positions, diversity and inclusion leadership roles, and consulting work that can push total compensation higher. The table below highlights the five highest-paying states by median salary, along with national benchmarks. Salaries vary widely by region, institution type, and experience level, so treat these numbers as a starting point rather than a guarantee.
| Location | Median Annual Salary | 25th Percentile | 75th Percentile | Total Employment |
|---|---|---|---|---|
| United States (National) | Data not separately reported at the national level for this occupation. See state figures below. | 91,600 | ||
| District of Columbia | $103,780 | $85,070 | $122,260 | 130 |
| Hawaii | $102,180 | $82,380 | $109,370 | 370 |
| California | $99,010 | $65,510 | $124,290 | 6,120 |
| Texas | $97,610 | $73,670 | $123,360 | 5,940 |
| New York | $93,640 | $63,540 | $128,930 | 5,380 |
Frequently Asked Questions About Nurse Educators and Health Equity
These are some of the most common questions nurses and aspiring educators ask about the intersection of nursing education and health equity. Each answer draws on the competencies, strategies, and assessment approaches discussed throughout this guide.
Awareness-building and systemic change are two very different goals, and equity-centered nursing education must aim for the second. Three levers do the heavy lifting: building faculty competency through structured development, integrating equity content across the full curriculum rather than isolating it in one elective, and securing institutional investment that protects time, funding, and promotion pathways for this work.
Start small but start now. Pick one course you teach this semester and audit it against the AACN Essentials equity competencies, then map at least one assessment (whether a rubric, OSCE station, or reflective debrief) to measurable student growth. Exploring careers in nurse education can also help you see how equity expertise opens doors to leadership, consulting, and grant-funded roles. Nurse educators sit at the only point in the system where every future nurse passes through. That position is rare, and it is exactly why the change you build into a syllabus today reshapes care delivery for decades.