What you’ll learn in this article…
- Most nurse educators interact with patients indirectly, though clinical instructors regularly supervise bedside care in real time.
- BLS projects 16.8% job growth for postsecondary nursing instructors from 2024 to 2034, well above the national average.
- Patient educators and nurse educators serve different audiences: one teaches patients, the other teaches nurses.
- Dual role positions let you combine part-time bedside shifts with formal teaching responsibilities to maintain clinical skills.
Many nurses assume becoming an educator means leaving patient care, but the reality is more layered. Nurse educators span academic, hospital, and community settings, and patient contact varies from zero to daily bedside supervision.
The National League for Nursing's 2026 workforce framework identifies four distinct roles, each with a different relationship to clinical practice. Some positions require active licensure and ongoing clinical hours; others rarely involve a patient encounter.
For nurses weighing the transition, the real question is not whether educators work with patients, but which model of educator you intend to become, and whether your state board expects you to prove hands-on competence to keep that license active.
What Does a Nurse Educator Actually Do?
The National League for Nursing recognizes four distinct nurse educator roles in its 2026 workforce framework, each anchored in the fourth edition of "The Scope of Practice for Academic Nurse Educators."1 That document outlines seven core competencies, from facilitating learning and guiding learner development to advancing scholarship and understanding the forces shaping health care, giving the role a scope far wider than many nurses expect.2
Roles Defined by Two Major Frameworks
Both the NLN and the American Nurses Association describe nurse education as an active, multidimensional specialty. The NLN centers its framework on academic settings: designing and revising curriculum, mentoring students through foundational and advanced coursework, evaluating clinical competencies, and leading faculty development initiatives. The ANA broadens the picture by addressing nurses who work in professional development contexts inside health systems, a population it supports through the Nursing Professional Development Certification (NPDC-BC).3 Together, these frameworks make clear that nurse educators are accountable not just for what students learn in a classroom but for how competently they perform in practice.
Three Employer Types, Three Different Daily Realities
To understand where nurse educators work, consider how the setting shapes everything about the job.
- Universities and colleges: Faculty design course syllabi, grade written work, run simulation labs, supervise clinical rotations, and often carry a research or scholarship expectation.
- Hospitals and health systems: Staff development educators onboard new hires, coordinate continuing education, lead skills fairs, and respond to quality gaps identified through incident reviews.
- Community organizations and public health agencies: Educators develop health literacy programs, train community health workers, and deliver patient-facing instruction at a population level.
Each setting demands a different balance of pedagogical skill, clinical currency, and administrative capacity.
Credentials and Certification
The minimum credential for most nurse educator positions is a BSN, but a Master of Science in Nursing with a nurse educator concentration is the standard expectation for academic roles.3 Doctoral preparation (DNP or PhD) is increasingly required for tenure-track faculty. On the certification side, the NLN offers four credentials: the CNE for experienced academic educators, the CNEcl for clinical nurse educators, the CNEn for novice educators with up to three years of experience, and the CNEpv for those in practice and vocational settings.1 These credentials signal specialization and, in many institutions, carry a pay premium.
More Than a Classroom Role
The label "educator" can mislead nurses who picture a lecture hall and nothing else. Understanding the academic vs clinical nurse educator distinction helps clarify just how varied the work can be. Clinical instruction happens at the bedside, in simulation labs stocked with high-fidelity manikins, and through preceptorship oversight where students deliver real care to real patients under direct supervision. In those environments, the nurse educator is not a distant administrator: she or he is present, assessing student technique, intervening when patient safety is at risk, and modeling the clinical reasoning that novice nurses are still building. The classroom is one venue. The hospital unit, the simulation suite, and the community clinic are others.
Do Nurse Educators Provide Direct Patient Care?
The honest answer sits somewhere between a clear yes and a clear no, and where you land depends almost entirely on your setting, your role title, and whether your institution is running short-staffed on any given shift.
