What you’ll learn in this article…
- Three validated tools (PET, CLES+T, and CLEI) serve different program needs based on length, design philosophy, and clinical context.
- Eighteen ready-to-use evaluation questions organized by domain can replace vague feedback prompts with structured, actionable data.
- Collecting feedback at both midpoint and endpoint of each rotation reveals trends that a single survey misses entirely.
- Tiered evaluation forms adapted to student level and specialty produce more accurate data than a one-size-fits-all instrument.
Most nursing students arrive at a clinical placement knowing almost nothing about what to expect. A thread on Reddit's r/StudentNurse captures this plainly: students asking peers how to actually find out what a placement is like before showing up, because their programs have told them nothing. That information gap is not a student failure. It is a systems failure, and nurse educators are in the best position to fix it.
Before anything else, a critical distinction: evaluating a clinical placement is not the same as evaluating student performance. Performance appraisals measure what a student did. Placement evaluations measure the conditions the student worked in, including preceptor availability, patient acuity mix, orientation quality, and psychological safety. Conflating the two produces neither useful faculty data nor fair student records.
Structured evaluation programs that collect and act on site-level feedback consistently produce stronger clinical partnerships and better-prepared graduates. The gap between programs that do this well and those that rely on informal hallway comments is wide, and it is widening as accreditation bodies increasingly expect documented, systematic approaches to clinical quality assurance.
Why Clinical Placement Evaluation Matters for Nursing Education
Clinical placement evaluation has moved from a nice-to-have checkbox to a core program responsibility, yet many nursing programs still rely on informal feedback or anecdotal reports to gauge the quality of their clinical sites. If you are building or refining your program's approach, understanding why systematic evaluation matters will help you advocate for resources and faculty buy-in.
The Link Between Placement Quality and Student Outcomes
Research in nursing education consistently suggests that the quality of the clinical learning environment influences student retention, clinical confidence, and readiness for practice. Programs where students report strong preceptor support, adequate patient exposure, and a culture of psychological safety tend to see higher completion rates and stronger performance on licensure examinations. While isolating the direct effect of any single clinical site on NCLEX pass rates is difficult, the cumulative impact of placement quality across a cohort is hard to ignore. Systematic evaluation gives you the data to identify which sites are contributing to student growth and which may be creating gaps.
Think of it this way: you would never wait until a student fails a course to review your didactic curriculum. The same logic applies to the clinical learning environment. Faculty who cultivate the qualities of a good nurse educator already understand that continuous improvement extends beyond the classroom and into every clinical setting.
Accreditation Standards Demand Systematic Oversight
Both the Commission on Collegiate Nursing Education (CCNE) and the Accreditation Commission for Education in Nursing (ACEN) require programs to demonstrate that clinical sites are sufficient, appropriate, and available to meet program outcomes.1 CCNE standards effective January 1, 2025 expect programs to maintain supporting documentation for each standard, including evidence of ongoing clinical site oversight.2 ACEN's accreditation process centers on a self-study report corroborated by a site visit, during which peer evaluators compare the program's own evaluation claims against actual documentation and observations.3
In practical terms, this means your program needs:
- Records showing each clinical site has been evaluated on a regular cycle.
- Documentation that student and faculty feedback is collected and reviewed.
- Evidence that evaluation findings inform decisions about whether to continue, modify, or discontinue a clinical partnership.
Without these records, accreditation reviewers will flag a gap, and that gap can jeopardize your program's standing.
Protecting Students and the Program
Evaluation data serves a dual protective function. For students, it creates a structured channel to report safety concerns, inadequate supervision, or learning environments that do not align with program objectives. For the program, it builds a defensible record that clinical placements meet professional standards, reducing liability and giving administrators evidence to act on problems before they escalate.
Reframing Evaluation as a Partnership Tool
One of the most common objections you will hear from faculty and clinical coordinators is that formal evaluations could strain relationships with clinical partners. This concern is understandable, especially when clinical sites are scarce and competition for placements is fierce. The ongoing nursing faculty shortage only intensifies the pressure, since fewer faculty means less bandwidth to manage clinical partnerships proactively. However, framing evaluation as a complaint mechanism is a mischaracterization.