The Short Answer: Most Do Not Hold Their Own Patient Assignments
For the majority of nurse educators, particularly those working in academic settings such as colleges and universities, direct patient care is not part of the job description. Their primary function is teaching: designing curricula, delivering lectures, evaluating competencies, and developing staff.1 They are not assigned a patient panel, they do not administer medications as part of their educator duties, and they are not responsible for managing a caseload the way a bedside nurse is.
That said, the line between "educator" and "clinician" is blurrier than most job postings suggest.
Clinical Teaching Is Hands-On, Even If It Is Not Direct Care
When academic nurse educators supervise students in a clinical practicum, they are present at the bedside. They guide students through physical assessments, medication administration, and patient communication. If a student is struggling with a procedure or a patient situation escalates, the educator steps in. That level of hands-on involvement is real and meaningful, but it is categorically different from providing direct care under your own license. The educator is overseeing the learning encounter, not managing the patient assignment independently.
Hospital-based educators occupy a somewhat different position. Nurse educators in clinical development roles, sometimes called clinical nurse educators or nurse professional development specialists, often work on active units and may interact with patients directly while orienting new staff or demonstrating a skill.2 In these hybrid roles, patient contact is a regular part of the work, even if it remains secondary to the teaching function. If you are weighing these two paths, understanding the clinical nurse educator role compared to its academic counterpart can help clarify what daily life actually looks like.
Staffing Shortages and the Floor Pull: A Liability Gray Zone
One scenario worth taking seriously: during acute staffing shortages, some hospitals have pulled nurse educators back to direct patient care to cover floor assignments. Whether this is appropriate depends on several factors, including the educator's current clinical competency, how long they have been out of direct practice, and the institution's own policies. The broader nursing faculty shortage compounds this pressure, as fewer educators means existing staff may be stretched into clinical coverage more often.
This practice raises real scope-of-practice and liability questions. An educator whose role has shifted primarily to classroom or administrative work may not be current on clinical protocols, and neither the educator nor the institution should assume that an active nursing license automatically translates to safe independent practice at the bedside after an extended absence. Nurses considering an educator role in a hospital setting should ask directly about expectations during short staffing and review what indemnification or professional liability coverage applies when they are pulled from their educator duties to the floor.
What the Evidence Suggests
Precise national data on the percentage of nurse educators who engage in direct patient care as part of their role is not currently available in published workforce surveys.1 Reports from organizations such as the American Association of Colleges of Nursing and the National League for Nursing focus primarily on faculty vacancy rates, academic qualifications, and compensation rather than cataloging how frequently educators provide bedside care. What practitioner accounts and institutional descriptions do consistently show is this: academic nurse educators rarely hold patient assignments, while hospital-based educators are far more likely to maintain some form of regular patient contact through their careers in nurse education.3
Questions to Ask Yourself
How Patient Contact Varies by Setting
Classroom teaching versus bedside supervision: these two poles capture most of the variation in patient contact across nurse educator roles. Where you work shapes nearly everything about how often you see patients, what those interactions look like, and whether you carry any direct responsibility for their care.
Academic Faculty in Colleges and Universities
Faculty at nursing schools spend the majority of their time in lecture halls, simulation labs, and faculty offices. Patient contact, if it happens at all, is indirect. It occurs through the students they supervise during clinical rotations, not through personal patient assignments. Some faculty maintain a part-time clinical role to stay current, but that is a personal choice rather than a job requirement. Of the four settings, this one involves the least proximity to patients on a routine basis.
Hospital-Based and Clinical Staff Educators
Staff educators employed by hospitals operate much closer to the floor. For context, bedside nurses in inpatient settings typically spend 60 to 70 percent of their time in direct patient care.1 Staff educators, by contrast, conduct competency checks, orient new hires, and roll out updated protocols, often on the same units where that direct care is being delivered. They may observe nurses at the bedside or step in briefly during a skills demonstration, but they do not carry a patient assignment. Their contact with patients is incidental and observational rather than therapeutic. If you are weighing a clinical nurse educator role against a staff nurse position, this distinction matters.
Clinical Instructors
Of all nurse educator job titles, clinical instructors spend the most time physically near patients. They accompany students into clinical placements at hospitals, clinics, and long-term care facilities, standing close to the bedside while students practice assessments, administer medications, and perform procedures. The instructor does not own the patient assignment, but they must be ready to intervene at any moment for safety reasons. The proximity is real and continuous throughout every clinical shift.
Community Health and Patient Education Roles
Community health educators and hospital-based patient educators land somewhere in the middle. They interact with patients directly, delivering discharge teaching, running wellness classes, or conducting health screenings. The contact is purposeful and face-to-face, but it centers on education rather than clinical intervention. They rarely perform hands-on procedures, and the relationship is time-limited compared to bedside nursing.
The setting you choose is one of the most practical levers you have over how much patient contact remains part of your daily work life as a nurse educator.
Nurse Educator Vs. Patient Educator: Key Differences
The term "nurse educator" gets used loosely, and that creates real confusion. In everyday conversation, someone might call a bedside RN who explains discharge instructions a "nurse educator." But as a career title, those two words point to a very different role with different credentials, a different audience, and a different scope of practice.
What a Patient Educator Actually Does
A patient educator is an RN or a certified health education specialist (CHES) whose primary job is teaching individual patients about their diagnosis, medications, treatment plan, and ongoing self-care. The American Nurses Association identifies patient education as a core nursing function, something every licensed nurse is expected to do regardless of specialty or setting.1 Because it is a foundational nursing competency rather than a separate certification, there is no standalone "RN patient educator" credential. The role lives within the nursing license itself.
The Certified Health Education Specialist credential, awarded by the National Commission for Health Education Credentialing (NCHEC), takes a related but distinct path.2 CHES practitioners may or may not be nurses; their preparation is rooted in public and community health education, and the credential is open to anyone with a bachelor's, master's, or doctoral degree in health education. Their audience is the general public and community populations rather than individual hospital patients alone.
What a Nurse Educator Does
The nurse educator, as a formal career title, teaches nurses and nursing students, not patients. The National League for Nursing (NLN) defines the role through its Core Competencies for Academic Nurse Educators framework, which sets the standard for MSN-prepared faculty working in academic and clinical education programs.3 The ANA echoes this in its guidance on becoming a nurse educator, pointing consistently toward graduate preparation at the MSN or DNP level, with many practitioners also holding the Certified Nurse Educator (CNE) credential.1
The target audience is nursing learners: pre-licensure students in simulation labs, new graduates in hospital orientation, or experienced RNs completing continuing education. If you are curious about what subjects nurse educators teach, the scope ranges from pharmacology and pathophysiology to clinical simulation and leadership.
The Overlap Worth Acknowledging
These roles are not completely separate worlds. Every nurse educates patients; it is woven into practice at every level. And nurse educators, particularly those who maintain clinical hours or work in hospital-based staff development, interact with patient care environments regularly. Understanding the difference between a nurse and a nurse educator helps clarify your path. The distinction is about primary purpose and professional identity, not an absolute wall between the two.
- Patient educator (RN): BSN-prepared, no separate credential required, audience is patients and families.
- CHES: bachelor's-to-doctoral preparation in health education, NCHEC-certified, audience is community populations.
- Nurse educator: MSN or DNP required, often CNE-certified, audience is nursing students and clinical staff.
Knowing where you fall, or where you want to fall, matters when you are choosing a graduate program, targeting a job posting, or explaining your career goals to a hiring committee.
Related Articles
Combining Education and Bedside Nursing: Dual-Role Careers
Many nurses assume they must choose between teaching and clinical practice, but dual-role careers let you do both. These hybrid positions are more common than you might think, and they offer a rewarding way to stay connected to patient care while shaping the next generation of nurses.