When you share aggregated, constructive evaluation data with clinical partners, you are offering them something valuable: insight into how their site is perceived as a learning environment. Many clinical sites welcome this feedback because it helps them improve their own onboarding, preceptor development, and student integration processes. Approaching the conversation as a quality improvement collaboration, rather than a report card, strengthens the partnership rather than threatening it.
The bottom line is straightforward. Evaluation protects your students, satisfies your accreditors, and gives your clinical partners actionable information. Skipping it is not just a missed opportunity; it is a risk your program cannot afford.
Key Criteria Students Should Evaluate in a Clinical Placement
A clinical placement evaluation is a structured way for students to report what they actually experienced at a clinical site, covering the conditions that shaped their learning, their safety, and their professional development. It is not a satisfaction survey. The goal is to capture observable, specific evidence that educators can act on.
For that to happen, the criteria you build into your evaluation instrument must focus on what students can directly observe and experience, not administrative details that lie outside their view. A student cannot judge whether a hospital meets Joint Commission standards, but they can tell you whether their preceptor was present and available when they needed guidance.
Aligning each domain with your program's student learning outcomes also matters. When evaluation criteria map to the competencies you are teaching, the data you collect becomes curriculum intelligence, not just site feedback.
Supervision Quality
This domain asks whether students received adequate guidance from a qualified preceptor or supervisor. A strong indicator is consistent preceptor availability during patient care activities and feedback that was specific, timely, and tied to observable performance. A red flag is a student left to manage unfamiliar clinical situations without a supervisor reachable within a reasonable time, or feedback limited to a thumbs-up at the end of a shift.
Learning Opportunity Variety
Students should assess whether the placement offered a realistic range of patient conditions and nursing tasks relevant to the specialty. A good placement exposes students to cases that stretch their skills under supervision, reinforcing the kind of clinical judgment in nursing you are building in the classroom. A red flag is being assigned only low-acuity, repetitive tasks for the majority of the rotation.
Patient Safety Culture
This domain captures whether staff modeled safe practice and whether students felt comfortable raising concerns. A healthy culture means students observed incident reporting treated without blame, and felt they could ask a question without embarrassment. A red flag is pressure to skip safety checks because of time, or a culture where staff discourage speaking up.
Interprofessional Collaboration, Emotional Support, and Environment
Three remaining domains round out a thorough instrument. Interprofessional collaboration asks whether students observed or participated in teamwork across disciplines. Emotional and psychological support asks whether students had access to debriefing after difficult events and whether the team culture was respectful. Developing emotional intelligence in nursing students depends partly on placements that model empathy and open communication. The physical environment domain covers practical conditions: adequate equipment, private space for handoff communication, and a safe working layout.
Orientation adequacy is worth including as a standalone criterion. Students can directly observe whether they received a site orientation before beginning patient care, including introductions to emergency protocols and unit layout. A site that skips orientation is signaling a broader gap in how seriously it takes student integration.
Keep the language of each question grounded in what a student witnessed or experienced, and you will collect data specific enough to drive real improvements at the site level.
Questions to Ask Yourself
Standardized Evaluation Instruments: PET, CLES+T, and CLEI Compared
Which validated clinical placement evaluation tool should your nursing program actually adopt: PET, CLES+T, or CLEI? Each has a different design philosophy, length, and best-fit use case. Here is how they compare so you can match the instrument to your program's size, student level, and administrative bandwidth.
Side-by-Side Comparison
- Items: PET uses 19 items, CLES+T uses 34 items, and CLEI uses 42 items.1 If you want a short survey students will actually finish, PET is the leanest option.
- Domains measured: PET focuses on welcome and belonging, support to meet learning needs, and confidence and competence through reflection on learning.2 CLES+T covers pedagogical atmosphere on the ward, leadership style of the ward manager, premises of nursing on the ward, the supervisory relationship, and the role of the nurse teacher. CLEI assesses personalisation, involvement, task orientation, innovation, individualisation, and satisfaction.
- Validated populations: All three have been validated with undergraduate nursing students. None of these instruments was originally designed and validated for graduate-level or advanced practice clinical rotations, so adapt with caution if your learners are post-licensure.