One of the most popular dual-role paths is the clinical adjunct instructor position. In this role, you continue working as a bedside nurse (often part-time or per diem) while supervising nursing students during their hospital rotations. You bring real-world expertise into the learning environment, coaching students through assessments, medication administration, and hands-on patient interactions. Because you remain active in practice, your teaching carries the credibility that only current clinical experience can provide.
Another option is the clinical nurse educator role, where you work within a hospital or health system to train staff nurses, orient new hires, and roll out evidence-based practice changes. These educators spend significant time on patient care units, often rounding alongside nurses, troubleshooting complex cases, and modeling best practices at the bedside. While the primary "students" are fellow nurses rather than pre-licensure students, the impact on patient outcomes is direct and measurable.
Some nurse educators negotiate split appointments between a university and a clinical partner. For example, you might teach two courses per semester at a school of nursing while maintaining a 0.5 FTE position as a staff nurse or nurse practitioner in a specialty unit. These arrangements benefit both institutions: the university gains a faculty member with active clinical skills, and the healthcare facility retains an experienced nurse who also mentors students on-site.
If you are drawn to a dual-role career, keep a few practical tips in mind. First, clarify scheduling expectations with both employers early to avoid burnout. Second, pursue certifications (such as the CNE or CNEcl) that validate your teaching competence alongside your clinical credentials. Finally, consider whether nurses teach nurses in your current workplace already. If so, you may already be performing educator functions without the formal title, and formalizing that role could open new career possibilities.
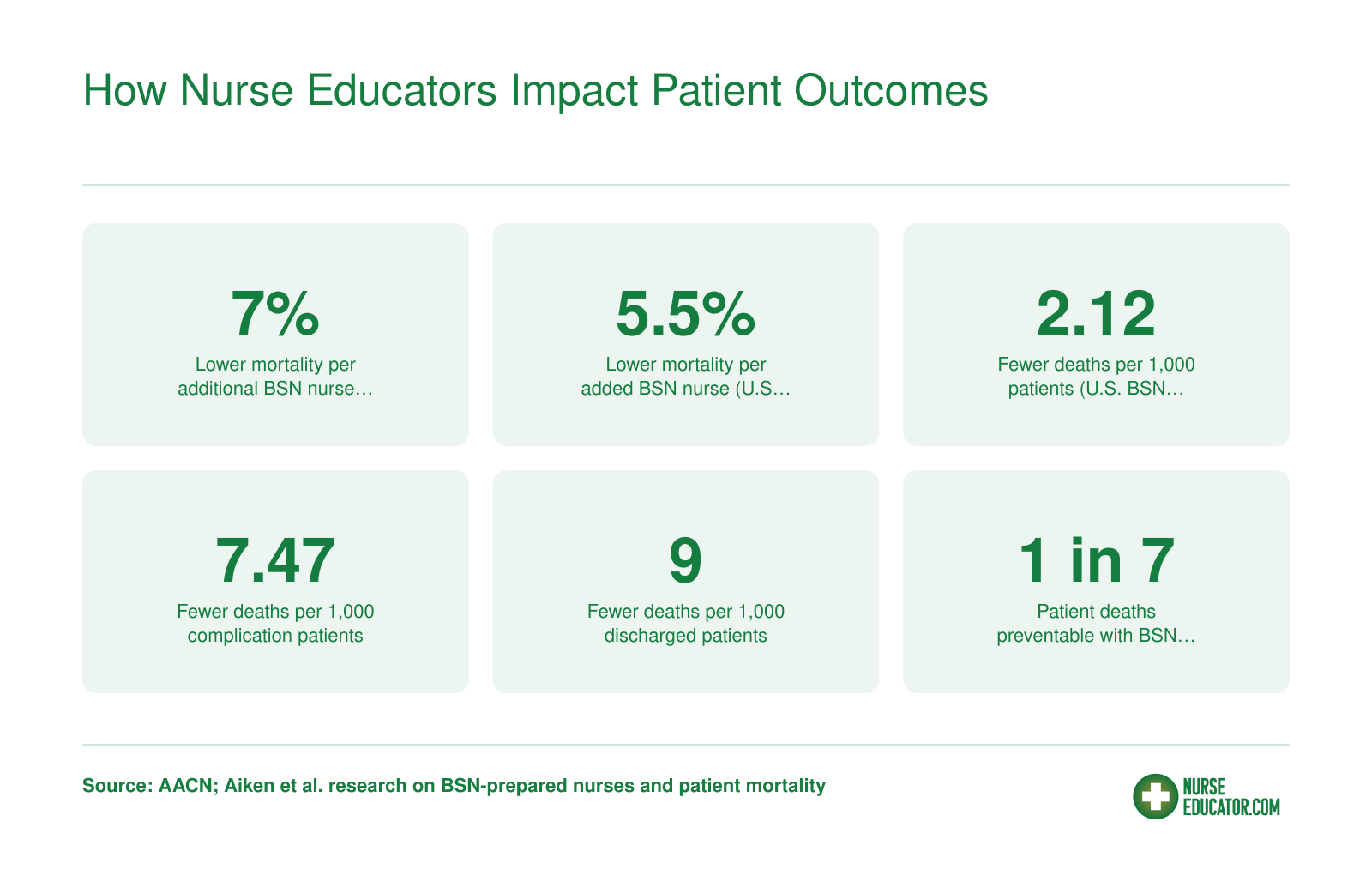
How Nurse Educators Impact Patient Outcomes
Even nurse educators who never touch a patient still shape care quality at scale. The pathway is indirect but powerful: better-prepared educators produce better-prepared nurses, and better-prepared nurses deliver measurably safer care. The statistics below illustrate how investments in nursing education translate into fewer patient deaths and complications.
Maintaining Clinical Skills as a Nurse Educator
Transitioning from bedside to classroom can quietly erode your hands-on proficiency, yet state boards and many employers still expect educators to maintain active clinical competence. The challenge lies in balancing teaching responsibilities with opportunities to practice assessment, intervention, and patient-facing skills in real settings.
Know Your State Board of Nursing Requirements
Every state establishes its own continuing education mandate for RN license renewal, and those rules apply equally to nurse educators. Check your state board of nursing website to confirm the number of CE hours required, the renewal cycle (typically two or three years), and whether any portion must come from hands-on clinical practice. Some states specify minimum direct-care contact hours or simulation-lab credits, while others accept any approved CE without clinical practice stipulations. A few jurisdictions ask only for proof of active employment in nursing, which can include academic teaching, but most do not distinguish between clinical and non-clinical roles when setting baseline CE expectations. Missing these state-specific requirements can stall your license renewal and disrupt both bedside shifts and teaching contracts.
Consult National Standards and Position Statements
The National League for Nursing (NLN) and the American Nurses Credentialing Center (ANCC) publish evolving guidelines on clinical competency for nurse educators. Visit the NLN website for position papers addressing faculty practice and skill currency, and review ANCC resources if you hold or plan to pursue the Nurse Executive or Nursing Professional Development specialty certifications. If you are weighing credential options, comparing CNE vs CNEcl certification can help clarify which path best fits your practice goals. These organizations recommend that educators engage in periodic clinical practice, simulation facilitation, or collaborative partnerships with healthcare facilities to stay current with evidence-based protocols, emerging technologies, and bedside workflows. While neither body enforces a universal clinical-hours mandate, their frameworks influence accreditation standards and employer expectations.
Review Employer and Accreditation Expectations
Job postings from nursing schools often list "recent clinical experience" or "active practice within the past two years" as preferred or required qualifications, especially for faculty teaching clinical courses. Browse openings on the American Association of Colleges of Nursing (AACN) career center and the NLN job board to gauge how programs define clinical currency. Many schools expect educators to work per-diem shifts, participate in faculty practice arrangements, or lead clinical rotations to model competence for students. Accreditation bodies such as the Commission on Collegiate Nursing Education (CCNE) and the Accreditation Commission for Education in Nursing (ACEN) also evaluate whether faculty demonstrate sufficient clinical expertise to teach safely and effectively, making ongoing practice a reputational and compliance issue for your institution.