- Access and licensing: PET is freely available for educational and research use through the National Placement Evaluation Centre (NPEC); registration and proper citation are required.4 CLES+T is an academic instrument that is generally free for research and educational use with citation, though permission is expected for new translations or major adaptations. CLEI is similarly a research instrument typically used without fee, with permission requested for large-scale or adapted use.
- Digital availability: All three can be administered online and are routinely deployed through standard survey platforms.
Choosing the Right Fit
For a small program or a first attempt at structured evaluation, PET's 19 items lower the response burden and produce focused data on student belonging and learning support. If you need a richer view of the ward environment, including ward leadership and the nursing educator role, CLES+T is the most comprehensive choice and is the dominant instrument in European nursing research. If your program is interested in classroom-style learning environment constructs (innovation, individualisation, task orientation), CLEI maps closely to that framework.
Budget is rarely the deciding factor here, since all three are accessible at no cost for typical educational use. The real trade-off is survey length versus depth of insight, and whether the domains measured align with the questions your faculty actually want answered.
Sample Clinical Placement Evaluation Questions You Can Use
The difference between a vague "How was your clinical?" prompt and a data-rich evaluation lies in structured, actionable questions. Below are 18 ready-to-use questions organized by domain, with guidance on question design and sequencing that produces meaningful feedback you can act on.
Structuring Your Questionnaire for Valid Responses
Start with concrete, observational items before moving to evaluative or emotional questions. When students first recall specific behaviors ("My preceptor demonstrated a skill before asking me to perform it"), they anchor their later judgments in observable facts rather than mood or first impressions. This ordering reduces recency bias and produces more reliable data. Save open-ended reflective prompts for the end, when students have mentally reviewed the full placement experience.
Supervision and Preceptor Support (5-point Likert: Strongly Disagree to Strongly Agree)
- My preceptor was consistently available during my scheduled clinical hours: Detects staffing adequacy and preceptor reliability, flagging sites where students are left unsupervised.
- I received individualized feedback on my clinical performance at least weekly: Measures developmental support; sites scoring low may assign preceptors who lack time or training.
- My preceptor encouraged me to ask questions and think critically: Assesses psychological safety and teaching philosophy, distinguishing mentors from task delegators.
- I was able to discuss my learning goals with my preceptor during the first clinical day: Identifies goal-setting practices that correlate with student satisfaction and competency growth.
Learning Opportunities (Frequency scale: Never, Rarely, Sometimes, Often, Always)
- I performed skills and procedures appropriate to my level of training: Reveals scope-of-practice alignment and whether sites challenge students appropriately.
- I participated in interprofessional rounds or team meetings: Captures exposure to collaborative practice, an AACN Essentials requirement often missing in task-focused placements.
- I cared for patients with diverse diagnoses and acuity levels: Detects clinical variety; monotonous placements score low and may need rotation or replacement.
- I had opportunities to practice clinical reasoning and priority-setting: Assesses cognitive skill development beyond psychomotor tasks.
Safety and Professional Environment (5-point Likert)
- I felt physically safe in the clinical environment: Screens for workplace violence, infection control lapses, or unsafe nurse-to-patient ratios that endanger learners.
- Staff treated me with respect and professionalism: Identifies toxic cultures; students reporting disrespect often disengage or underperform. If you notice patterns of disrespect tied to student anxiety, consider exploring strategies for teaching emotional intelligence to nursing students as a complementary intervention.
- I observed adherence to evidence-based practice and standards of care: Gauges quality of role modeling; students internalize the practices they see, good or bad.
Resources and Organizational Support (5-point Likert)
- I had access to necessary supplies, equipment, and technology: Detects resource scarcity that limits hands-on learning.
- Orientation to the unit was adequate for my learning needs: Poor onboarding correlates with student anxiety and slower skill acquisition. Pairing a strong unit orientation with thoughtful first day of nursing school preparation can ease this transition considerably.
- The patient population matched the course objectives: Ensures curricular alignment; mismatches waste clinical capacity and student time.
Overall Evaluation and Qualitative Data
- Overall, this clinical placement supported my learning goals: (5-point Likert) Provides a global satisfaction metric for benchmarking sites.
- What was the most valuable learning experience at this site?: (Open-ended) Captures strengths to preserve and replicate.