Strategies to Keep Skills Sharp
Common approaches include picking up per-diem or PRN shifts at a hospital or clinic, serving as a clinical preceptor during student rotations, volunteering at community health events, or maintaining a part-time staff-nurse position alongside teaching duties. Simulation-lab facilitation, high-fidelity manikin programming, and continuing education workshops (especially those offering hands-on skills stations) also help sustain procedural muscle memory. Some educators negotiate faculty practice agreements that reserve a set number of hours each semester for direct patient care, embedding clinical work into their academic contracts. Dispelling nurse educator misconceptions, such as the idea that educators never touch patients, can also help you advocate for protected practice time with your department. The key is consistency: sporadic bedside visits preserve less competence than a regular, predictable practice schedule woven into your calendar.
Nurse Educator Salary and Job Outlook
Nurse educators enjoy strong demand and competitive compensation, though pay differs from bedside nursing roles. The Bureau of Labor Statistics projects a 16.8% growth rate for postsecondary nursing instructors and teachers from 2024 to 2034, well above the average for all occupations. With roughly 91,600 professionals employed nationally as of 2024, expanding nursing programs and faculty shortages are fueling significant hiring activity. Below is a snapshot of how nurse educator earnings compare to registered nurses and nurse practitioners based on BLS May 2023 wage data.
| Occupation | National Median Salary | 25th Percentile | 75th Percentile | Total Employment |
|---|---|---|---|---|
| Nursing Instructors and Teachers, Postsecondary | $79,940 | $62,210 | $102,020 | 74,250 |
| Registered Nurses | $93,600 | $78,610 | $107,960 | 3,282,010 |
| Nurse Practitioners | $129,210 | $109,940 | $149,570 | 307,390 |
Highest-Paying States for Nursing Instructors
Geography plays a significant role in how much nursing instructors and teachers earn at postsecondary institutions. The table below ranks the top 10 highest-paying states by median annual salary, based on the most recent BLS data for the occupation classified as Nursing Instructors and Teachers, Postsecondary. Keep in mind that states with higher pay often carry a higher cost of living, so weigh that factor when evaluating relocation or remote teaching opportunities.
| State | Total Employment | Median Annual Salary | 25th Percentile | 75th Percentile | Mean Annual Salary |
|---|---|---|---|---|---|
| California | 6,120 | $99,010 | $65,510 | $124,290 | $101,770 |
| Texas | 5,940 | $97,610 | $73,670 | $123,360 | $104,640 |
| New York | 5,380 | $93,640 | $63,540 | $128,930 | $99,170 |
| Alaska | 190 | $92,050 | $82,800 | $105,590 | $94,990 |
| Nevada | 920 | $84,660 | $63,070 | $97,040 | $86,640 |
| Montana | 230 | $84,550 | $66,280 | $105,390 | $85,630 |
| Florida | 4,990 | $83,940 | $66,100 | $104,120 | $88,970 |
| Delaware | 250 | $83,420 | $65,190 | $106,410 | $89,730 |
| North Dakota | 120 | $83,130 | $64,360 | $102,080 | $83,460 |
| Connecticut | 1,160 | $81,490 | $63,780 | $101,600 | $93,090 |
Every nurse educator, whether teaching in a classroom or running a hospital skills lab, is directly shaping the quality of care patients will receive tomorrow. Choosing education over bedside practice is not a step away from patient care: it is one of the most far-reaching ways a nurse can influence it.
Frequently Asked Questions About Nurse Educators and Patient Care
These are some of the most common questions nurses ask when exploring how patient interaction fits into a teaching career. Each answer draws on the details covered throughout this article.