- What change would most improve this placement for future students?: (Open-ended) Generates specific, actionable improvement targets rather than generic complaints.
Why These Domains and Question Types Matter
Likert-scale items yield quantitative data you can trend over time and compare across sites. Frequency scales reveal consistency, not just presence, of good practices. Open-ended questions surface issues you did not anticipate and provide context for numerical scores. Together, they give you both the statistical power to justify site decisions and the narrative detail to guide improvement conversations with clinical partners.
Related Articles
Step-By-Step: Implementing a Placement Evaluation System
Many nursing programs collect student feedback on clinical sites, but few build a true evaluation system with digital infrastructure and a defined collection cadence. The two steps most programs skip are selecting a purpose-built digital platform and establishing a dual-timepoint collection schedule (midpoint formative plus end-of-placement summative). Following the sequence below will help you move from ad hoc surveys to a sustainable, accreditation-ready evaluation cycle.
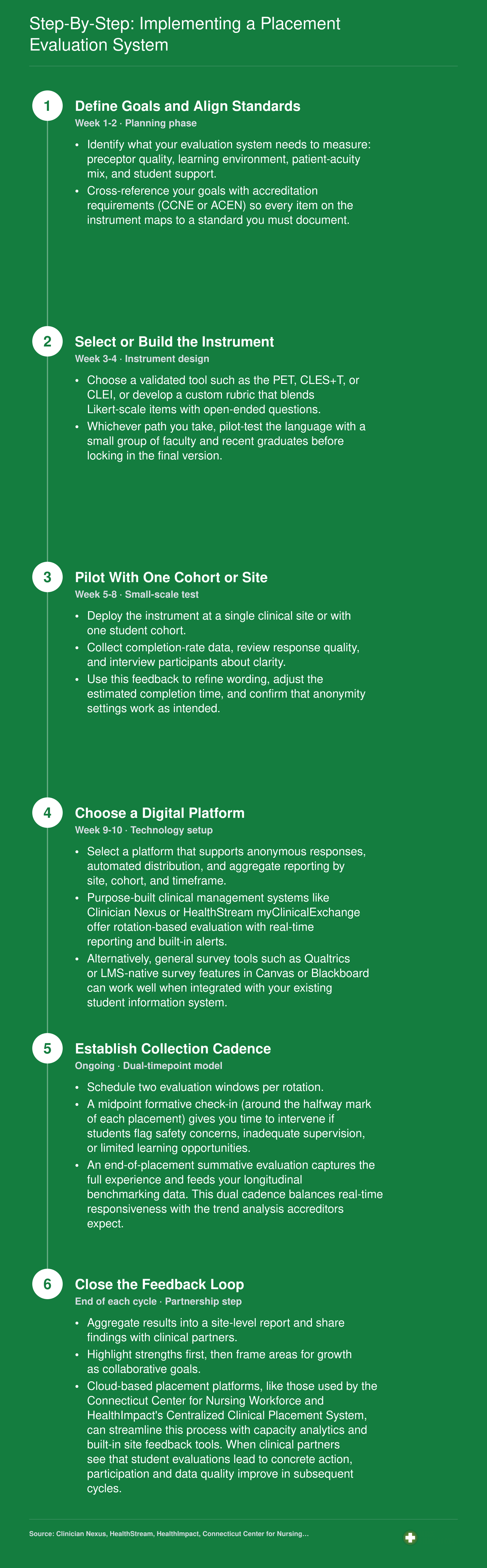
Clinical sites that receive structured, actionable feedback are more likely to maintain long-term partnerships with nursing programs. When you frame evaluation as collaborative quality improvement rather than criticism, you build trust, demonstrate professionalism, and create opportunities for dialogue that benefit future student cohorts and strengthen the clinical education pipeline.
Interpreting Results and Setting Benchmarks for Clinical Sites
Raw numbers versus meaningful patterns: the difference between these two approaches determines whether your clinical placement evaluation data actually drives decisions or simply fills a filing cabinet. Once students have completed their evaluations, your job as a nurse educator shifts from data collection to data interpretation, and that requires a clear, defensible framework.
Calculating Composite and Subscale Scores
Most validated instruments use Likert-scale items grouped into domains such as supervisory support, learning opportunities, and interprofessional collaboration. The simplest approach is to calculate the mean score for each domain by adding the item ratings and dividing by the number of items. This gives you a subscale score per domain and, when averaged across all domains, a composite site score.
A weighted approach assigns greater importance to domains your program considers higher stakes. For example, you might weight patient-safety items or direct preceptor supervision at 1.5 times other domains. There is no single correct weighting scheme; the key is to document your rationale and apply it consistently so scores remain comparable across sites and semesters.1
Setting Benchmark Thresholds
Published universal cut scores for instruments like the CLES+T or PET do not currently exist.2 Both tools were designed for benchmarking and comparison rather than pass/fail classification.3 That means your program needs to set context-specific thresholds using local norming. A practical starting framework looks like this:
- Acceptable site: Composite and subscale scores at or above your program's rolling mean, with no domain falling below the 25th percentile of all your sites.
- Flagged site: Any domain score that drops below the internal benchmark, a consistently weak subscale across two or more evaluation cycles, or a notable negative shift from the previous cohort.3
- Discontinued site: Persistently low scores paired with repeated adverse reports, documented supervision gaps, or inability to meet stated learning objectives after a formal improvement plan.2
Programs that publish on benchmarking clinical placement quality recommend combining percentile rules with red-flag criteria (such as any safety-related item scoring below a set minimum) rather than relying on a single composite number alone.3
Using Trend Analysis Instead of Snapshots
A single cohort's ratings can be skewed by one difficult semester or an unusually strong group of preceptors. Comparing site scores across at least three consecutive cohorts reveals whether a dip is an anomaly or a genuine decline. In practical terms, plot each site's composite score on a simple line graph semester by semester. A downward trajectory over two or more cycles is a far more reliable signal for intervention than any one low score.
Rolling averages, calculated by averaging the current semester with the two prior semesters, smooth out noise and give you a steadier picture of site performance over time.4
Handling Small Samples and Response Bias
Some clinical sites host only two or three students per rotation. With samples that small, a single outlier rating can dramatically shift the mean. Consider pooling data across two or three semesters before drawing conclusions about these sites, and flag the sample size alongside any reported score so decision-makers understand the level of confidence behind the numbers.
Response bias is equally important. Students sometimes fear that critical feedback could affect their grade or their relationship with a preceptor. You can reduce this concern by collecting evaluations after final grades have been posted, by ensuring anonymity (suppressing results when fewer than five responses are collected at a single site), and by framing the evaluation explicitly as a program-improvement tool rather than a complaint mechanism. Clear communication about how results are used, and how individual responses cannot be traced, encourages honest reporting and produces data you can actually trust. Building these communication habits is part of what makes a great nurse educator: the ability to create psychological safety around feedback so your data reflects reality.
Turning Evaluation Data Into Clinical Site Improvements
What do you actually do with clinical placement evaluation results once students submit them? Collecting feedback without acting on it is the fastest way to erode student trust and hollow out your evaluation program. The three steps below give you a repeatable workflow for moving from raw responses to real change.
Step 1: Aggregate and Anonymize the Data
Before anything leaves your desk, pool responses by clinical site and strip out any detail that could identify an individual student. That means removing cohort-specific phrasing, unusual shift references, or comments that describe a single memorable incident tied to one person. Aggregating by site rather than by individual preceptor protects students and keeps the conversation with your clinical partner focused on systemic patterns rather than personal grievances.
Once data is cleaned, calculate composite scores for each domain you measured, such as preceptor availability, feedback quality, learning opportunity variety, and psychological safety. Compare each site's scores against your program-wide average so the feedback report carries context, not just raw numbers.
Step 2: Deliver a Structured Site Feedback Report
A site feedback report does not need to be lengthy to be useful. A single-page format works well and should include:
- Composite domain scores: Numerical averages for each evaluation category, displayed alongside the program average for comparison.
- Top two strengths: Specific, evidence-based language drawn from the data, not generic praise.
- Top two improvement areas: Framed as development opportunities rather than deficiencies.
- Anonymized student comments: One or two direct quotes that illustrate a pattern already visible in the scores.
Sharing this report with the clinical site coordinator before any face-to-face meeting gives them time to process the findings without feeling put on the spot.
Step 3: Co-Create an Action Plan with Measurable Goals
The most common mistake educators make at this stage is leaving the meeting with vague language like "we will work to improve feedback practices." That commits no one to anything. Instead, tie each improvement area to a concrete action, a responsible party, and a timeline.
If students consistently scored feedback quality low, the action item is a targeted preceptor development workshop on delivering structured clinical feedback, scheduled within the next semester. If orientation clarity was the concern, the site agrees to revise its student orientation checklist by a specific date. Measurable goals give you something to revisit at the follow-up meeting six months later. This kind of evidence-driven cycle is one reason building a research culture in nursing education matters for program quality overall.
Closing the Loop With Students
None of this work pays off if students never hear what happened. A brief end-of-semester message explaining two or three changes made in response to evaluation feedback does more for future participation rates than any reminder email urging students to complete the survey. When students see that their input shifted a preceptor workshop agenda or prompted a site to revise its orientation process, the evaluation stops feeling like a bureaucratic checkbox and starts feeling like a professional responsibility worth taking seriously.
Adapting Evaluations for Different Student Levels and Specialties
A single evaluation form cannot capture the vastly different learning needs of a first-semester fundamentals student and a final-year student preparing for independent practice. The challenge lies in balancing consistency for longitudinal tracking against the flexibility required to assess developmentally appropriate outcomes. A tiered approach solves this tension: maintain a stable core of questions while adding targeted items that reflect each cohort's clinical focus.
Tailoring for Student Progression
First-year students need clinical environments that prioritize orientation quality, physical and psychological safety, and a sense of belonging. Their evaluation questions should ask whether they received adequate site orientation, felt welcomed by staff, understood emergency protocols, and had access to appropriate supervision during basic skills. These foundational elements, much like the ones you would address when preparing nursing students for first clinical experiences, determine whether novice learners can focus on skill acquisition rather than survival.
Final-year students require environments that foster autonomy, complex decision-making, and preceptor relationships that mirror collegial mentorship. Their evaluation items should probe whether they received opportunities to lead patient care, engage in critical thinking discussions, participate in interprofessional collaboration, and receive constructive feedback on clinical judgment rather than just task completion.
Specialty-Specific Adaptations
Different clinical specialties demand unique evaluation dimensions:
- ICU and acute care: Add items assessing exposure to high-acuity patients, appropriate nurse-to-patient ratios for learning, access to advanced monitoring technologies, and opportunities to participate in rapid response or code situations under supervision.
- Community and public health: Include questions about population-level assessment opportunities, independent practice readiness, home visit logistics, and exposure to social determinants of health across diverse communities.
- Mental health: Incorporate items evaluating therapeutic communication practice, supervision availability for emotional processing after difficult patient interactions, and opportunities to participate in treatment planning and group therapy facilitation.
When building community and public health evaluation items, consider how nurse educators promote health equity through intentional placement design that exposes students to underserved populations.
Maintaining Longitudinal Comparability
To track clinical site quality over time, keep eight to ten core items identical across all evaluation versions. These should address universal elements: preceptor availability, learning opportunity adequacy, communication clarity, respect from staff, and alignment between clinical experiences and course objectives. Then add three to five specialty-specific or level-specific questions as a separate module. This structure allows you to compare sites across years while still capturing the nuanced feedback each student population needs to provide.
Common Questions About Clinical Placement Evaluation
These are the questions nurse educators ask most often when building or refining a clinical placement evaluation process. If you are just getting started, these answers will help you distinguish key concepts and avoid common missteps.
Clinical placement evaluation is not a form you send out at the end of a rotation. It is an ongoing quality culture that connects students, faculty, and clinical partners around a shared commitment to better learning environments.
Your next step is concrete: pick one validated instrument from the PET, CLES+T, and CLEI comparison, then pilot it at your strongest clinical site this semester. Use those early results to calibrate realistic benchmarks before scaling program-wide. Starting small lets you refine your process, train preceptors on how feedback will be used, and build internal credibility with the data. That iterative, evidence-driven mindset is central to fostering research culture in nursing education, and it applies just as powerfully to clinical site oversight.
Do not wait for the perfect system. An imperfect evaluation process, run consistently and acted on transparently, will always outperform a polished tool that never launches.